
Understanding Clinical Radiology of Fracture Acetabulum
Vol 2 | Issue 2 | May – Aug 2016 | page:9-16 | U K Sadhoo
Author: U K Sadhoo [1]
[1] Nayati Hospital, Mathura, U.P. 281003
Address of Correspondence
Dr. U K Sadhoo
Nayati Hospital, Mathura, U.P. 281003
Email: uksadhoo@yahoo.com
Abstract
Acetabulum is one of the most anatomically complex regions of the body. Fractures in this area are difficult to visualise due to complex anatomy and overlaping of radiological shadows. Plain radiology od acetabular and pelvis fractures require detailied understanding of the imaging techniques and anatomy. Newer advances like 3-D CT etc have added new dimensions to the radiological assessment of acetabular fractures. Current review focusses on basic radiological principles to help the readers understand and categorised acetabulam fractures an also plan the surgical intervention.
Keywords: Acetabular fractures, radiological asessement, CT Scan.
Introduction
Acetabulum is a major weight-bearing joint, connecting Axial skeleton to lower limbs. Therefore a fracture of Acetabulum has implications for the mobility and disability for rest of life. Until the pioneering work of Judet and Letournal (1), these injuries were poorly understood and inadequately treated. Now this sub-specialty has come of age. The difficulty in understanding the nature of these injuries is the complex shape of Pelvis anatomy. Radiology not only provides an accurate assessment, it also gives a pointer to the approach and definitive treatment. Judet and Letournal classification is based on the lines produced by xray beams on the cortical surfaces in AP and two 45 degree oblique projections. Though advent of CT has enhanced our understanding, this classification remains the de facto standard. The other classifications are AO/OTA classification and the CT based Harris et al classification (3,4)
Anatomy
Acetabulum is formed by confluence of Ilium, Ischium and Pubis into an inverted horse-shoe shaped structure that is deficient inferiorly, bridged by Transverse Acetabular Ligament. The central non-articular part is known as cotyloid fossa which houses fat (Pulvinar) and Ligamentum Teres (Fig 1). Bony Acetabulum has inclination of 55-60 degrees to horizontal. This is deepened by Labrum, a soft fibro-cartilagenous structure not unlike meniscus. This increases the load-sharing area and provides additional check against dislocation.

Radiology
X-rays (Fig. 3):
Look for 6 landmarks :
1. Post. Wall : Lateral-most projection on AP and Obturator view x-ray. Seen clearly because of anteverted Acetabulum.
2. Ant. Wall : Superimposed on post. Wall, still visible as undulation line on good quality x-ray.
3. Dome : weight-bearing area of acetabulum.
3 variants :
TransTectal : through weight-bearing area
Juxta Tectal : at roof of cotyloid fossa where it joins articular area
Infra Tectal : Through floor Cotyloid fossa. Juxta and infra-Tectal don’t involve weight bearing surfaces so rarely need operative measures.
4. Tear Drop : Not an anatomical structure. Seen on AP projection. Lateral wall represents inferior-most Acetabulum articular surface, medial boundary by Quadrilateral plate.
