
Where Do We Need More than One Approach for Acetabular Fractures and Which One First?
Vol 3 | Issue 1 | Jan – Apr 2017 | page:10-13 | Raju Vaishya, Vipul Vijay, Amit K Agarwal, Abhishek Vaish
Author: Raju Vaishya [1], Vipul Vijay [1], Amit K Agarwal [1], Abhishek Vaish [2]
[1] Department of Orthopaedics and Joint Replacement Surgery, Indraprastha Apollo Hospitals, New Delhi, India,
[2] Department of Orthopaedics, Canterbury Christ Church University, Kent, UK.
Address of Correspondence
Dr. Raju Vaishya,
Indraprastha Apollo Hospitals, New Delhi, India.
E-mail: raju.vaishya@gmail.com
Abstract
Acetabular fractures are often difficult to manage. The majority of fractures require anatomical reduction to prevent secondary
osteoarthritis and instability. Often a single approach is sufficient to fix these fractures. The choice of approach depends on the
major anatomical involvement of the acetabulum. However, some fracture patterns require more than a single approach to fixing the
fractured fragments adequately. This article addresses this particular issue.
Keywords: Acetabulum, fractures, pelvic, surgical approaches.
What to Learn from this Article?
The fixation of all the acetabular fractures cannot be achieved with a single approach, at all the times. Hence, it is necessary to do a good pre-operative planning and identify the fractures which may require a dual approach to achieve satisfactory fixation.
Introduction
The iPhone App Store was launched in July 2008 and was followed by the Google Play store in 2012. The above ones are the most popular mobile operating sys-tem in the world till date. The mobile apps have changed our lives and the way we com-municate with each other and go about doing things. So is the world of Medical and Orthopaedic Apps which have been on the forefront since last few years.
Here we present you a series of review of few Medical Apps which we regularly use and make a difference in our lives and the way we practice Orthopaedics and increase productivity.
Review
The basic fracture fixation principles in the lower extremity are anatomical reduction and the possibility of early rehabilitation. A combination of these two factors can help one achieve good prognosis and outcomes. The acetabular fractures are no different. They should be managed aggressively, and an attempt should be made to achieve anatomical reduction so as to prevent the most common complication of osteoarthritis (1). There are some restrictions on the surgical management of acetabulum fractures which may influence the decision of the treating surgeon towards an operative or conservative treatment. Factors like the proximity to important anatomical structures, the difficulty in achieving surgical exposure and the lack of experience in managing these fractures, all influence the decision-making (1).
With advances in imaging technology, a better understanding of anatomy and improved approaches for the management of the acetabulum fractures; focus is shifting towards an effort to achieve anatomical reduction (2). The first step in achieving anatomical reduction for any fracture is good surgical exposure. The most commonly used approaches are the Kocher Langenback and ilioinguinal approach, which have been the workhorse for acetabular surgeons. Recently, further modifications and some extensile approaches like iliofemoral, Stoppa’s, trochanteric osteotomy, etc have also been introduced (3-8). The type and combination of the surgical approach to be used is of paramount importance in achieving a good outcome.
Limitations of a Single Approach
The first step is to understand the anatomy, displacement and the direction of displacement of the fracture. The second step is to plan an approach which would allow proper visualization and accurate reduction of the fracture fragments (2). The ilioinguinal approach is useful for fixation of the anterior column and wall fractures, but they are unable to help in achieving an accurate reduction in cases of displaced posterior column fractures (1) (Figure 1). Similarly, the Kocher-Langenback approach can be used for good visualization of the posterior column and wall fractures, but they provide inadequate exposure to the anterior column and wall (1) (Figure 2).

Matta emphasized the need for anatomical reduction of the fracture fragments in acetabulum for optimal results (9). The key to anatomical reduction is good exposure and visualization of the fracture fragments. A single approach can adequately manage fractures involving a single column or wall. Also, certain bicolumnar fractures which have minimal displacement in one of the columns can also be managed by approaching the more displaced column directly.
However, in certain fractures like T-type fractures with significant displacement in both columns cannot be managed with a single approach. They require either the use of the described extensile approaches like iliofemoral, tri-radiate, etc. or the use of sequential approaches. These approaches are not without their sets of complications like increased rates of infection, delayed rehabilitation, higher rates of ectopic ossification and prolonged abductor weakness (2). Hence, whenever an extensile or a sequential approach is planned, the decision should be based on sound scientific judgement.
