
Classification of Pelvis and Aetabulum Injuries
Vol 2 | Issue 2 | May – Aug 2016 | page:4-8 | Sameer Aggarwal, Vikas Bachhal
Author: Sameer Aggarwal [1], Vikas Bachhal [1]
[1] Department of Orthopaedics, PGIMER, Chandigarh, Punjab, India.
Address of Correspondence
Dr Sameer Aggarwal
Department of Orthopaedics, PGIMER, Chandigarh, Punjab, India.
Email: drsameer35@yahoo.co.in
Abstract
Classifications are meant for easier academic communication as well as predict prognosis and outcome. The importance of classification is best stressed in case of pelvis and acetabular fracture. the complex anatomy of the area and complexity of the injuries makes it difficult to standardise a classification that will easily predict the management protocol and outcomes. Various attempts have been made over the years to find the best classification system for these complex injuries and this review takes the readers through these many classifications and also presents the currently acceptable classification.
Keywords: Hip fractures – complication – salvage procedure – therapeutic algorithm.
Introduction
The earliest attempt at classifying pelvic ring injuries was made by Bucholz where he described three groups essentially defining anteroposterior injuries of later classification systems.[1] Pennal et al described their classification based on mechanism of injury as anteroposterior compression injuries, lateral compression injuries, or vertical shear injuries.[2] This classification was later modified by more comprehensive description of same groups by Young and Burgess while Tile modified the original Pennal classification by factoring in the vital element of stability.[3,4] Both these later classification systems are in current common usage although they compliment each other as Young and Burgess gives better anatomical description of injury thereby guiding the type of fixation, while Tile factors in the element of stability which is the single most important factor dictating need for fixation. Helfet later developed comprehensive system of classification where he incorporated both these existing systems and described injuries on the lines of AO/OTA system.[5] Although for routine usage many prefer to use either Young-Burgess or Tile system, however it is recommended to use comprehensive system for the purpose of comparing or reporting results.
