
Chronic Tibial Tunnel Infection Following ACL Reconstruction: A Case Report and Review of the Literature
Vol 7 | Issue 1 | January-June 2021 | page: 19-21 | Bishnu Pokharel, Rosan Prasad Shah Kalawar, Ashish Kumar Goyal
Author: Bishnu Pokharel [1], Rosan Prasad Shah Kalawar [1], Ashish Kumar Goyal
[1] Department of Orthopaedics, BPKIHS, Dharan, Nepal. [2] Department of Orthopaedics and Joint Replacement Surgery, Indrparastha Apollo Hospitals, Sarita Vihar, New Delhi, India.
Address of Correspondence
Dr. Ashish Kumar Goyal
Senior Registrar; Department of Orthopaedics and Joint Replacement Surgery Indrparastha Apollo Hospitals, Sarita Vihar, New Delhi, India.
Email: drgoyal41@gmail.com
Abstract
Introduction: Rupture of the anterior cruciate ligament (ACL) is a common injury in active people and one of the most common knee injuries in sports. Foreign body granuloma with concomitant infection is a rare complication in ACL surgery. Very few cases have been reported on it. We present a young patient with a chronic discharging sinus at a surgical site on the tibia in a diabetic patient and its successful management.

Case Report: A thirty-two-year-old male presented to us with a persistent discharging sinus at the surgical site following an Anterior Cruciate Ligament (ACL) reconstruction two years back. Since then, he developed wound infection at the incision site created for graft harvesting, which kept on discharging sero-purulent discharge even with several antibiotics and local dressing courses. There was no stiffness or instability in the knee. We did a follow-up arthroscopic evaluation of the joint and debridement of the wound. A portion of hamstring graft and non-absorbable suture with unhealthy granulation tissues were found subcutaneously during the surgery. A partially resorbed bioscrew with unhealthy granulation tissue was observed in the tibial tunnel. After thorough debridement of the site, the wound completely healed.
Conclusion: Surgical site infection and foreign body granuloma should be considered and treated accordingly if the patient presents with persistent discharging sinus at the surgical site in ACL reconstruction
Keywords: Anterior cruciate ligament reconstruction, ACL, Surgical site infection, Tibial tunnel.
References
1) Miyasaka KC, Daniel D, Stone M, and Hirshman P. The incidence of knee ligament injuries in the general population. Am J Knee Surg. 1991; 4: 3-8.
2) Weiss KS, Weatherall JM, Eick J, and Ross JR. (2017). Delayed Tibial Osteomyelitis after Anterior Cruciate Ligament Reconstruction with Hamstrings Autograft and Bioabsorbable Interference Screw: A Case Report and Review of the Literature. Case Reports in Orthopedics. 2017; 1-7. doi:10.1155/2017/6383526.
3) Barber FA. Complications of Biodegradable Materials. Sports Medicine and Arthroscopy Review. 2015; 23(3):149-155. doi:10.1097/jsa.0000000000000076.
4) Barber FA. Complications of biodegradable materials: anchors and interference screws. Sports Medicine and Arthroscopy Review. 2015;3(3):149–155.
5) Frank M, Schmucker U, David S, et al. Devastating femoral osteomyelitis after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthr. 2008;16: 71–74. https://doi.org/10.1007/s00167-007-0424-7.
6) McAllister DR, Parker RD, Cooper AE, Recht MP, and Abate J. Outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. Am J Sports Med. 1999;27 : 562- 570.
7) Van Tongel A, Stuyck J, Bellemans J, and Vandenneucker H. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: a retrospective analysis of incidence, management and outcome. Am J Sports Med. 2007; 35 : 1059 – 1063.
8) Numazaki H, Kobayashi H, Yoshida K, Hakozaki M, and Konno SI. Prolonged infection at the tibial bone tunnel after anterior cruciate ligament reconstruction. Fukushima J Med Sci. 2017; 63(2):121-125. doi:10.5387/fms.2017-02. 9) O’Neill BJ, Molloy AP, and McCarthy T. Osteomyelitis of the tibia following anterior cruciate ligament reconstruction. International Journal of Surgery Case Reports. 2013;4(2): 143-145. doi: https://doi.org/10.1016/j.ijscr.2012.10.020.