5. Ilio-Ischial line : representing Posterior column
6. Ilio-Pectineal line : representing Anterior column
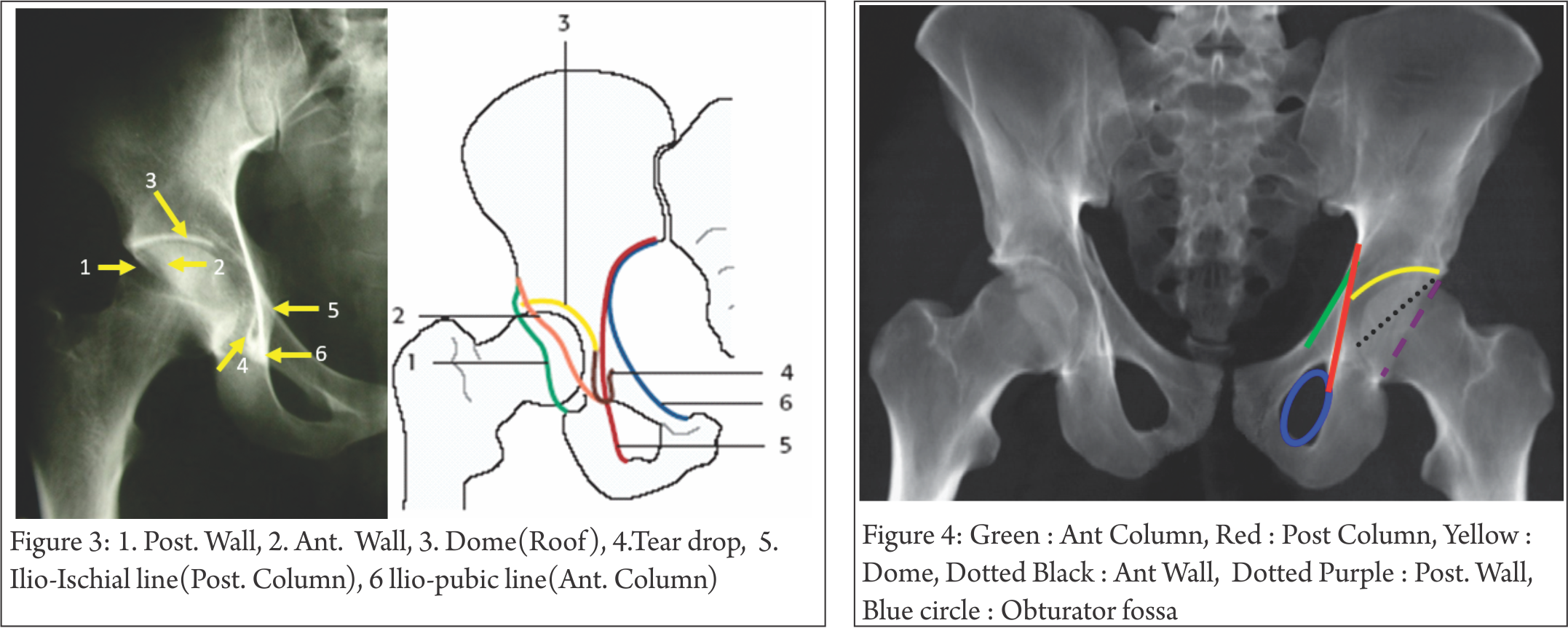
AP View 1-minute assessment (Fig. 4) : Basic, quick, cheap investigation. Look at 4 lines, 1 curve, 1 circle; it gives lot of information, enough to make a considered decision about the severity of injury and urgency of treatment. It may not pick up subtle fractures, small intra-articular