
Fixation of Inter-condylar Eminence fragment in Bi-condylar Tibial plateau fracture – Technical note
Vol 2 | Issue 2 | May – Aug 2016 | page:50-52 | RM Chandak
Author: RM Chandak [1]
[1] Chandak Nursing Home Nagpur Maharashtra India.
Address of Correspondence
Dr. RM Chandak
Chandak Nursing Home Nagpur Maharashtra India.
Email: chandakrm@yahoo.com
Abstract
Bicondylar tibia fractures are most of the time associated with a separate tibial eminence fragment. This fragment is wedge shaped and is lodged between the two main condylar fragments. We we apply clamps to the condylar fragments to hold the fracture, this wedge shaped fragment may get dislodged in the joint cause incongruous reduction. This may later cause knee pain and stiffness. It is important to identify these fragments in bicondylar fractures and to try and reduce them using the technique described below. This will avoid the stiffness and help achieve better and early range of movement
Keywords: Tibia eminence fracture, bicondylar tibia fracture.
Introduction
Bi-condylar tibial plateau fractures are serious injuries and difficult to treat more so if associated with inter-condylar eminence fracture.
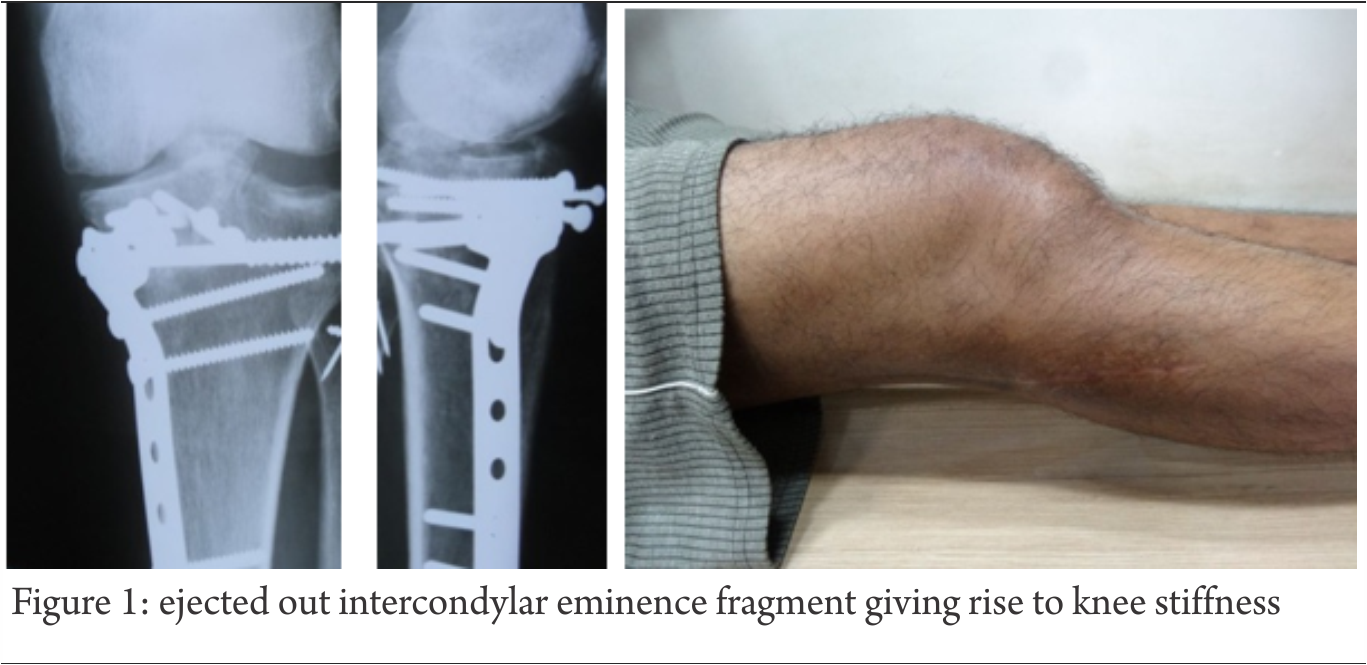
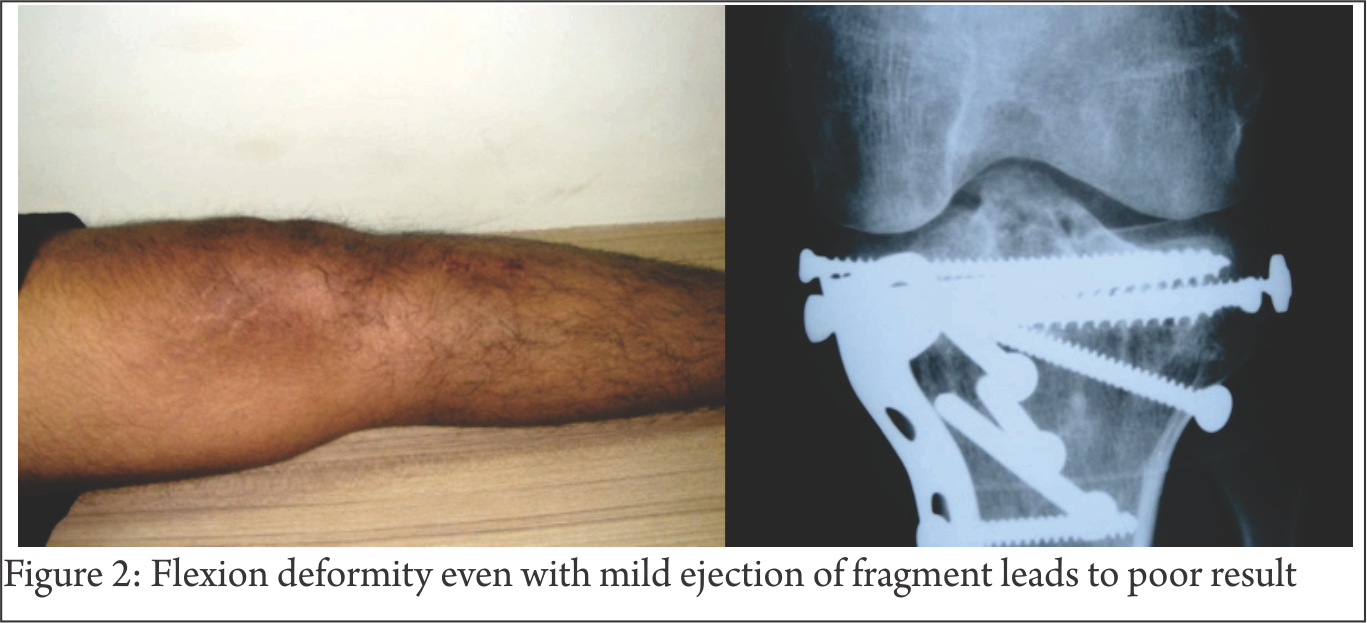