Young-Burgess classification (Mechanism of Injury)
It is useful to predict mortality, transfusion requirements, and associated organ injury. This system classifies the pelvic ring injuries into four types according to vector of force causing them. These are anteroposterior compression (APC), lateral compression (LC), vertical shear (LC) and combined mechanism (CM) injuries. Both APC and LC injuries are further divided into three groups according to extent of injury (Fig. 1, Table 1).
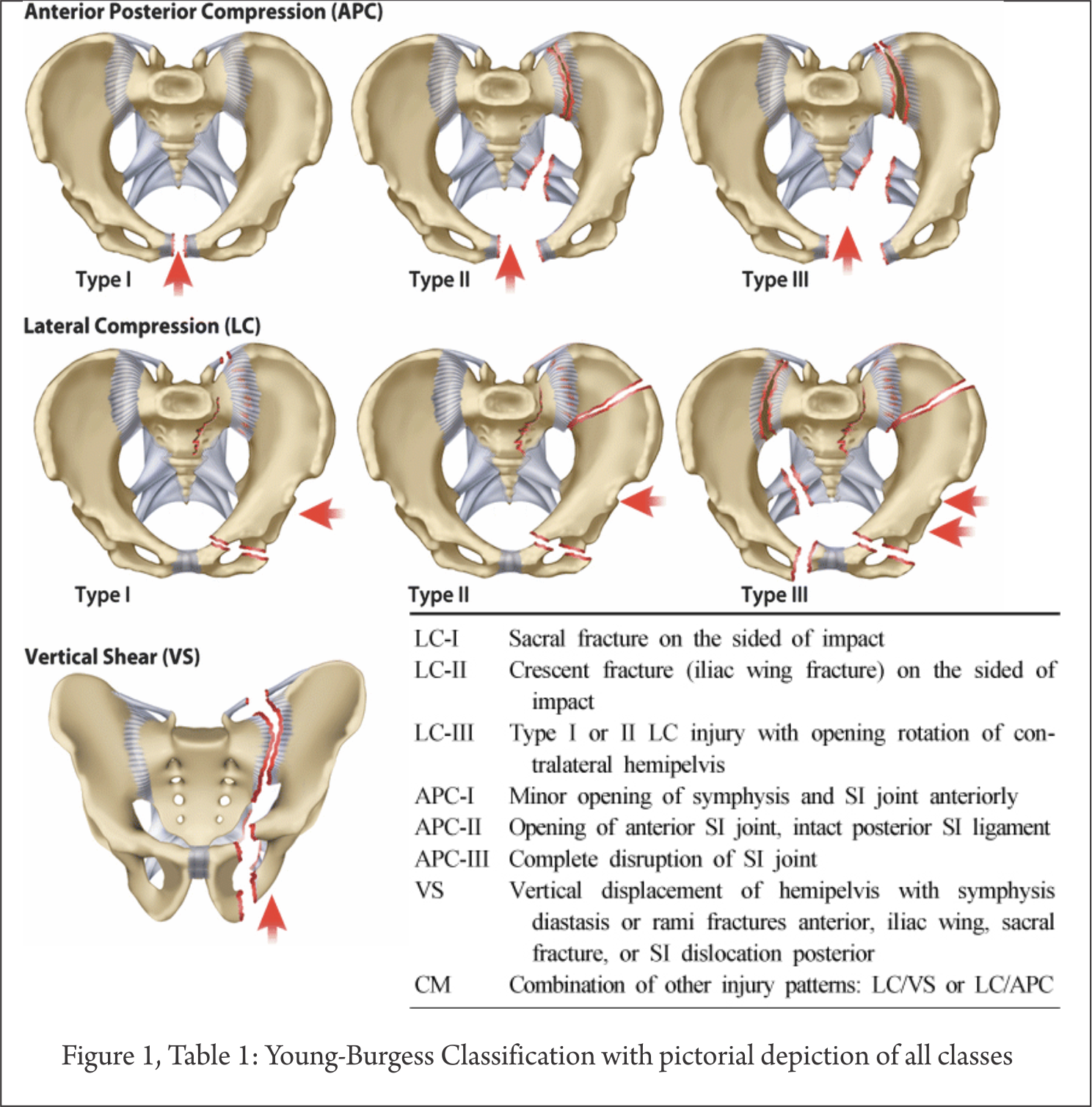
Anteroposterior Compression
The essential element is disruption of anterior ring generally at symphysis. The three subgroups represent progressive extent of injury involving only symphysis (APC I), disruption of pelvic floor and anterior sacroiliac ligament (APC II) and disruption of posterior sacroiliac ligaments (APC III). Although earlier studies showed predictive level of diastasis for these three groups (APC I: 1-2.5cm, APCII: 2.5-4cm; APCIII: >4cm), however this has been challenged recently. Moreover, radiographs represent only a static image and might underestimate the extent of injury which require stress examination under fluoroscopic guidance for more comprehensive evaluation.
Lateral Compression
The essential lesion in this injury pattern is injury to posterior ring with anterior displacement at level of symphysis or fractured rami. Posterior lesion can be either compression fracture of sacrum (LC I) or fracture dislocation of sacroiliac joint where a crescent shaped portion of iliac bone remains attached to sacrum while rest of joint is dislocated (LC II; crescent fracture). LC III injuries have either LC I or LC II ipsilateral injury with contralateral open book injury of sacroiliac joint (windswept pattern).
Vertical Shear
The essential element of this pattern is vertical and posterior displacement of hemipelvis typically assessed at posterior ring level. Posterior ring injury may be at sacrum, sacroiliac joint or ilium which is combined with anterior injury at symphysis or rami.