10) Chua CG and Zubair M. A Modified Technique To Treat Infected Tibial Tunnel Post ACL Reconstruction: A Case Report. Malaysian Orthopedic Journal. 2019;13supplA.
| How to Cite this article: Pokharel B, Kalawar RPS, Goyal AK | Chronic Tibial Tunnel Infection Following ACL Reconstruction: A Case Report and Review of The Literature | Trauma International | January-June 2021; 7(1): 19-21. |
(Article Text HTML) (Download PDF)
Acute Scaphoidectomy and Lunocapitate Fusion for the Surgical Treatment of Compound Trans Styloid, Trans-Scaphoid, Peri-Lunate Fracture- Dislocation with Extensor Tendon Injury
Vol 7 | Issue 1 | January-June 2021 | page: 15-18 | Divyesh V. Bukalsaria, Sachin Kale, Prakash D. Samant, Arvind Vatkar, Sanjay Dhar, Prasad Chaudhari
Author: Divyesh V. Bukalsaria [1], Sachin Kale [1], Prakash D. Samant [1], Arvind Vatkar [1], Sanjay Dhar [1], Prasad Chaudhari [1]
[1] Department of Orthopaedic Surgery, D Y Patil Medical College and Research Centre, Navi Mumbai, Maharashtra, India.
Address of Correspondence
Dr. Divyesh Vinod Bukalsaria,
Resident Physician, Department of Orthopaedic Surgery, D Y Patil Medical College and Research Centre, Navi Mumbai, Maharashtra, India.
E-mail: divyeshbukalsaria7@gmail.com
Abstract
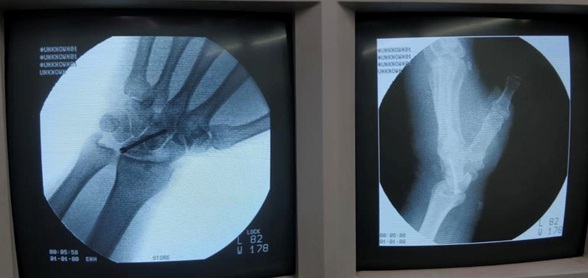
Compound fracture-dislocations of proximal carpal bones are very rare. We report a 54-year-old male, laborer, who sustained a compound Gustilo Anderson type III-A dorsal wound with trans styloid, trans-scaphoid, peri-lunate dislocation with an extensor tendon injury. The patient underwent primary scaphoidectomy with Lunocapitate fusion with extensor tendon repair. On follow-up after 3 months, the patient had partial recovery of range of motion around the wrist without any significant discomfort.
Keywords: Compound fracture-dislocation, Primary proximal row carpectomy, Trans-styloid trans scaphoidperilunate dislocation
References
1. Ali, Nadeem, et al. “Compound Transstyloid, Transscaphoid, Perilunate Fracture Dislocation.” Journal of the Scientific Society, vol. 40, no. 2, 2013, p. 111., doi:10.4103/0974-5009.115485.
2. Herzberg, G., and D. Forissier. “Acute Dorsal Trans-Scaphoid Perilunate Fracture-Dislocations: Medium-Term Results.” Journal of Hand Surgery, vol. 27, no. 6, 2002, pp. 498–502., doi:10.1054/jhsb.2002.0774.
3. Calandruccio, James H., et al. “Capitolunate Arthrodesis with Scaphoid and Triquetrum Excision.” The Journal of Hand Surgery, vol. 25, no. 5, 2000, pp. 824–832., doi:10.1053/jhsu.2000.16364.
4. Oehmke, M. J., et al. “The Blood Supply of the Scaphoid Bone.” Journal of Hand Surgery (European Volume), vol. 34, no. 3, Dec. 2009, pp. 351–357., doi:10.1177/1753193408100117.
5. Mayfield, Jack K. “Patterns of Injury to Carpal Ligaments.” Clinical Orthopaedics and Related Research, & NA; no. 187, 1984, doi:10.1097/00003086-198407000-00006.
6. Herzberg G, Comtet JJ, Linscheid RL, et al. Perilunate dislocations and fracture-dislocations: a multicenter study. J Hand Surg Am.1993;18:768–79.
