Vol 2 | Issue 2 | May – Aug 2016 | page:25-30 | Nadeem Akhtar Faruqui
Author: Nadeem Akhtar Faruqui [1]
[1] Regency Hospital, Kanpur , Uttar Pradesh, India.
Address of Correspondence
Dr Nadeem A Faruqui
14/116d, Civil Lines,
Kanpur 208001 India
Email: nafaruqui@hotmail.com
Abstract
Hemorrhage is leading cause of death following pelvic fractures. 15-25% of patients of closed pelvic fractures and 50% of open pelvic fracture patients die as a result of haemorrhage. The main source of hemorrhage is the shearing injury of posterior thin walled venous plexus (80%). Other sources of bleeding include the bleeding cancellous bone and arterial injury. Injury to the pelvic viscera is also quite common because of the close proximity. Perineal lacerations make a closed injury into an open injury thereby more than doubling the risk of morbidity and mortality. Adequate fluid replacement and application of a pelvic Binder or Sheet can markedly reduce the mortality associated with this fracture. A linen sheet folded onto itself to make it about 20-30 cms wide applied tightly over the pelvis and centered over the trochanters can significantly reduce the mortality figures.
Keywords: Acetabulum fractures, pelvis fracture, emergency management.
Introduction
The basic principles of emergency management, Airway, breathing and circulation hold true for pelviacetabular fractures too. However there are certain practical tips and principles that will help in getting better results in these situations. These principles and tips are detailed below.
Hemorrhage is Leading Cause of Death
15-25% for closed pelvic fractures and 50% for open pelvic fractures are fatal secondary to exsanguination following either external or internal occult bleeding [1,2]. Increased mortality associated with
– systolic BP <90 on presentation
– age >60 years
– increased Injury Severity Score (ISS)
– need for transfusion > 4 units
– Head and neck injuries
Sources of Major Bleeding
• intrathoracic
• intraabdominal
• retroperitoneal
• extremity (thigh compartments)
• pelvic
• Common source of hemorrhage
• venous injury (80%)
• shearing injury of posterior thin walled venous plexus
• bleeding cancellous bone
• Less common sources of hemorrhage
• arterial injury (10-20%)
• superior gluteal most common (posterior ring injury, APC pattern)
• internal pudendal (anterior ring injury, LC pattern)
• obturator (LC pattern)
Blood Transfusion
Replacement volume is estimated by using the formula of 3 ml of crystalloid for each 1 mm of blood loss. A minimum of 2 litres of crystalloid solution is given rapidly if the patient is in shock. Crystalloid is administered until type-specific blood of non–cross-matched universal donor (O-negative) is available
• Packed RBC:FFP:Platelets should ideally be transfused in the ratio 1:1:1
• this ratio has been shown to decrease mortality in patients requiring massive transfusion
D) Disability
Clinical Examination
Pelvis: NO firm endpoint on rotation or traction indicates that there is no gross instablity (Fig 1). Pelvic compression and distraction test can detect gross instabilities, however these may at times be dangerous and can dislodge clots leading to further bleeding [3,4]. These test have been reported to have poor sensitivity and specificity and are no longer recommended in cases of pelvic fractures [4]

Perineum (Fig 2): Look for
• lacerations of perineum
• degloving injuries
• flank hematoma
• scrotal, labial or perineal hematoma, swelling or ecchymosis
• urethral bleeding

Rectal Examination
mandatory to rule out occult open fracture
• rectal blood
• anal sphincter tone
• bowel wall integrity
• bony fragments
• prostate position
Vaginal Examination
mandatory to rule out occult open fracture
Presence of blood in vaginal vault
Vaginal lacerations

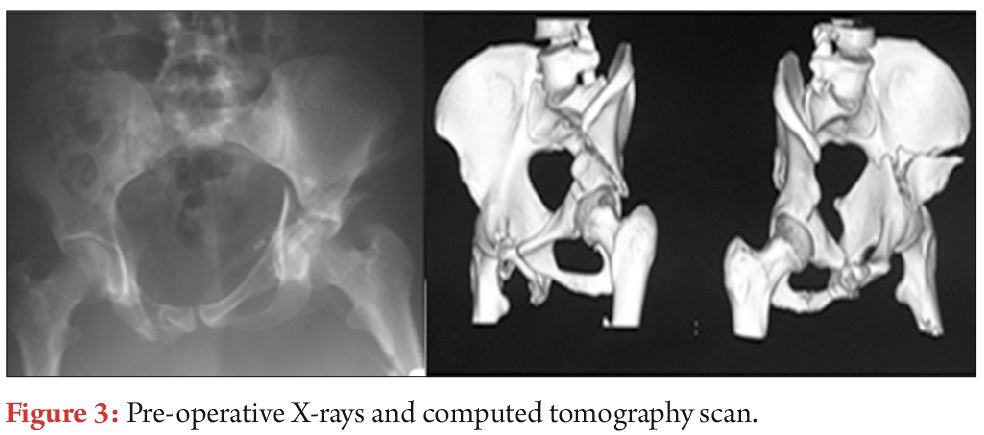
Urogenital Examination (Fig 3)
Bladder and the urethra are most frequently injured (25-30% of major pelvic fractures). 66% male versus 34% females patients difficulty in voiding urine or blood at the urethral meatus.