fragments, marginal impaction. There is virtually nil to be deduced from x-ray about the soft tissue component of injury.
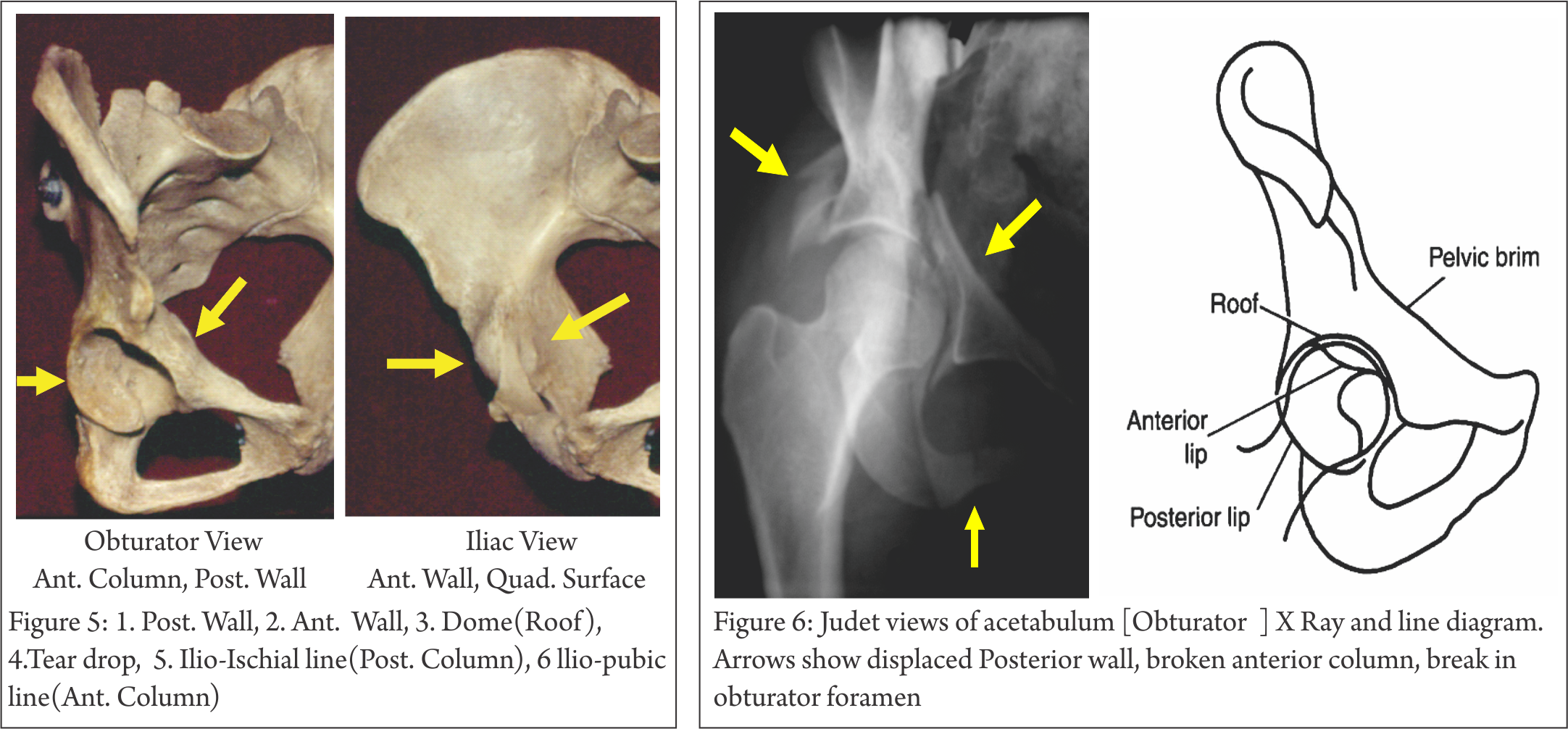
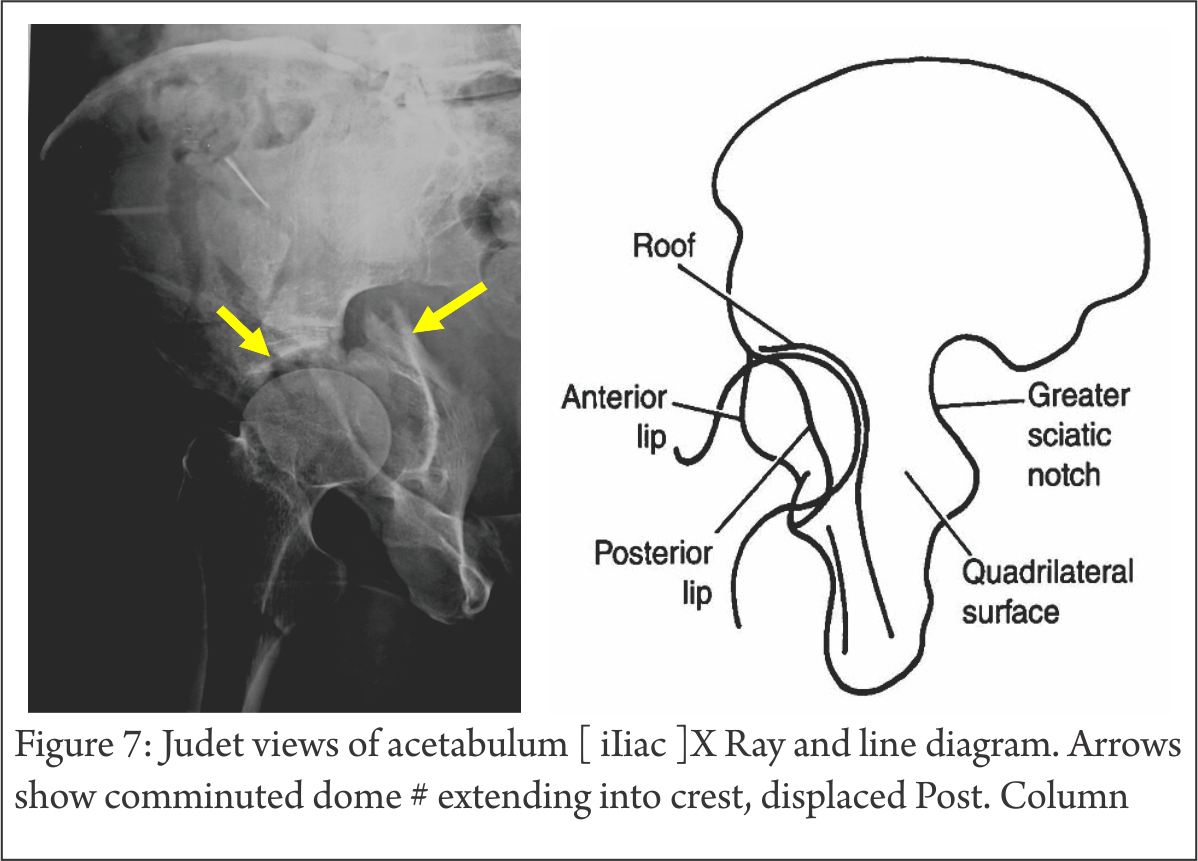
Judet Views (Fig. 5,6,7) : Patient is tilted 45 degree to horizontal, once with injured side up, then normal side up, at right angle to each other. The x ray beam is perpendicular to Horizontal, focused on affected hip in both views.