7. Herzberg, G., and D. Forissier. “Acute Dorsal Trans-Scaphoid Perilunate Fracture-Dislocations: Medium-Term Results.” Journal of Hand Surgery, vol. 27, no. 6, 2002, pp. 498–502., doi:10.1054/jhsb.2002.0774.
8. Herzberg, G., et al. “Perilunate Dislocations and Fracture-Dislocations: A Multicenter Study.” The Journal of Hand Surgery, vol. 18, no. 5, 1993, pp. 768–779., doi:10.1016/0363-5023(93)90041-z.
9. E. Hagert, M. Garcia-Elias, S. Forsgren, B.O. LjungImmunohistochemical analysis of wrist ligament innervation in relation to their structural composition
10. J Hand Surg, 32 (2007), pp. 30-36
11. Moody, Lisa, and Andrew Y. Zhang. “Treatment of an Unusual Trans-Scaphoid Perilunate Avulsion Fracture Dislocation: A Case Report.” Hand, vol. 10, no. 2, Mar. 2014, pp. 328–332., doi:10.1007/s11552-014-9634-x.
12. Sotereanos DG, Mitsionis GJ, Giannakopoulos PN, et al.Perilunate dislocation and fracture-dislocation: a critical analysis of the volar-dorsal approach. J Hand Surg Am. 1997;22:49–56.
13. Yao, Yu-Cheng, et al. “Lunocapitate Fusion with Scaphoid Excision for the Treatment of Scaphoid Nonunion Advanced Collapse or Scapho-Lunate Advanced Collapse Wrist.” Journal of the Chinese Medical Association, vol. 80, no. 2, 2017, pp. 117–120., doi:10.1016/j.jcma.2016.10.001
| How to Cite this article: Bukalsaria DV, Kale S, Samant PD, Vatkar A, Dhar S, Chaudhari P | Acute Scaphoidectomy and Lunocapitate Fusion for the Surgical Treatment of Compound Trans Styloid, Trans-Scaphoid, Peri-Lunate Fracture-Dislocation with Extensor Tendon Injury | Trauma International | January-June 2021; 7(1): 15-18. |
(Article Text HTML) (Download PDF)
Multi-Fragment Patellar Non-Union in a Young Patient Due to Failed Fixation and its Management – A Rare Case Report
Vol 7 | Issue 1 | January-June 2021 | page: 12-14 | Neetin P Mahajan, Prasanna Kumar GS, Pranay Kondewar, Kishor Jadhav
Author: Neetin P Mahajan [1], Prasanna Kumar GS [1], Pranay Kondewar [1], Kishor Jadhav [1]
[1] Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India.
Address of Correspondence
Dr. Prasanna Kumar GS,
Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India.
E-mail: prasannakumargs5@gmail.com
Abstract
Introduction: Multi-fragmentary patellar non-union is rare and it causes functional disability in patients. The purpose of studying this case is to present an unusual patella multi-fragmentary non-union and discuss its management.
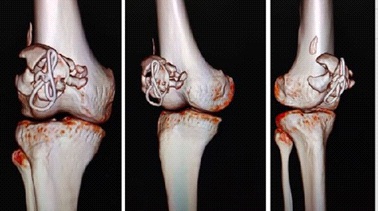
Case presentation: We present a case of a 25-year-old male patient presented with pain and instability and decreased movements of the right knee since last 1 year. The patient had a history of trauma for which he was operated at the local hospital. X-ray and CT scan of the right knee was suggestive of the non-union of the right patella with three main fragments. We managed with open reduction and internal fixation using CC screw, cerclage and tension band wiring. At one-year follow up, the patient is having a clinical and radiological union of non-union with good functional outcome.
Conclusion: Combination of cannulated cancellous screw, cerclage and tension band wiring provides stable fixation in the multi-fragmentary patellar non-union, helps in early mobilisation which in turn helps in getting good functional outcome and prevents implant-related complications.
Keywords: Non-union; Multi-fragmentary patella; Internal fixation; Fixation failure.
References
1. E. J. Eric, “Fractures do joelho,” in Fractures em adultos, R. CAJ, D. P. Green, and R. W. Bucholz, Eds., vol. 1991, pp. 1729–1744, Lippincott, Philadelphia, PA, USA, 3rd edition.