95% of bladder injuries have gross haematuria
urethral injuries are suspected under following clinical scenario
• blood at the urethral meatus
• gross hematuria
• inability to spontaneously void
• high riding prostate on rectal examination
• retrograde urethrogram (RUG) should ideally be done before insertion of Urinary catheter in unstable patient with suspected urethral injury make only 1 attempt to pass the urinary catheter, if it fails do RUG
Neurologic Examination
• rule out lumbosacral plexus injuries (L5 and S1 are most common)
• rectal exam to evaluate sphincter tone and perirectal sensation
Whenever an unstable pelvic injury is suspected in a haemodynamically unstable patient, a pelvic binder/sheet should be applied to control bleeding
The goal of treatment for pelvic fracture stabilization is early control of life-threatening hemorrhage. Returning pelvic bones to correct position helps to reduce pelvic volume and control venous bleeding.
Pelvic Binder [5,6]
• Applies compression leaving less space for blood to accumulate. It decreases the pelvic volume and also reduces pelvic fractures
• Tamponades bleeding sources, such as fractured bony surfaces or ruptured vessels
• Reduces instability of the injured pelvis
• Prevents further damage to pelvic organs and vessels
• Reduces pain by limiting movement of pelvis
Commercially available pelvic binder are also useful but use of lumbosacral belts is to discouraged [6].
Pelvic Binder/sheet
Indications
• initial management of an unstable pelvic ring injury
Contraindications
• hypothetical risk of over-rotation of hemipelvis and hollow viscus injury (bladder) in pelvic fractures with internal rotation component (LC)
• no clinical evidence exists of this complication occurring
Technique
• A linen sheet folded onto itself to make it about 20-30 cms wide is passed under the pelvis
• Centered Over Greater Trochanters to effect indirect reduction
• Applied very tightly over the pelvis
• do not place over iliac crest/abdomen as it makes the ineffective and precludes assessment of abdomen
• augmented with traction & internal rotation of lower extremities and taping at knees & ankles
• transition to alternative fixation as soon as possible
• prolonged pressure (>24 hours) from binder or sheet may cause skin necrosis
• working portals may be cut in sheet to place percutaneous fixation
Lumbosacral belt should not be used because it is elastic and cover abdomen.
Important note. Binder should be centered over the TROCHANTERS and Not the ASIS
Because of their ease of use and fast application, Pelvic Binders have
largely replaced the Pelvic C-Clamp and External Fixators for early
mechanical stability in pelvic fracture [5].
Radiology & CT
X-ray Pelvis –AP
Pelvis Is Unstable When There Is
Sacro-Iliac joint Diastasis > 1 cm or
Cephalad Displacement of Posterior Sacro-Iliac Complex > 1 cm
Usually associated with Avulsion fracture of ischial spine, ischial tuberosity, sacrum or transverse process of 5th lumbar vertebrae
High Risk Patients as per the Young and Burgess Classification:
– LC III
– APC II
– APC III
– VS
– CM
Ct Scan is the Gold Standard
CT scan is essential in determining:
Posterior ring instability
Helps define comminution and fragment rotation
Intra-articular fragments
Fractures of articular surface of acetabulum and femoral head
Ultrasonography
Allows Focused Assessment with Sonography for Trauma (FAST)
Four classic areas are examined quickly by ultrasonography for free fluid (Blood):
Perihepatic space (hepatorenal recess)
Perisplenic space
Pericardium
Pelvis
External Fixation/ Stabilization of Pelvic Ring Injury
These are temporary life saving measures in the acute stage to stabilize the pelvis in a haemodynamically unstable patient. However, None of these methods can fully stabilize the pelvis. These are put on till such time as more definitive fixation can be done.