Fractures which can not be accessed through K-L approach alone
1. Both columns fractures
2. Anterior column fractures
3. Anterior column and posterior Hemi transverse fracture
Fractures which can not be accessed through ilioinguinal approach alone
1. T-type fractures
2. Isolated posterior column fractures
Fractures needing more than one approach
The fractures which may require more than one approach for an optimal result include –
1. T-type fractures
2. Selected both column fractures with significant displacement (>10mm) in both the columns.
3. Transtectal transverse fractures
4. Transverse fractures with posterior wall fracture with wide displacement
T-type and complete both column fractures
The T-type fractures and complete both column fractures need special mention. In these types of fractures, the femoral head is displaced medially, and both the columns rotate around the femoral head in opposite directions. This mechanism of rotation of the two columns can be understood as one similar to the two doors of a gate opening up in opposite direction around a central hinge. Any attempt at indirect reduction of the columns in these types of fractures will only lead to maintenance of the malrotation and the persistence of inaccurate reduction (1). These fractures are an absolute indication for open reduction, direct visualization, and internal fixation. Hence, these fractures may sometimes require the use of extensile approach or two sequential approaches for optimal fixation (2).
Transtectal fractures which have an anterior displacement also may require sequential approaches for fixation of these fractures. Some of the transtectal fractures may be fixed using a single anterior or posterior approach, especially if they have isolated posterior displacement. Some fractures with high anterior obliquity, on Judet views, with minimal displacement may also be fixed with an isolated posterior approach. Fractures with large displacement (>10 mm) in the anterior direction, usually need sequential surgical approaches (10).
In the transtectal fractures, the vertical nature of the fracture line makes it difficult to palpate the reduction through the greater sciatic notch (11). Moreover, since the fracture line passes through the supra-acetabular dome, imperfect reductions are very poorly tolerated (11). An adequate fixation may require in some of these fractures to utilize two approaches.
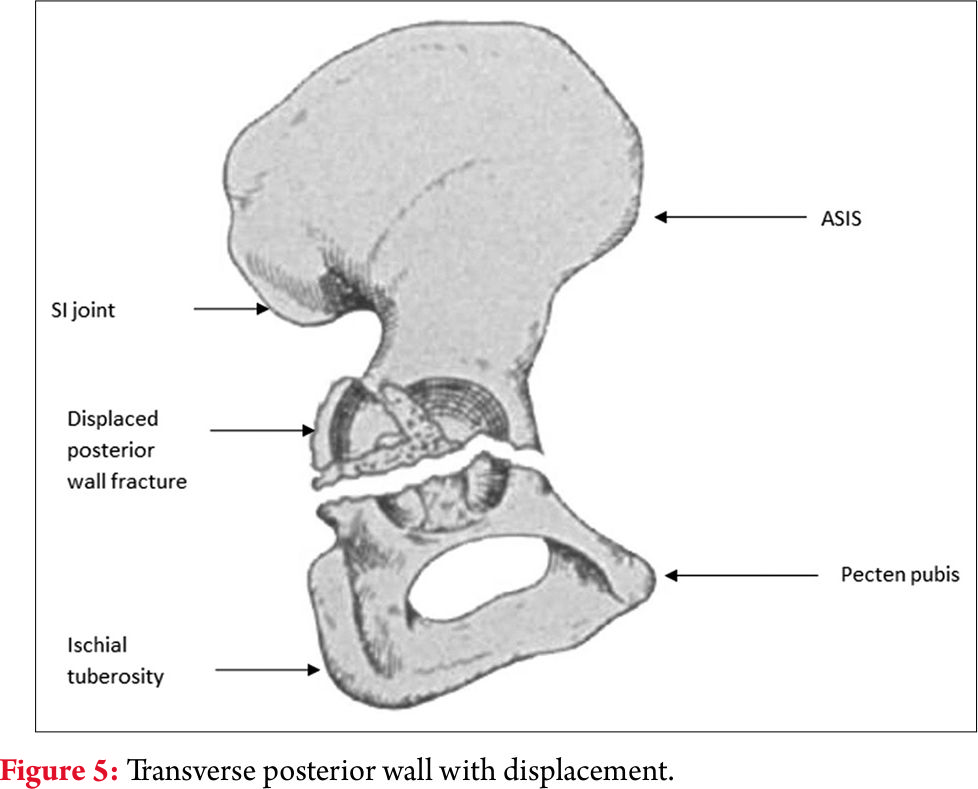
Transverse plus posterior wall fractures may make it difficult to be fixed through the isolated anterior approach. If approached through the K-L approach alone, the reduction of the transverse fractures may be difficult to assess through the posterior wall window, even after femoral head distraction. This may make it useful that the surgeon fixes the posterior wall using the K-L approach and then use the ilioinguinal approach for fixation and assessment of the transverse fracture reduction and fixation (1).

Decision making
The decision making for the choice of effective approach depends on the pre-operative CT scan (10). The first choice of fixation of the fractures mentioned is the Kocher-Langenback approach in preferably prone or lateral decubitus position. The pre-operative CT scan should be assessed and if there is a vertical fracture pattern or greater anterior displacement, then it would not be amenable to fixation through the isolated posterior approach but would require an additional anterior approach for optimal fixation (1,10).
Which approach first?