2. Klassen JF, Trousdale RT. Treatment of delayed and nonunion of the patella. J Orthop Trauma. 1997;11(3):188–194.
3. Lachiewicz PF. Treatment of a neglected displaced transverse patella fracture. J Knee Surg. 2008;21:58–61.
4. Satku K, Kumar VP. Surgical management of non-union of neglected fractures of the pa-tella. Injury. 1991;22:108–10.
5. Dhar SA, Mir MR. Use of the Illizarov method to reduce quadriceps lag in the manage-ment of neglected non union of a patellar fracture. J Orthop. 2007;4:12.
6. Nathan ST, Fisher BE, Roberts CS, Giannoudis PV. The management of nonunion and delayed of unionof patella fractures: A systematic review of the literature. Int Orthop. 2011;35:791–5.
7. R. K. Baruah, “Modified Ilizarov in difficult fracture of the patella. A case report,” Jour-nal of Orthopaedic Case Reports, vol. 6, no. 1, pp. 26–28, 2016.
8. C. Gwinner, S. Märdian, P. Schwabe, K. D. Schaser, B. D. Krapohl, and T. M. Jung, “Cur-rent concepts review: fractures of the patella,” GMS Interdisciplinary plastic and recon-structive surgery DGPW, vol. 5, pp. 1–15, 2016.
9. Sutton S, Jr, Thompson C, Lipke J, Kettelkamp D. The effect of patellectomy on knee function. J Bone Joint Surg Am. 1976;58:537–40.
10. Lennox IA, Cobb AG, Knowles J, Bentley G. Knee function after patellectomy a 12- to 48-year follow-up. J Bone Joint Surg Br. 1994;76:485–7.
| How to Cite this article: Mahajan NP, Prasanna Kumar GS, Kondewar P, Jadhav K | Multi-Fragment Patellar Non-Union in a Young Patient Due to Failed Fixation and its Management- A Rare Case Report | Trauma International | January-June 2021; 7(1): 12-14. |
(Article Text HTML) (Download PDF)
Prospective Evaluation of The Results of External Fixation of Unstable Fractures of Distal Radius- A Comparison Between Open and Close Fractures and an Analysis of Similar Studies
Vol 7 | Issue 1 | January-June 2021 | page: 05-11 | Brijesh Sharma, Vipul Agrawal, Rajendra Kumar Shakunt, Chandra Prakash Pal, Mayur Gupta, Rohit Yadav
Author: Brijesh Sharma [1], Vipul Agrawal [1], Rajendra Kumar Shakunt [1], Chandra Prakash Pal [1], Mayur Gupta [1], Rohit Yadav [1]
[1] Department of Orthopaedics, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
Address of Correspondence
Dr. Mayur Gupta,
Department of Orthopaedics, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
E-mail: mayur29.mg@gmail.com
Abstract
Background: Unstable or severely comminuted and intra-articular fractures of distal radius represent traumatic high energy injuries. Prospective study to evaluate the results of external fixation of such fractures was conducted from January 2017 to January 2020 in the Department of Orthopaedics. The aim of this study is to identify the results of external fixation of unstable fractures of distal radius and find out the best treatment options for such fractures under different clinical conditions by comparing the results for open and close fractures and analysis of similar studies.
Materials and Methods: 50 cases of unstable distal radius fractures, including 25 patients with open fractures and 25 patients with close fractures, were treated by external fixation. The patients had mean age of 33 years with 3:2 male female ratio. The fracture was anatomically reduced and fixed with external fixator. The mean follow up was of 24 months.

Results: Final assessment was done at 6 months postoperative follow up using the Sarmiento’s modification of Lindstrom criteria for radiological outcome, showing excellent to good results in 60% cases among open fracture group and 80% cases among close fracture group , Mayo Wrist Score for functional outcome showing excellent to good results in 52% cases among open fracture group and 76% cases among close fracture group. Long term assessment done using Jakim’s scoring system (for clinicoradiological correlation) at 24 months follow-up for all 50 patients, showed excellent to good results in 88% patients. Analysis of similar studies shows external fixation to be the most rewarding treatment option for varied clinical presentations of unstable fractures of distal radius.