Femoral traction pin with 10-12 kg weight should be applied to maintain the reduction of the hemipelvis.
Mode of Action of External Fixation
•Decreases pelvic volume
•Stabilizes bleeding bone surfaces and venous plexus in order to form clot
•Reduces Pain
Types
A) Pelvic Binder/sheet
B) Pelvic C Clamp
C) External Fixator
A) Pelvic Binder/Sheet
Easily available everywhere annd is easy to apply. Technique of application discussed previously
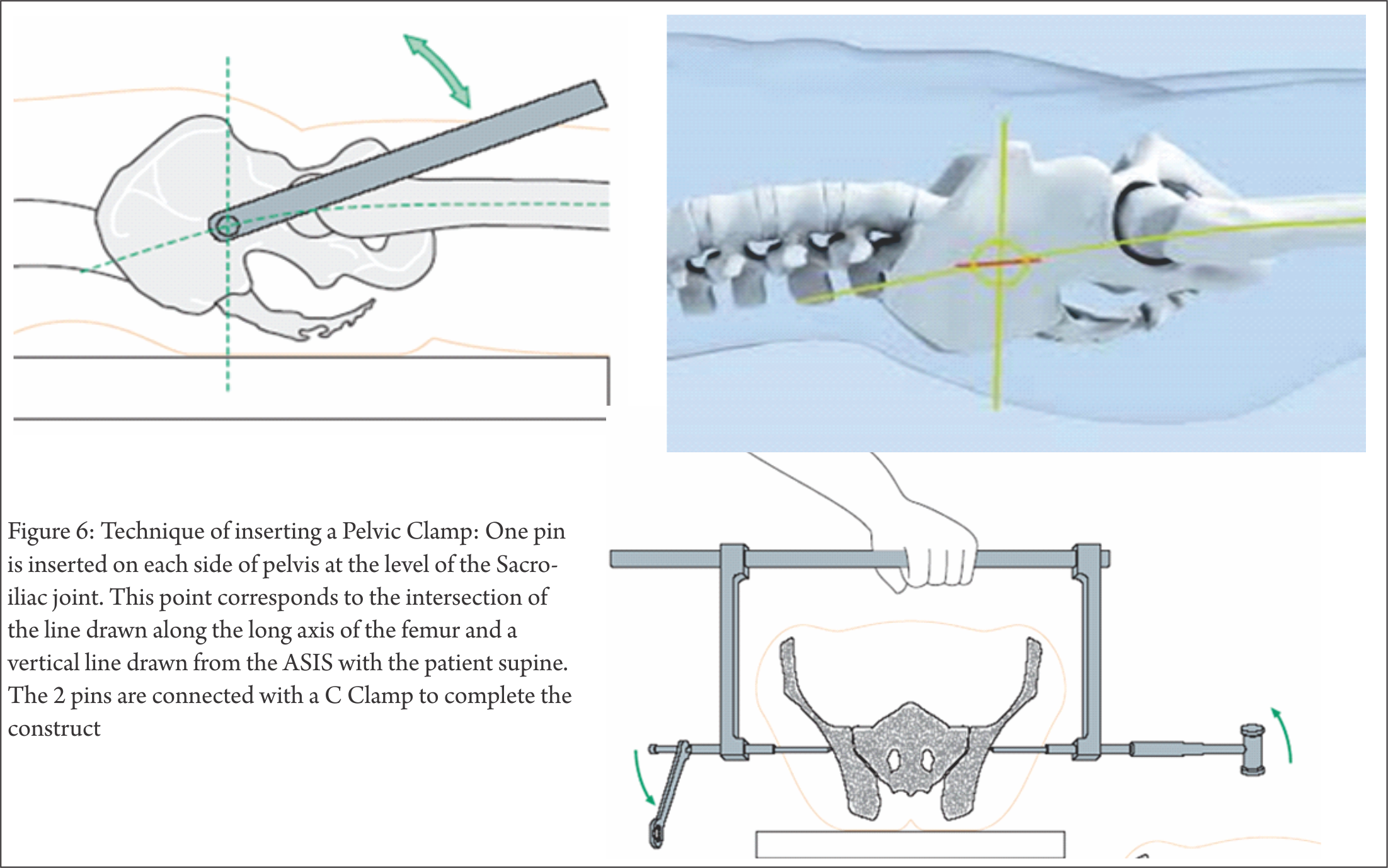
B) Pelvic C Clamp (Fig 6)
Indications
– Emergency stabilization of Sacroiliac joint disruptions and fractures of the sacrum with associated circulatory instability
Contraindications
Absolute contraindications are:
•Fracture lines within the illium (transiliac fracture) as it bears the risk of pin perforation through the fracture line
•Hemodynamic stability in Pelvic fractures
Relative contraindications are:
•Hemodynamic stability of the patient after Unstable type injuries
•Comminuted sacral fractures with risk of compression of the sacral nerve plexus
In life threatening situations hemorrhage control takes priority over the potential risk of nerve root compression
One Pin is inserted on each side of pelvis at the level of the Sacro-iliac joint. This point corresponds to the intersection of the line drawn along the long axis of the femur and a vertical line drawn from the ASIS with the patient supine. The 2 pins are connected with a C Clamp.