Obturator : shows Iliac wing seen end-on, Obturator foramen in full profile. (highlights Anterior column, Posterior Wall)
Iliac : shows Iliac blade, Posterior column, Ant. wall (most lateral projection), Sciatic notch, Quadrilateral plate.
Sometimes, it is not possible to do Judet views because of patient discomfort. In such cases, angiographic C-arm can be tilted, instead of the patient, to gain necessary information (7).
Planar CT scan (Fig 8,9,10) : Thin-slice scans, axial, coronal and sagittal, are invaluable tool for complete evaluation of Acetabulum fractures. It can show marginal impaction, intra-articular fragments, subtle fracture lines, and posterior Sacro-Iliac injury. It thus complements the information gained on x-rays. In addition, soft tissue injury like Morell-Lavalle lesion can be picked up on CT (or MRI).

3D CT (Fig.11): It is a reformatted image from thin sections into 3D surface-rendered images. These images are easy to understand, easy to manipulate in any direction, with or without femoral head in acetabulum. No doubt finer details like intra-articular bone pieces, impaction, and fine fracture lines are lost but it remains a powerful tool to have a bird’s eye-view of a very complex anatomy and injury. One major advantage is the ability to process data into reformatted images (Fig.12) to appear as planar AP or Judet views without the need to move or tilt the patient (5).

CT can show fracture in coronal or sagittal planes; it can also be used with artefact-suppression software for post–op evaluation of adequacy of reduction, intra-articular metal or loose bone pieces (Fig 13). The fracture lines through the Dome need understanding to interpret the diagnosis correctly (Fig 14).
Proximal 10mm of Axial CT also corresponds to the weight-bearing Dome (6). Therefore, if a fracture does not involve the proximal 10mm of Acetabulum, conservative treatment is indicated.

Judet and Letournal Classification:
Before discussing Classification, it is important to keep the following points in mind:
-Fractures are described with respect to a lateral-facing Acetabulum (Fig 1). This is quite different from real-life situation in which Acetabulum is tilted anteriorly and inferiorly. Therefore, a Transverse fracture orients in oblique-sagittal plane in a Pelvis-AP x-ray than a horizontal line.
-Walls are part of the column (Fig 2). Therefore, it is possible to break either wall or column or both simultaneously. For a column to break, exit line is through Obturator oval in most, but not all, cases. Add to this, part or complete Transverse # element and many possibilities emerge.

10 fracture patterns are recognized (fig. 15, 16); 5 elementary and 5 associated which are combination of one or more of elementary pattern. All of them are based on the walls getting separated from columns and columns getting broken at Sciatic buttress, with transversely oriented fracture through Acetabulum completing the picture.

5 elementary types are Anterior Wall, Anterior Column, Posterior Wall, Posterior Column and Transverse fracture (Fig. 15).
5 Associated patterns (Fig. 16), as name suggests, are combination of two or more Elementary patterns. These are: Posterior wall and Column fracture, Transverse with Post Wall, T Shaped, Ant Wall/Column with Posterior Hemi-transverse and associated both column. Not every fracture can be pigeon-holed in these 10 patterns, but it is as good a working classification as any.