Conclusions: Outcome at 6 months is significantly better in close fracture group as compared to open fracture group showing that good soft tissue cover is necessary for functional fracture healing. The long-term outcome in majority of the patients (44 cases) was excellent to good showing reliability of biological ligamentotaxis under various clinical presentations as suggested by analysis of similar studies. This treatment of choice leads to clinically rewarding functional, anatomical and radiological outcomes in unstable distal radius fractures.
Keywords: External fixation, ligamentotaxis, Distal radius.
References
[1] Cooney WP,Linscheid RL,Dobyns JH.External Pin Fixation for Unstable Colles’ Fractures.J Bone Joint Surg. 1979;61-A:840-5.
[2] Chung KC, Watt AJ, Kotsis SV, Margaliot Z, Haase SC, Kim HM (2006) Treatment of unstable distal radial fractures with the volar locking plating system. J Bone Jt Surg Am 88:2687–94
[3] Egol K, Walsh M, Tejwani N, McLaurin T, Wynn C, Paksima N (2008) Bridging external fixation and supplementary Kirschner wire fixation versus volar locked plating for the unstable fractures of the distal radius: a randomised, prospective trial. J Bone Jt Surg 90-A:1214–21
[4] Gouk, C., Ng, S.-K., Knight, M., Bindra, R., & Thomas, M. (2019). Long term outcomes of open reduction internal fixation versus external fixation of distal radius fractures: A meta-analysis. Orthopedic Reviews, 11(3). https://doi.org/10.4081/or.2019.7809
[5] Williksen JH, Husby T, Hellund JC, Kvernmo HD, Rosales C, Frihagen F. External Fixation and Adjuvant Pins Versus Volar Locking Plate Fixation in Unstable Distal Radius Fractures: A Randomized, Controlled Study With a 5-Year Follow-Up. J Hand Surg Am. 2015;40(7):1333-40. doi:10.1016/j.jhsa.2015.03.008
[6] Zhang Li-hai , Wang Ya-nan, Mao Zhi , Zhang Li-cheng, Li Hong-da, Yan Huan , Liu Xiao-xie , Tang Pei-fu . Volar locking plate versus external fixation for the treatment of unstable distal radial fractures: a meta-analysis of randomized controlled trials. J Surg Res. 2015;193(1):324-33. doi:10.1016/j.jss.2014.06.018
[7] Kasapinova K, Kamiloski V. Open reduction and internal fixation versus external fixation and/or kirschner wires for distal radius fractures. A systematic review. Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2014;35(1):225-36. Review. PubMed PMID: 24802315.
[8] Shukla R, Jain RK, Sharma NK, Kumar R. External fixation versus volar locking plate for displaced intra-articular distal radius fractures: a prospective randomized comparative study of the functional outcomes. J Orthop Traumatol 2014;15:265-70.
[9] Gradl G, Wendt M, Mittlmeier T, Kundt G, Jupiter JB. Non-bridging external fixation employing multiplanar K-wires versus volar locked plating for dorsally displaced fractures of the distal radius. Arch Orthop Trauma Surg. 2013;133(5):595-602. doi:10.1007/s00402-013-1698-5
[10] Xuetao Xie, Xiaoxing Xie, Hui Qin, Longxiang Shen & Changqing Zhang (2013) Comparison of internal and external fixation of distal radius fractures, Acta Orthopaedica, 84:3,286-91, DOI: 10.3109/17453674.2013.792029
[11] Esposito J, Schemitsch EH, Saccone M, Sternheim A, Kuzyk PR. External fixation versus open reduction with plate fixation for distal radius fractures: a meta-analysis of randomised controlled trials. Injury. 2013;44(4):409-16. doi:10.1016/j.injury.2012.12.003
[12] Karantana A, Downing ND, Forward DP, Hatton M, Taylor AM, Scammell BE, Moran CG, Davis TR. Surgical treatment of distal radial fractures with a volar locking plate versus conventional percutaneous methods: a randomized controlled trial. J Bone Joint Surg Am. 2013 Oct 2;95(19):1737-44. doi:10.2106/JBJS.L.00232. PubMed PMID: 24088965.