Combined Mechanism
It is not uncommon to see injuries where more that one of the above mentioned mechanisms are at play. All such injuries are grouped under CM injuries
Tile’s classification (Stability classification)
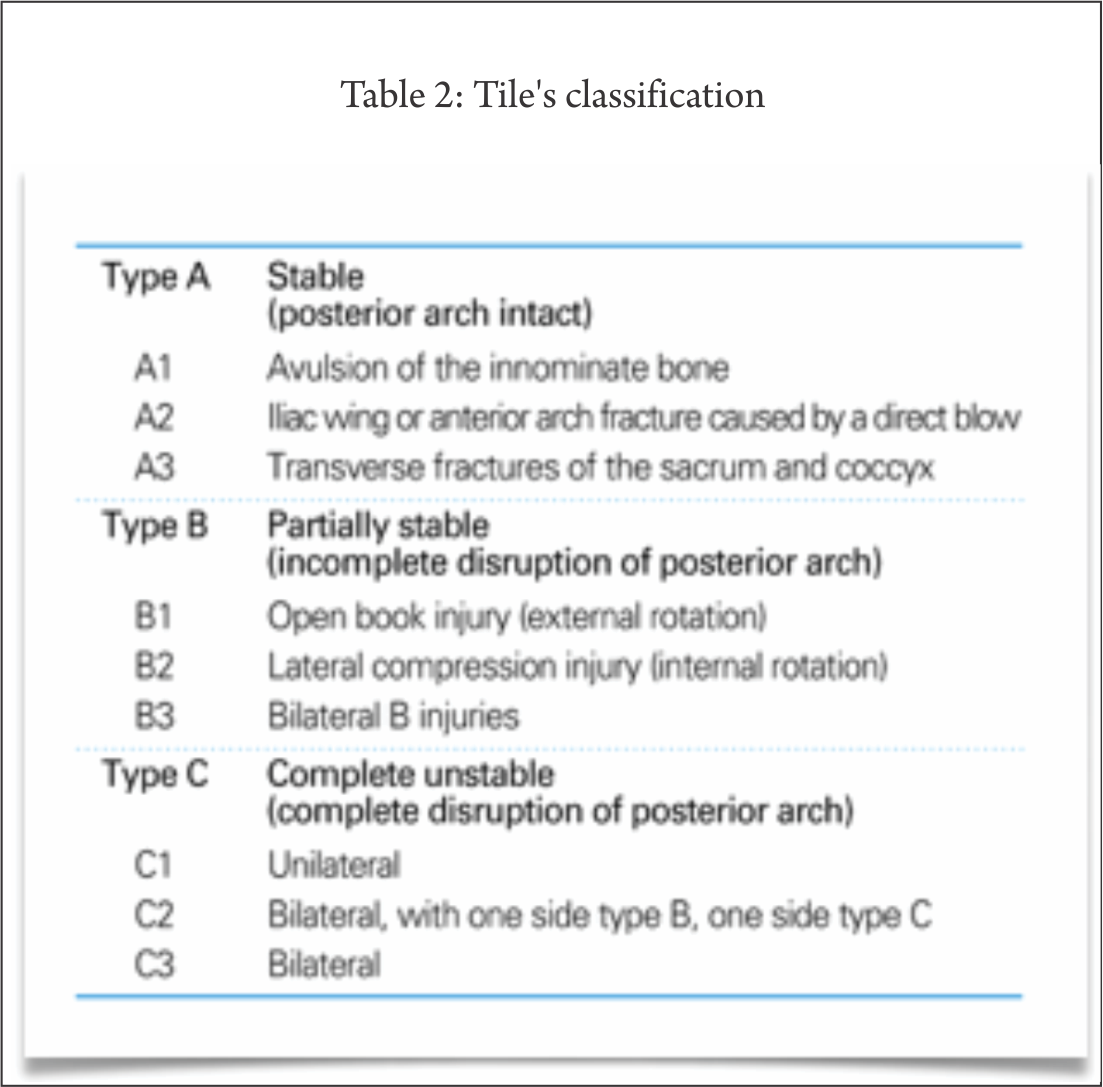
Tile laid emphasis on integrity of posterior arch to determine stability and classified pelvic ring injury into stable injuries with intact posterior ring (Type A); partially stable injuries with incomplete disruption of posterior ring (Type B) and unstable injuries with complete disruption of posterior ring (Type C). All types have been further classified based on location and mechanism of injury (Table 2).