Advantage
Can be applied in the emergency room
Laparotomy can be done with the C Clamp in place
Disadvantage
Costly and not available everywhere.
Efficacy similar to Pelvic Binder/ Sheet.
C) External Fixator
Indications
Pelvic ring injuries with an external rotation component (apc, vs, cm)
Provide only marginal stability in vertically unstable ring injury
APC II (OPEN BOOK injuries with posterior ligaments/hinge intact) :
All designs work
APC III injuries (Post Ligaments damaged)
No designs work well (but AIIS frames better than ASIS frames)
Contraindications
•Ilium fracture that precludes safe application
•Acetabular fracture

Technique
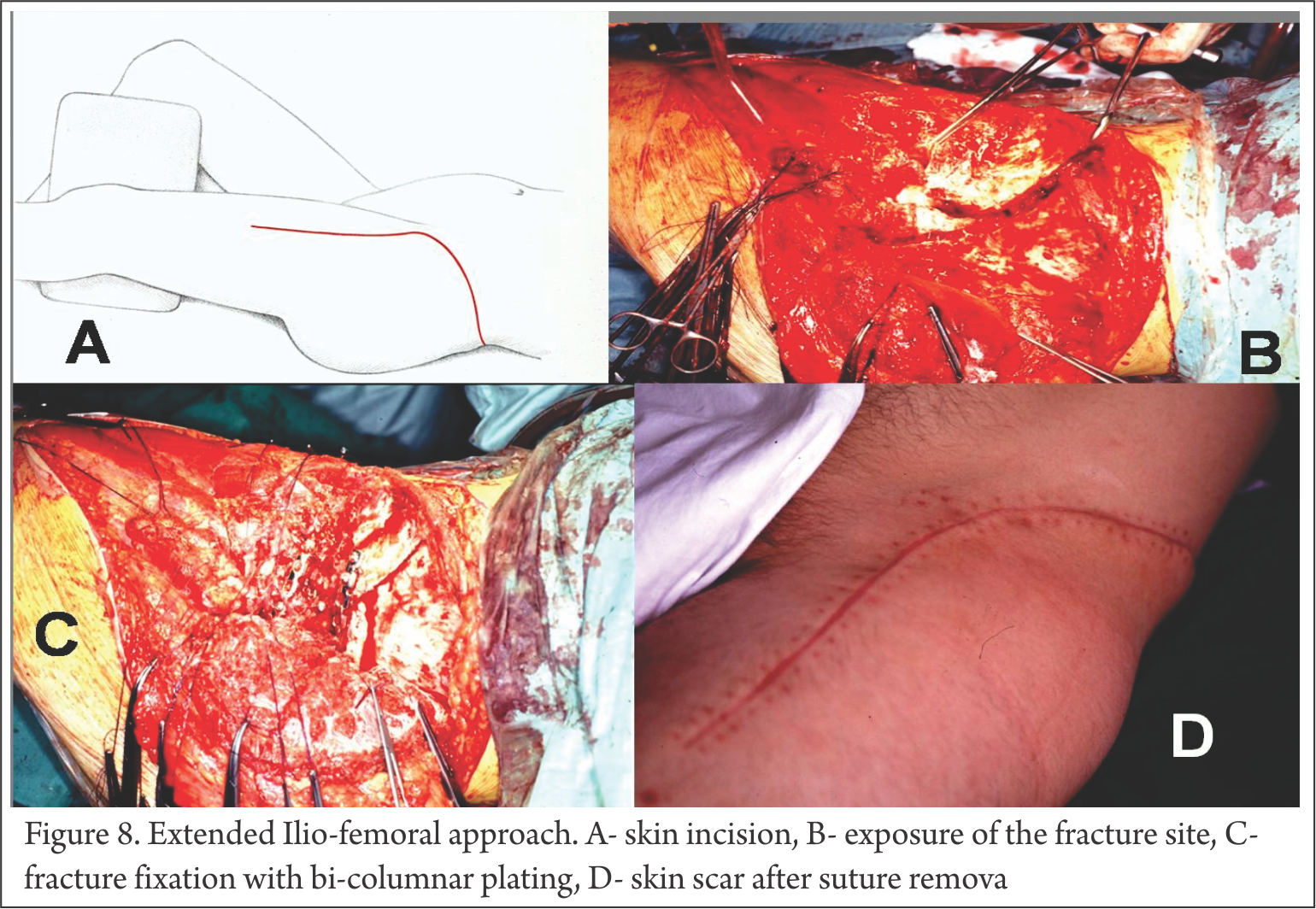
Pin insertion in iliac crest (ASIS) (Fig 7)
multiple half pins inserted in the superior iliac crest placed in thickest portion of anterior ilium or gluteus medius tubercle
Should be placed before emergent laparotomy
• Stab incision over iliac crest
• Pass 2 K-wires by hand 1 each on medial & lateral sides of iliac wing
• Drill hole started at junction of Medial 1/3 & lateral 2/3rd of iliac crest
• 45 degree inclination lateral to medial
• Ceplalad to caudal direction – towards acetabulum
• Drill 1 cm
• 5 mm Schanz pin inserted with hand
• Cortical walls to guide pin into position
• Obturator Oblique view on C-Arm /Outlet view
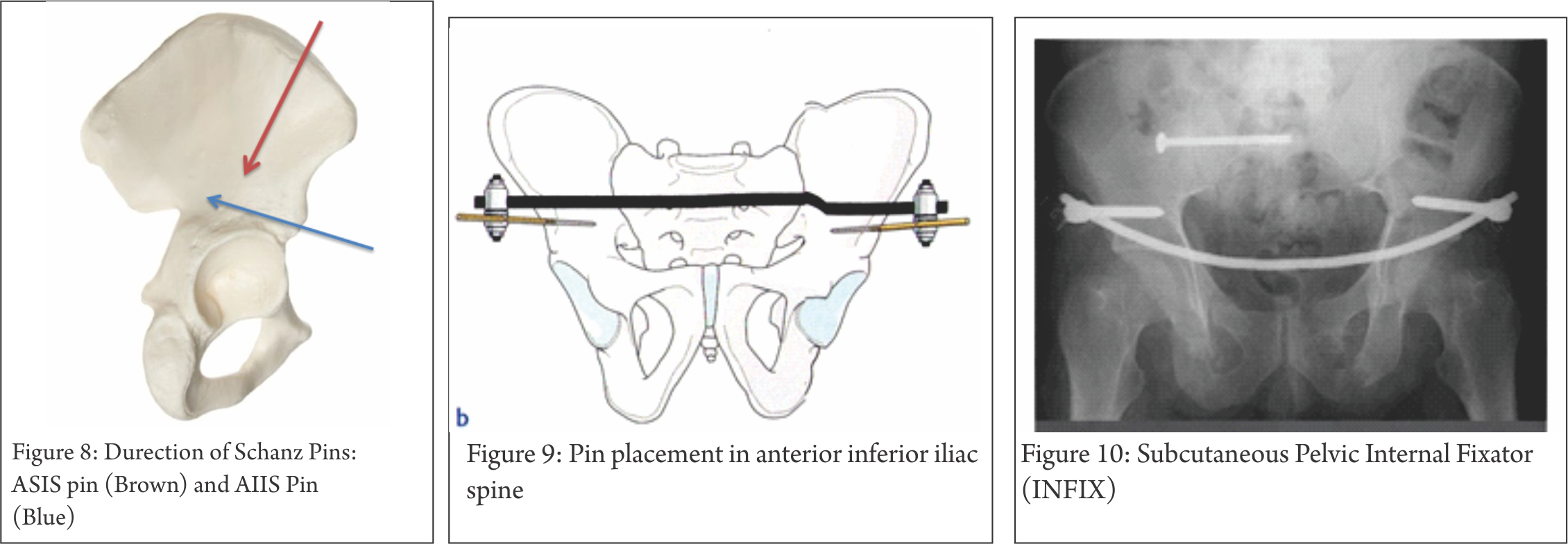
Pin Placement In Anterior Inferior Iliac Spine (AIIS) Fig 8,9)
single pin in column of supra-acetabular bone from AIIS towards PSIS. Obturator outlet or “teepee” view can be used to visualize this column of bone. AIIS pins can place the lateral femoral cutaneous nerve at risk
Tranverse skin incision at or below AIIS
•Muscles split longitudinally to avoid lateral femoral cutaneous nerve injury