[13] Walenkamp MM, Bentohami A, Beerekamp MS, Peters RW, vander Heiden R, Goslings JC, Schep NW (2013) Functional outcome in patients with unstable distal radius fractures, volar locking plate versus external fixation: a meta-analysis. Strategies Trauma Limb Reconstruction 8(2):67–75
[14] Wei DH, Raizman NM, Bottino CJ, Jobin CM, Strauch RJ, Rosenwasser MP (2009) Unstable distal radial fractures treated with external fixation, a radial column plate, or a volar plate. J Bone Jt Surg 91-A:1568–77
[15] H J Kreder, D P Hanel, J Agel, M McKee, E H Schemitsch, T E Trumble, D Stephen.Indirect reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular fractures of the distal radius: a randomised, controlled trial. J Bone Joint Surg Br 2005;87:829-36.
[16] Margaliot Z, Haase SC, Kotsis SV, Kim HM, Chung KC. A meta-analysis of outcomes of external fixation versus plate osteosynthesis for unstable distal radius fractures. J Hand Surg Am. 2005;30(6):1185-99. doi:10.1016/j.jhsa.2005.08.009
[17] Handoll HH, Madhok R. Surgical interventions for treating distal radial fractures in adults. Cochrane Database SystRev 2003:CD003209.
[18] Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002;84:1093–110.
[19] Zollinger PE, Tuinebreijer WE, Breederveld RS, Kreis RW. Can vitamin C prevent complex regional pain syndrome in patients with wrist fractures? A randomized, controlled, multicenter dose-response study. J Bone Joint Surg Am. 2007;89(7):1424-31. doi:10.2106/JBJS.F.01147
[20] Navarro CM, Pettersson HJ, Enocson A. Complications after distal radius fracture surgery: results from a Swedish Nationwide Registry study. J Orthop Trauma. 2015;29(2):E36-42.
| How to Cite this article: Sharma B, Agrawal V, Shakunt RK, Pal CP, Gupta M, Yadav R | Prospective Evaluation of The Results of External Fixation of Unstable Fractures of Distal Radius- A Comparison Between Open and Close Fractures and an Analysis of Similar Studies | Trauma International | January-June 2021; 7(1): 05-11. |
(Article Text HTML) (Download PDF)
To Evaluate The Outcome of Proximal Femoral Nail A2 in Management of Inter-trochanteric Fractures of Femur in Elderly
Vol 7 | Issue 1 | January-June 2021 | page: 01-04 | Karuna Shankar Dinkar, Rohit Yadav, Arjun Uppal, Chandra Prakash Pal, Mayur Gupta
Author: Karuna Shankar Dinkar [1], Rohit Yadav [1], Arjun Uppal [1], Chandra Prakash Pal [1], Mayur Gupta [1]
[1] Department of Orthopaedic Surgery, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
Address of Correspondence
Dr. Chandra Prakash Pal,
Professor and Head Dept. of orthopedics, S. N. Medical College, Agra, Uttar Pradesh, India.
E-mail: drcportho@gmail.com
Abstract
Introduction- The incidence of inter-trochanteric fracture in the elderly is rising because of increased age and with low bone mineral density. The presence of osteoporosis in inter-trochanteric fractures is important because the fixation of the proximal fragment depends entirely on the quality of the cancellous bone present. The surgical stabilization of inter-trochanteric fractures remains a persistent challenge. The purpose of this study is to study the effectiveness and drawbacks of one such newer intramedullary device, Proximal Femoral Nail Antirotation in the management of inter-trochanteric fractures.
Material and method- Patients who underwent PFNA for inter-trochanteric fractures at a tertiary care center Agra, who have given written and informed consent. Patients fitting into inclusion criteria would form the study group. Data collected by interviews, observation of clinical and radiological findings and assessment of function done using Harris hip score.
 Results- The study comprised 24 patients, with a mean age of mean age 63 years who suffered fracture inter-trochanteric femur, due to either trivial fall (75%) or RTA (17%) and managed by cephalomedullary nailing using Proximal Femoral Nai Antirotation at our center. The majority of the patients had the quality of reduction; the Majority of patients took 12 to 22 weeks for union with mean union time of 14 weeks. Patients were asked to follow up routinely, with post-operative follow up ranging from a minimum of 11 months to 18 months. At the final follow up following results obtained according to Harris Hip Score, were 55% patients excellent, 30.50% patients good, 12% patients fair, 2.50% patients poor.