The goal of treatment is to re-establish Joint stability, alignment, articular Congruity, Giving better functional outcome We are used to manage bi-condylar fractures with plates and screws at times resulting into flexion deformity and poor outcome due to ejected out eminence area (Fig. 1) Even small amount of dislogment of the fragment leads to pain and stiffness (Fig 2).
Surgical Technique
The surgical technique is basically aimed at preventing the dislodgement of the eminence fracture. In our example a 45 year old male presented with bicondylar proximal tibia fracture (Fig. 3).

CT Scan is essential in such comminuted cases to determine which column needs buttressing (Fig. 4). This will also help in planning of plates and reduction maneuver is according to complexity of fracture. CT also gives us direction and dimension for fixation of inter-condylar eminence area.
For bicondylar tibial fractures, reduction clamps are effective means of achieving reduction and compression however many a times this causes ejection of the tibial eminence fragment (Fig. 5).

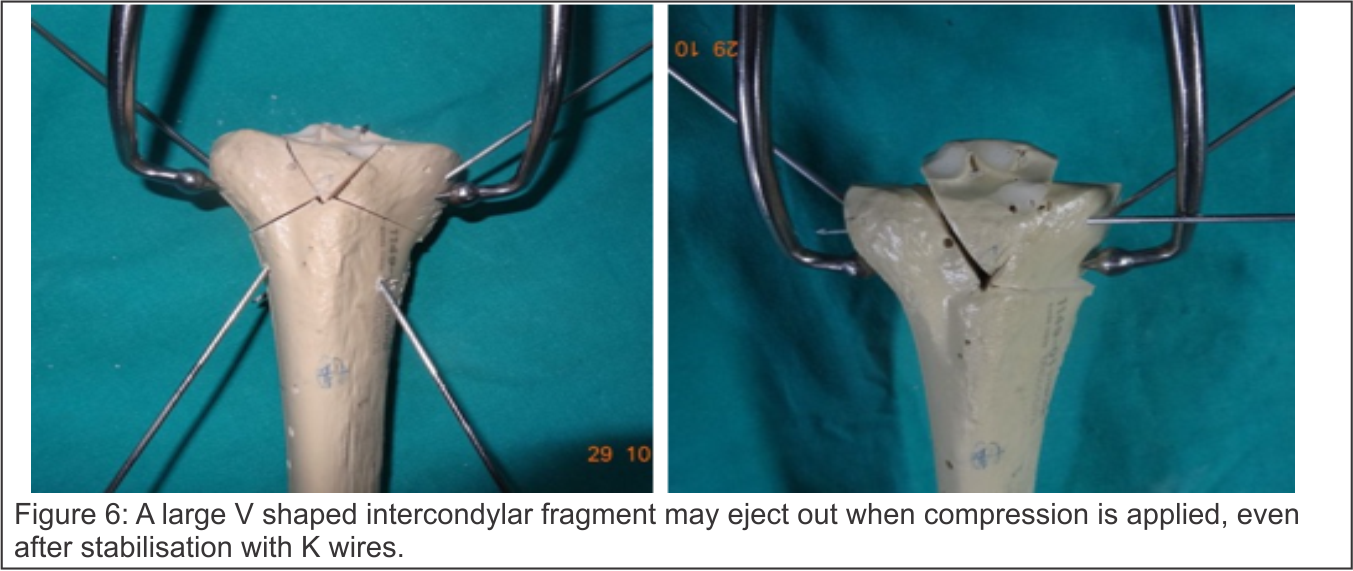
Specially a large V shaped fragment easily eject out on compression even if cross K wires have been used for temporariy fixation (Fig 6).