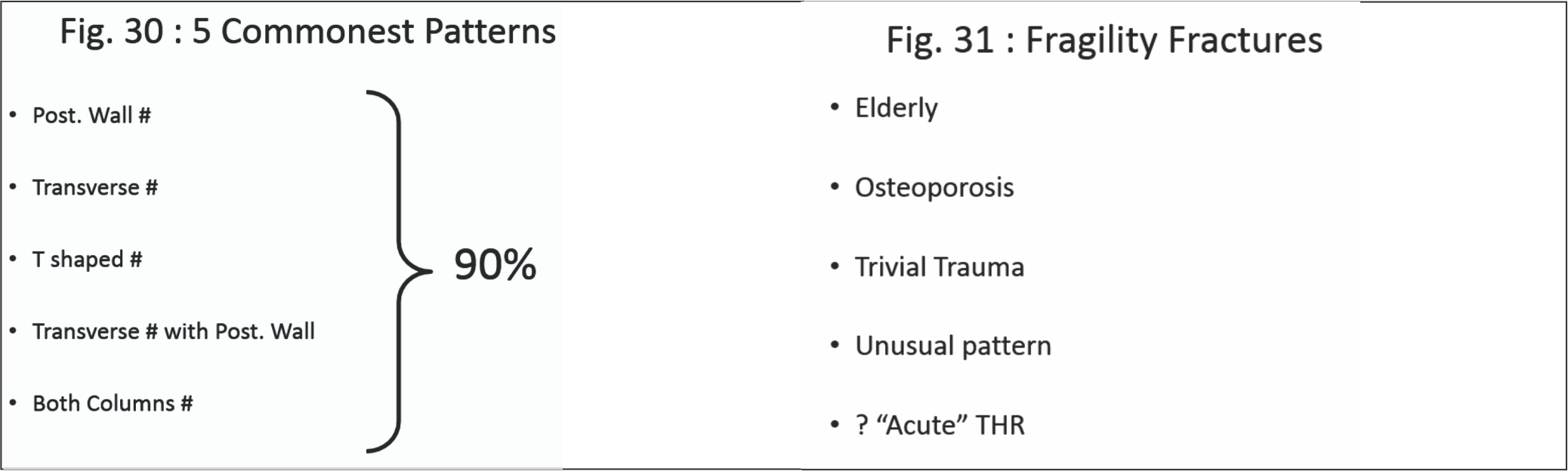
5 patterns of these 10 constitute 80% of all Acetabulum fractures: Post Wall, Transverse, Transverse with Post wall, T shaped and Both Columns (Fig. 30).(5,6)
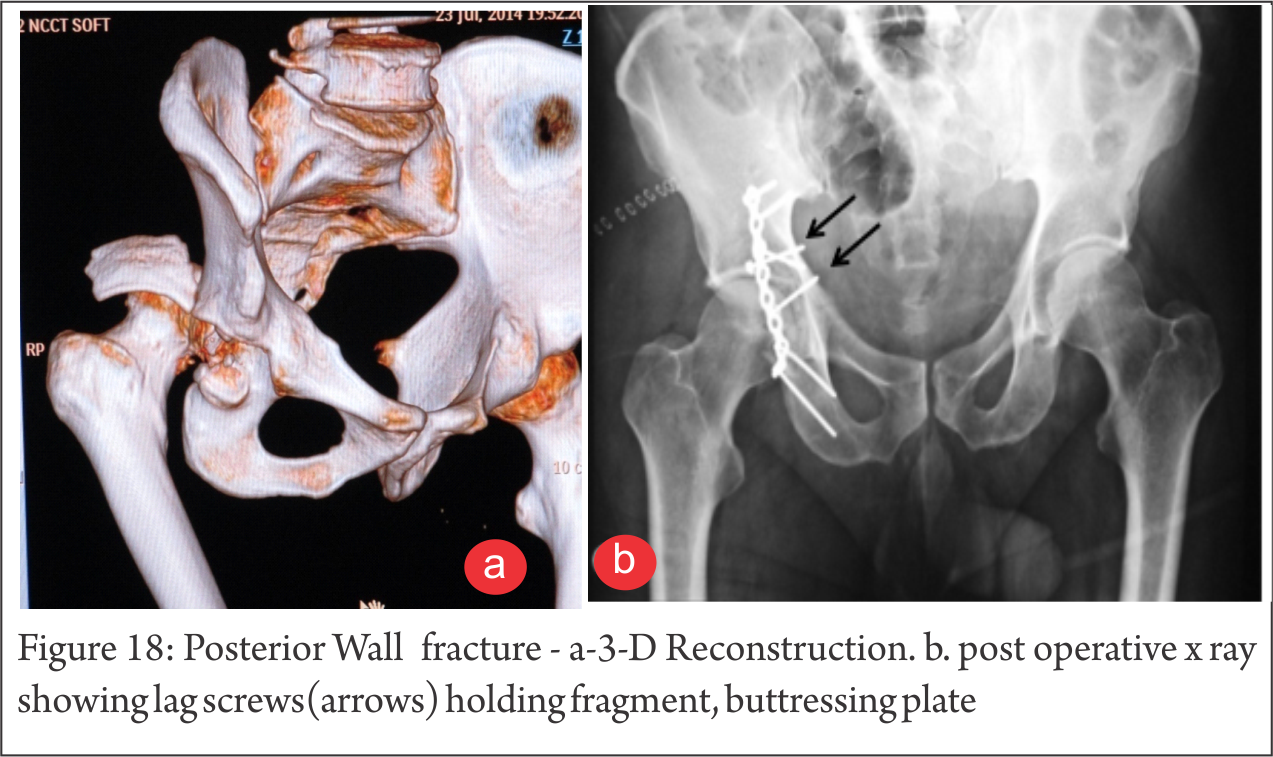
Post. Wall ( Fig.17,18) : A part of the rim with articular surface is broken. Often, it is displaced with subluxed/dislocated head Femur and best seen on Judet Obturator view (Fig 5,6). Comminution is not uncommon. Sciatic involvement is not infrequent and subtle injury even more common. On CT, marginal impaction can be picked up easily (Fig. 8).
Ant. Column (Fig 19) : Uncommon. Pure Ant. Wall fracture is even less common. It generally is a hallmark of elderly, osteoporotic individuals.

Transverse # (Fig. 20) : The fracture runs obliquely and can exit through weight-bearing Dome, at junction with Cotyloid fossa or through fossa itself. The distal fragment displaces medially and rotates. Both these factors need to be taken into account at ORIF. Though the fracture line traverses both Ilio-Pectineal and Ilio-Sciatic line, thus involving Anterior AND Post Columns, it still is not a “Both Column” Fracture, a term reserved for