•Drill through trocar under image intensifier towards greater sciatic notch
•Pins directed 30-450 towards midline in frontal plane
•Pins directed perpendicular to body axis or slightly cephalad
•Schanz pins of 50-70mm thread length required
•Fixator bar connects the pins on both sides
•Permits easy access for laparotomy
Subcutaneous Pelvic Internal Fixator (INFIX) (Fig 10)
One pedicle screw is fixed in the supra-acetabular bone of the ilium on each side. The pedicle screws are connected to each other by a rigid, anteriorly bowed fixation rod passed subcutaneously superficial to the sartorius muscles [7]
Less infection and wound site morbidity
After Stabilization/ External Fixation Of Pelvic Ring Injury
A) Control Hemorrhage
B) Control Contamination
A) Control of Haemorrhage
1) Pelvic Packing (Fig 11)
Make Midline Incision, pack the wound with sponges. Apply External Fixator. DON’T TRY TO LIGATE THE BLOOD VESSELS..Re-open wound after 24-48 hours and then ligate the vessels if possible or required.

2) Angiography
Indications
•Small bore artery (sup gluteal or obturator) can be controlled by embolization
•No role in Venous or bony bleeding
Available only in select centres and success based on multiple variables including: stability of patient, proximity of angiography suite, availability and experience of staff
CT angiography useful for determining presence or absence of ongoing arterial hemorrhage (98-100% negative predictive value)
Contraindications
• not clearly defined
Technique
•selective embolization of identifiable bleeding sources
• if uncontrolled bleeding even after selective embolization, bilateral temporary internal iliac embolization may be effective