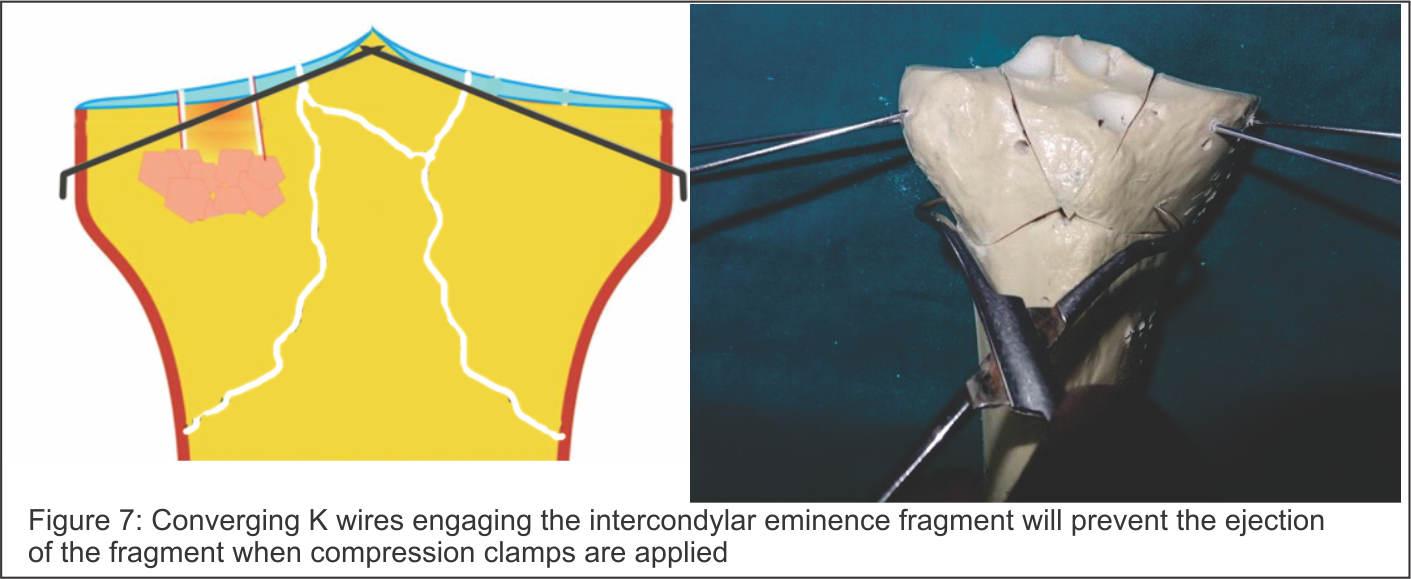
The main crux of this technique is putting in multiple K wires starting from proximal converging towards the intercondylar eminence. The wires may not pass through the the joint. These converging wires not only hold the condylar fragments but also prevent ejection of the interdondylar eminence fragment (Fig. 7).
If the fragment is too unstable and ejects out while putting in the K wires, direct pressure can be applied to the fragment by probe or Dura elevator (Fig. 8).