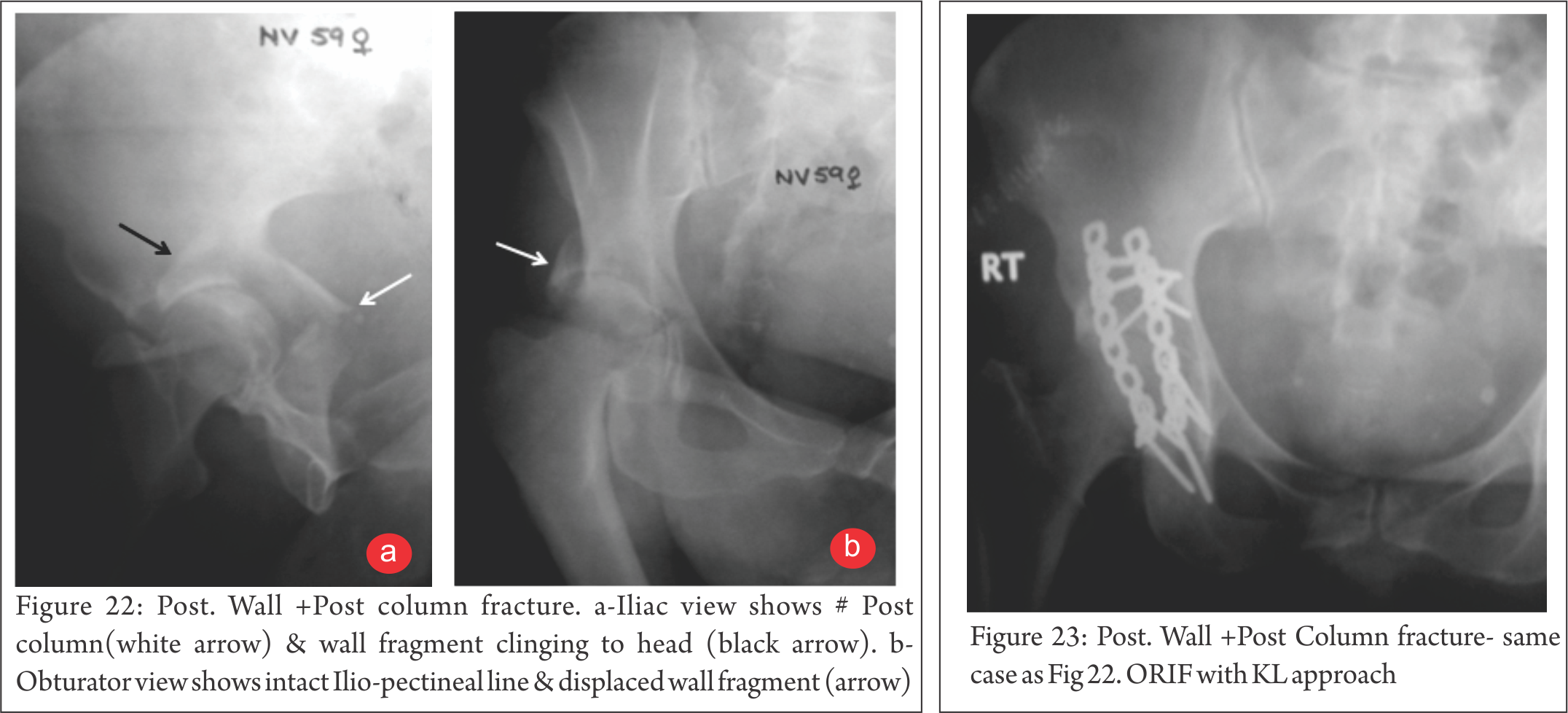
Post Wall and Column # (Fig 22, 23) : Post. Column break can occur in isolation or may be accompanied by Wall fracture. Column component exits proximally, Sciatic notch and distally, Obturator foramen. This is an unstable situation and at ORIF, Sciatic Nerve and Superior Gluteal neurovascular bundle are at risk.

Ant. Column with Post. Hemitransverse # (Fig. 24) : Not to be confused with Transverse or T #. The fracture line of Ant. Component exits obliquely compared to the straight line in Transverse #.
T-shaped # (fig. 25, 26) : The transverse component has additional break in Obturator fossa. This essentially separates Anterior and Posterior components. Therefore choosing appropriate approach is of paramount importance. Generally, the more displaced fragment decides approach. The other component is then reduced and held indirectly. Sometimes, two approaches may necessary.

Transverse with Post. Wall # (Fig. 27, 28) ; As name indicates, the post wall component makes the head displace posteriorly, often with communition.

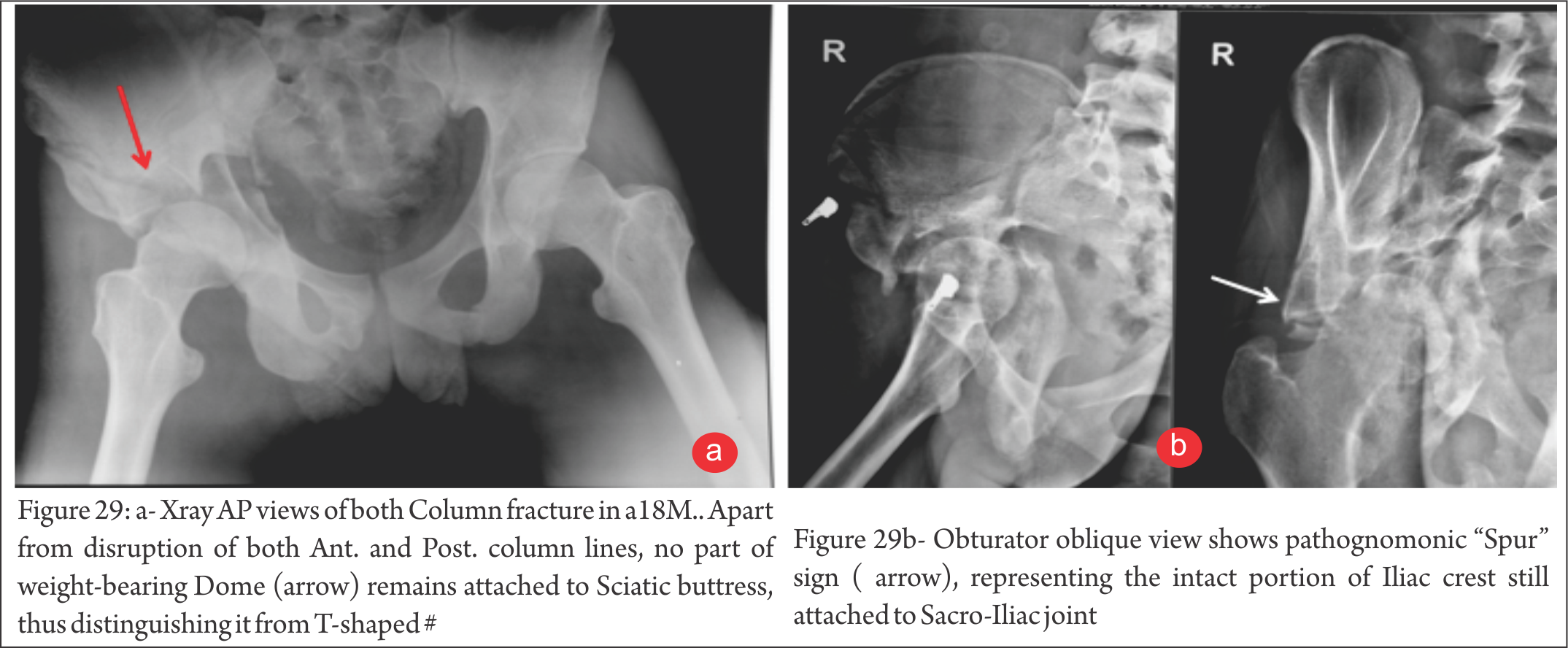