The decision of the first approach to be used depends on various factors. The amount of communication in one of the columns is one of the major determinants. The column which has a greater amount of communition should be fixed first. In the presence of a dislocation, the approach which gives direct access to the side of dislocation should be approached first. In case both the columns have equal comminution or are equally displaced, most of the surgeons prefer making the posterior approach first in the prone or the floppy lateral position (2). The anterior approach is made after making the patient supine.
The T-type fractures are a special case in the combined approach. It is often impossible to fix the posterior column through the K-L approach, without the screws passing through the anterior column fractures (11). Thus, the fractures of the anterior column must be reduced first, which makes the subsequent reduction of the posterior column and wall more amenable.
There have been some studies in the recent English literature, which have used the simultaneous anterior and the posterior approaches by two surgical teams (2). The advantages of simultaneous anterior and posterior approaches are decreased surgical time and simultaneous assessment of the reduction from anterior as well as the posterior directions. The disadvantages of this simultaneous approach are the requirement of two surgical teams which are equally adept and versed with acetabular fractures (2). Also, the anterior exposure is a bit difficult in the floppy lateral position, and the exposure is tough in obese patients (2).
Disadvantages
The disadvantages with the use of simultaneous or sequential approaches for acetabular fixation are –
1. Increased blood loss
2. Increased morbidity
3. Increased incidence of heterotopic ossification – due to increased soft tissue manipulation
4. Increased surgical time
Literature review
Combined exposures of the acetabulum have been used in the literature. Matta reported a very low incidence of 2% out of a total of 262 fractures operated (12). Letournel used a sequentially combined approach in only 3% of the cases, out of a total of 849 cases (3). Similarly, Mayo reported an incidence of 4% for combined approaches in their series of the acetabulum fractures (13).
The most important aim in acetabular fractures is anatomical reduction and adequate fixation. Even though all these studies emphasize that the number of fractures requiring more than one approach be limited, surgeon awareness is important so that an inaccurate reduction is not accepted. Adequate pre-operative planning using all the possible radiographic views and the CT scans available should be done, so that the surgeon is aware of the possibility of using two approaches based on the type of fracture and the displacement. This information can help the surgeon as well his team, including anaesthetists and assistants, be aware and prepared for the same.
The decision regarding whether the approach is made simultaneous or sequential and under the same or different anaesthesia, should be taken by surgeon expertise and OT backup. In most scenarios, the column with more comminution should be approached first and in the setting of equal comminution, the posterior column should be approached first.
References
1. Matta JM. Operative indications and choice of surgical approach for fractures of the acetabulum. Techniques Orthopaed 1986;1(1):13-22.
2. Harris AM, Althausen P, Kellam JF, Bosse MJ. Simultaneous anterior and posterior approaches for complex acetabular fractures. J Orthop Trauma. 2008 Aug;22(7):494-7.
3. Letournel E, Judet R, eds. Fractures of the Acetabulum. 2nd ed. Berlin, Germany: Springer-Verlag; 1993.
4. Mears DC, Rubash HE. Extensile exposures of the pelvis. Contemp Orthop. 1983;6:21–32.
5. Reinert CM, Bosse MJ, Poka A, et al. A modified extensile exposure for the treatment of complex or malunited acetabular fractures. J Bone Joint Surg. 1988;70A:329–337.
6. Routt ML Jr, Swiontkowski MF. Operative treatment of complex acetabular fractures. Combined anterior and posterior exposures during the same procedure. J Bone Joint Surg Am. 1990;72:897–904.
7. Griffin DB, BeaulA ˜ PE, Matta JM. Safety and efficacy of the extended iliofemoral approach in the treatment of complex fractures of the
acetabulum. J Bone Joint Surg Br. 2005;87:1391–1396.
8. Wey J, DiPasquale D, Levitt L, et al. Operative treatment of acetabular fractures through the extensile Henry approach. J Trauma. 1999;46: 255–260.
9. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients operatively treated within three weeks after injury. J Bone Joint Surg. 1996;78A:1632–1644.
10. Bogdan Y, Dwivedi S, Tornetta P 3rd. A surgical approach algorithm for transverse posterior wall fractures aids in reduction quality. Clin Orthop Relat Res. 2014 Nov;472(11):3338-44.
11. Bucholz RW, Heckman JD, Court-Brown C, eds. Rockwood Green’s Fractures in adults. 6th edn. New York, USA: Lipincott William & Wilkin’s;2006.
12. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients operatively treated within three weeks after injury. J Bone Joint Surg. 1996;78A:1632–1644.
13. Mayo KA. Open reduction and internal fixation of fractures of the acetabulum: results in 163 fractures. Clin Orthop. 1994;305:31–37.
| How to Cite this article: Vaishya R, Vijay V, Agarwal AK, Vaish A. Where Do We Need More Than One Approach for Acetabular Fractures and Which One First? Trauma International Jan-Apr 2017;3(1):10-13. . |