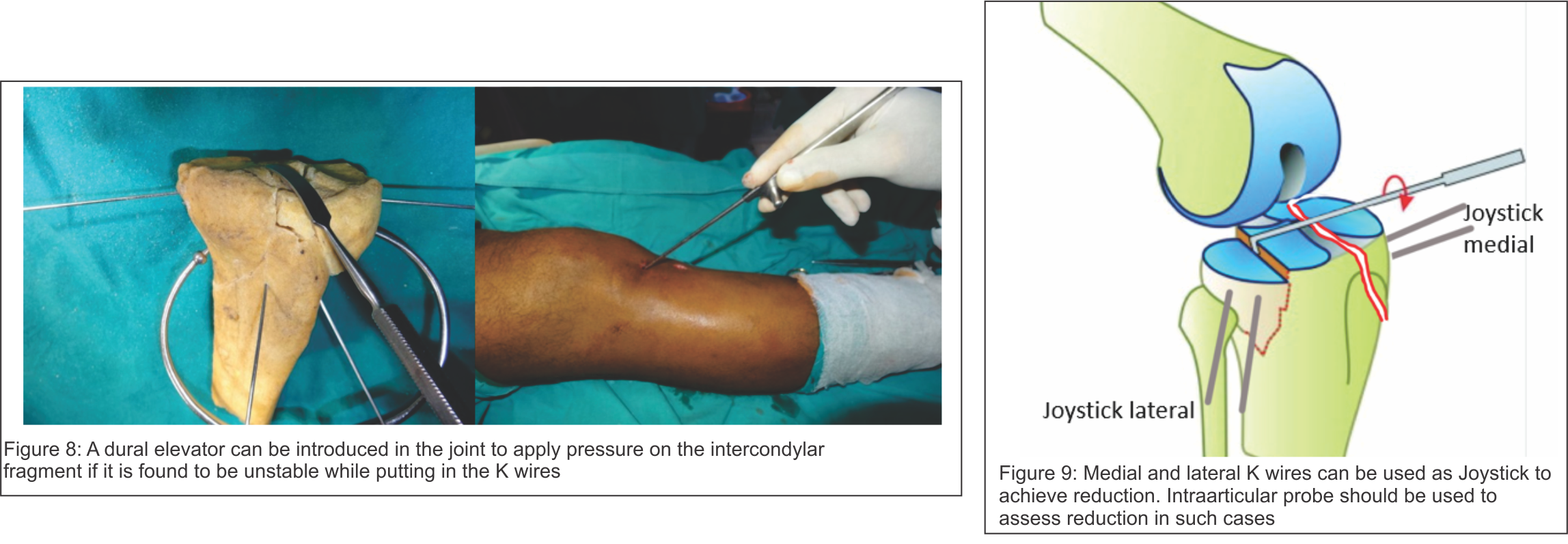
To begin with two K wires each can be put in both the medial and lateral fragment and these can then be used to joystick the fragments into reduction with the intercondylar fragments (Fig. 9). In case the central fragment is depressed, it will need elevation as first step and then reduction can proceed as above. A palpating probe can be introduced in the joint to assess the reduction by using a separate stab incision (Fig. 9). All fragments should be reduced and held before application of plates (Fig. 10).
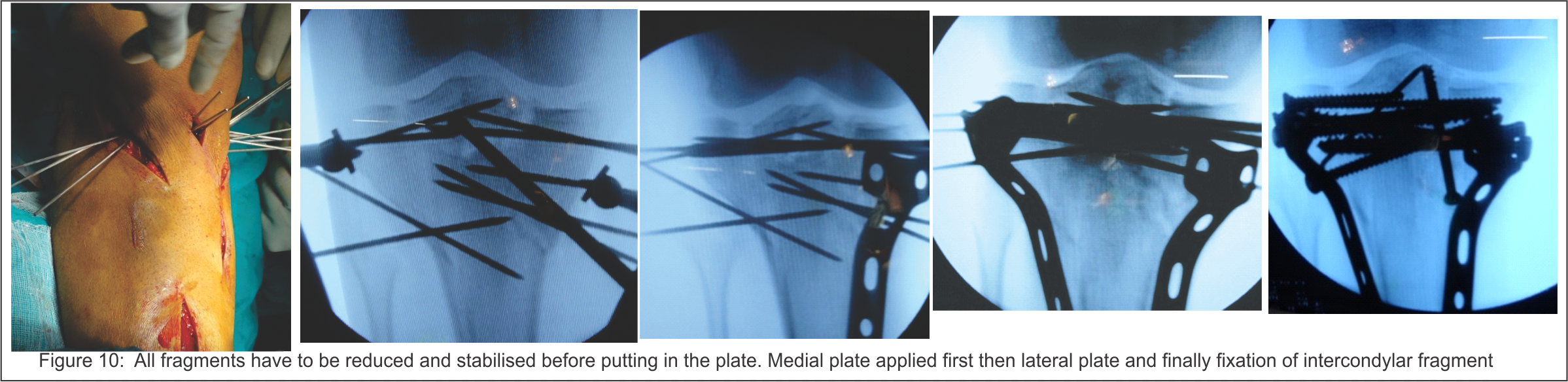
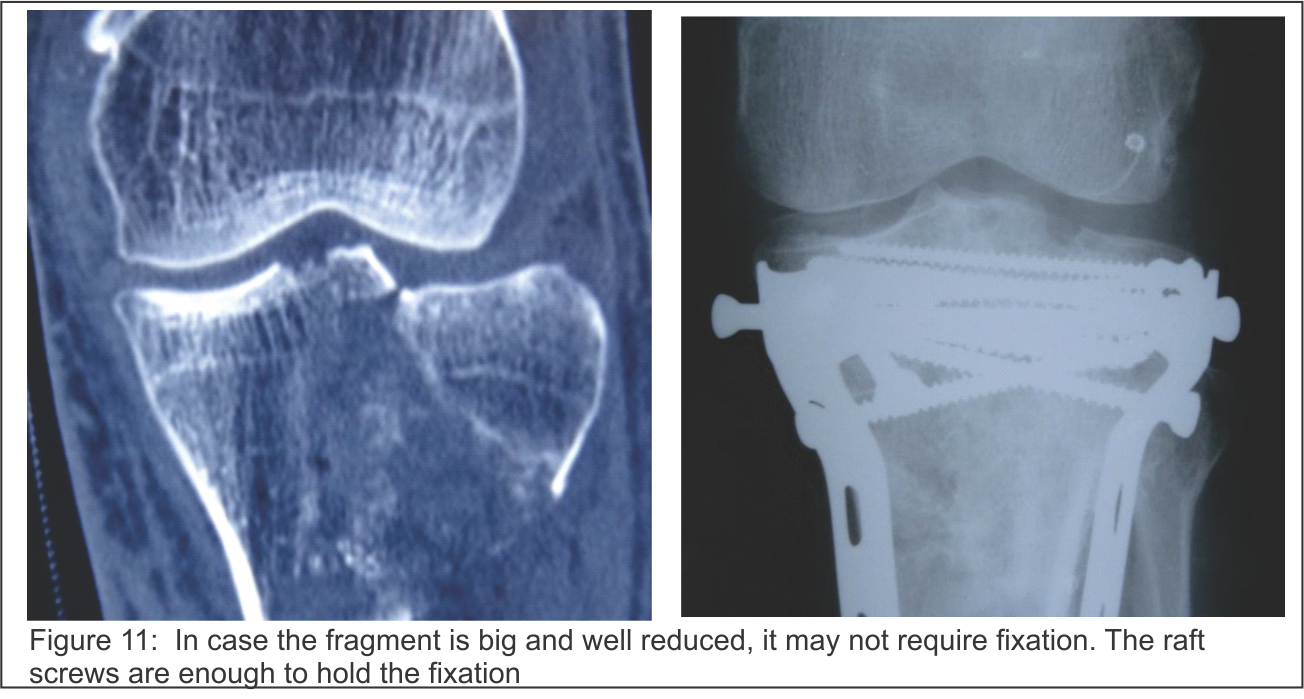
The trick is to reduce the intercondylar fragment with relation to both medial and lateral fragment by using joystick wires. Advancing the joystick wires in the intercondylar fragments once the reduction is achieved. Lastly apply the reduction clamps only one the reduction is achieved and is temporarily stabilised by raft wires. At times the intercondylar fragment may be a single large fragment and can be easily reduced. In these cases if the fragment remains reduced after application of compression clamps, there may be no need for fixation of this fragment and raft screws can hold the fragment well (Fig. 11).
However in cases the fragment is comminuted and is unstable after compression, K wires can be left as fixation methods or in case the fragment is large enough a screw can be used to fix the fragment (Fig. 12,13). Occasionally avulsed ACL fragment alone can be fixed with pull out suture in same or sub sequent procedure.
Conclusion
• Anatomical reduction and stabilisation of inter-condylar eminence fracture associated with bi-condylar tibial plateau fracture is necessary for good outcome.
• If the fragment is stable on condylar compression – don’t fix
• Fixation is a must if fragment ejects out with compression.
| How to Cite this article: Chandak RM. Fixation of Inter-condylar Eminence fragment in Bi-condylar Tibial plateau fracture – Technical note. Trauma International May – Aug 2016;2(2):50-52. |