Both Column # (fig. 29) : No part of the weight-bearing Dome is connected to the Sciatic buttress. On Obturator view, “Spur” sign is characteristic of this pattern.

Fragility Fractures : (Fig. 31, 32) : With increasing longevity, the fracture patterns are also changing due to osteoporosis. Anterior wall, column injuries are common and many injuries are because of trivial fall on Greater Trochanter.

“Gull wing” sign, which shows a depressed/punched-in part of weight bearing area, is a bad prognostic indicator.
Some of these fractures can be picked only on MRI and if, despite negative X-ray, a strong suspicion prevails, MRI is indicated.
Conclusion
Acetabulum fractures need evaluation comprehensively by X-rays and CT Scans. Only then can this complex injury to a complex region be understood. Radiology not only provides assessment of injury, it helps choose best possible approach for stabilization, if indicated..
References
1. Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res 1980;(151):81–106.
2. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium: 2007—Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21(10 suppl):S1–S133.
3. Harris JH Jr, Lee JS, Coupe KJ, Trotscher T. Acetabular fractures revisited: part 1—redefinition of the Letournel anterior column. AJR Am J Roentgenol 2004;182(6):1363–1366.
4. Harris JH Jr, Coupe KJ, Lee JS, Trotscher T. Acetabular fractures revisited: part 2—a new CT-based classification. AJR Am J Roentgenol 2004;182(6):1367–1375
5.Leschka S, Alkadhi H, Boehm T, Marincek B, Wildermuth S. Coronal ultra-thick multiplanar CT reconstructions (MPR) of the pelvis in the multiple trauma patient: an alternative for the initial conventional radiograph. Rofo 2005;177(10):1405–1411.
6. Olson SA, Matta JM. The computerized tomography subchondral arc: a new method of assessing acetabular articular continuity after fracture (a preliminary report). J Orthop Trauma 1993;7(5):402–413
7. Geijer M, El-Khoury GY. Imaging of the acetabulum in the era of multidetector computed tomography. Emerg Radiol 2007;14(5):271–287
8. Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum: a meta-analysis. J Bone Joint Surg Br 2005;87(1):2–9
9. Patel NH, Hunter J, Weber TG, Routt ML Jr. Rotational imaging of complex acetabular fractures. J Orthop Trauma 1998;12(1):59–63.
| How to Cite this article: U K Sadhoo. Understanding Clinical Radiology of Fracture Acetabulum Trauma International May – Aug 2016;2(2):9-16. |