• complications include gluteal necrosis and impotence
B) Control of Contamination
• Debridement & Packing of Open Wounds
• Suprapubic Catherization
• Diverting Colostomy
Conclusion
Priciples of pelvis fracture damage control
External Fixation
Pelvic Binder
Pelvic C-clamp
External Fixator
Control of Haemorrhage
Pelvic packing
Angiography
Control of Contamination
Debridement & packing of Open Wounds
Suprapubic catherization
Diverting colostomy.
References
1. O’Sullivan RE, White TO, Keating JF. Major pelvic fractures: identification of patients at high risk. J Bone Joint Surg Br. 2005;87(4):530-3.
2. Kido A, Inoue F, Takakura Y, Hoshida T. Statistical analysis of fatal bleeding pelvic fracture patients with severe associated injuries. J Orthop Sci. 2008;13(1):21-4.
3. Lee C, Porter K. The prehospital management of pelvic fractures. Emerg Med J. 2007 Feb;24(2):130-3
4. Grant PT. The diagnosis of pelvic fractures by ‘springing’. Arch Emerg Med. 1990 Sep;7(3):178-82.
5. Bottlang M, Krieg JC, Mohr M, Simpson TS, Madey SM. Emergent management of pelvic ring fractures with use of circumferential compression. J Bone Joint Surg Am. 2002;84-A Suppl 2:43-7
6. Mohanty K, Musso D, Powell JN, Kortbeek JB, Kirkpatrick AW. Emergent management of pelvic ring injuries: an update. Can J Surg. 2005 Feb;48(1):49-56.
7. Vaidya R, Kubiak EN, Bergin PF, Dombroski DG, Critchlow RJ, Sethi A, Starr AJ. Complications of anterior subcutaneous internal fixation for unstable pelvis fractures: a multicenter study. Clin Orthop Relat Res. 2012 Aug;470(8):2124-31.
| How to Cite this article: Faruqui NA. Emergency Management of Pelvic Fractures. Trauma International May-Aug 2016;2(2):25-30. |
(Abstract) (Full Text HTML) (Download PDF)