Results- The study comprised 24 patients, with a mean age of mean age 63 years who suffered fracture inter-trochanteric femur, due to either trivial fall (75%) or RTA (17%) and managed by cephalomedullary nailing using Proximal Femoral Nai Antirotation at our center. The majority of the patients had the quality of reduction; the Majority of patients took 12 to 22 weeks for union with mean union time of 14 weeks. Patients were asked to follow up routinely, with post-operative follow up ranging from a minimum of 11 months to 18 months. At the final follow up following results obtained according to Harris Hip Score, were 55% patients excellent, 30.50% patients good, 12% patients fair, 2.50% patients poor.
Conclusions- The inter-trochanteric fracture in elderly patients treated with cephalomedullary nailing using proximal femoral nail-anti-rotation, which has the biomechanical advantage of the helical blade providing bone compaction, increasing surface area and better anchorage in the femoral head, which showed favorable outcome by retarding rotation and varus collapse and prevents medialization by acting as a central pillar.
Keywords- Inter-trochanteric fractures; Proximal femoral nail A2; Harris Hip Score.
References
1. Kaufer H. Mechanics of the Treatment of Hip Injuries. Clin Orthop. 1980;146:53 -61.
2. Kyle RF, Gustilo RB, Premer RF. Analysis of six hundred and twenty – two intertrochanteric hip fractures. A retrospective and prospective study. J Bone Joint Surg. 1979;61A: 216 – 21.
3. Kaufer H, Mathews LS, Sonstegard D. Stable Fixation of Intertrochanteric Fractures. J Bone Joint Surg. 1974;56A:899 – 907.
4. Sommers MB, Roth C, Hall H, Kam BC, Ehmke LW, Krieg JC,et al. A laboratory model to evaluate cutout resistance ofimplants.
5. Sadic S et al. Proximal Femoral Nail Antirotation in Treatment of Intertrochanteric Hip Fractures:a Retrospective Study in 113 Patients Med Arh. 2015 Dec; 69(6): 353-356.
6. Jin-Song Pu & Lei Liu & Guang-Lin Wang & Yue Fang & Tian-Fu Yang Results of the proximal femoral nail anti-rotation (PFNA) in elderly Chinese patients International Orthopaedics (SICOT) (2009) 33:1441–1444 DOI 10.1007/s00264-009-0776-3.
7. Chaoliang Lv, MD;Yue Fang, MS; Guanglin Wang,MD; Tianfu Yang, BS; Hui Zhang, MD; Yueming Song,MD. The New Proximal Femoral Nail Antirotation Asia: Early Results. Orthopaedics:10.3928/1477447-20110317-26
8. Sahin S, Ertürer E, Oztürk I, Toker S, Seçkin F, Akman S. Radiographic and functional results of osteosynthesis using the proximal femoral nail antirotation (PFNA) in the treatment of unstable intertrochanteric femoral fractures. Acta Orthop Traumatol Turc. 2010;44(2):127-34. doi: 10.3944/AOTT.2010.2237.for pertrochanteric fracture fixation. J OrthopTrauma. 2004;18(6):361–8.5
9. Kumar GN et al. Treatment of Unstable Intertrochanteric Fractureswith Proximal Femoral Nail Antirotation II: Our Experience in Indian Patients the Open Orthopaedics Journal, 2015, 9, 456-459
10. Jacobs RR, McClain O, Armstrong H J. Internal fixation of intertrochanteric hip fractures: a clinical and biomechanical study. Clin Orthop. 1980; 146:62 –70.
11. Simpson AH, Vart y K, Dodd C A. Sliding hip screws: modes of failure. Injury. 1989;20:227 – 31.
| How to Cite this article: Dinkar KS, Yadav R, Uppal A, Pal CP, Gupta M | To Evaluate The Outcome of Proximal Femoral Nail A2 in Management of Inter-trochanteric Fractures of Femur in Elderly | Trauma International | Jauary-June 2021; 7(1): 01-04. |
(Article Text HTML) (Download PDF)
LICENSE
![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X