Comprehensive Classification
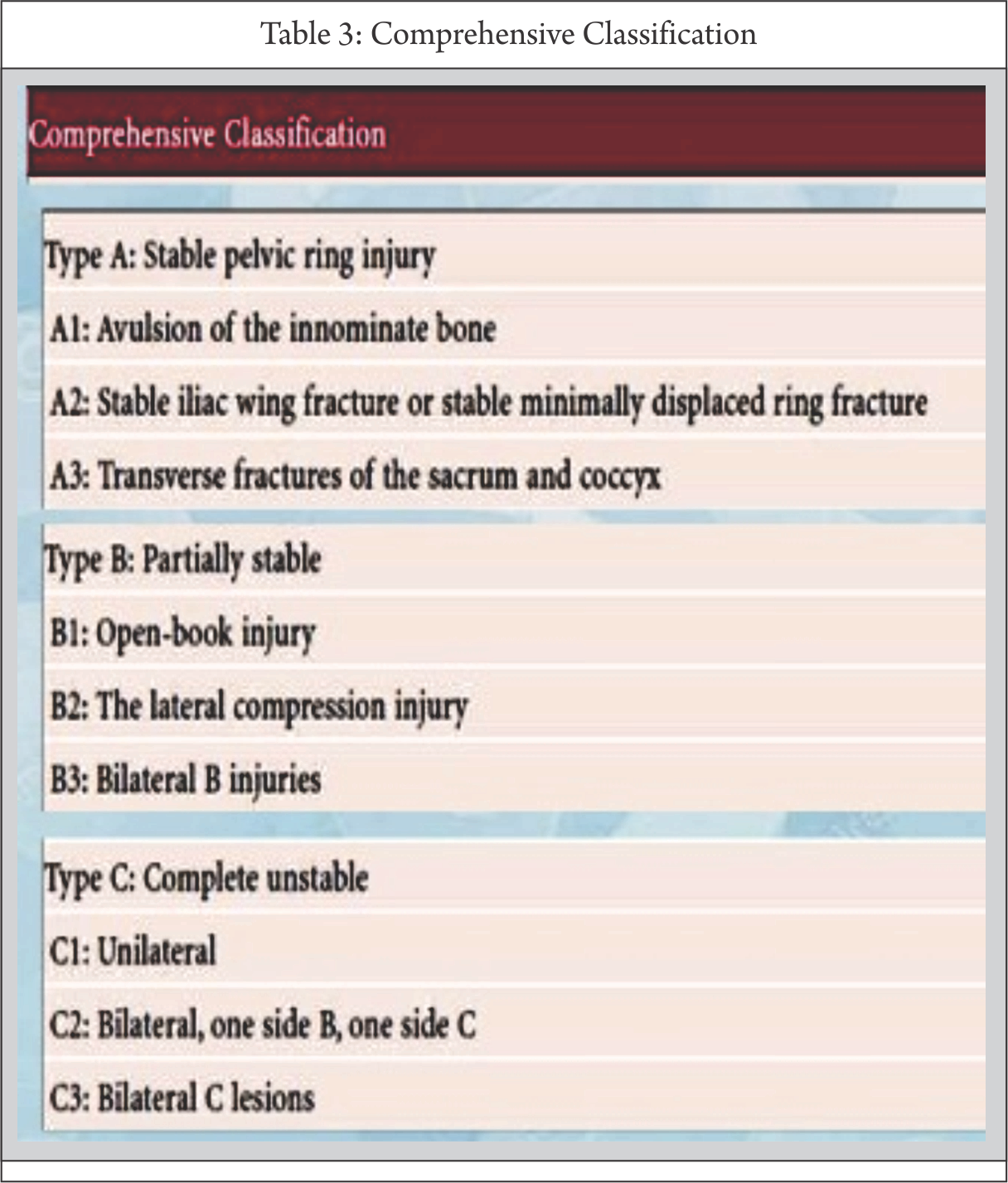
This classification of follows AO/OTA system where pelvis has been given number 6 while pelvic ring is number 1. [6] Thus pelvic ring injuries will be designated 61. Further classification in groups is based on stability which is described in context with integrity of posterior ring. Group A are stable injuries while Group B and C are partially stable and completely unstable respectively. Groups are further divided into subgroups and qualifications based on anatomical description and/or mechanism of injury (Table 3).
Classification of acetabular fractures
Letournel-Judet classification of acetabular fractures, described more than half a century ago, still remains the most commonly used system used in clinical practice.[7] Although, this anatomical classification provides useful clinical guide for approach and fixation methods for acetabular fractures, however it does not take into consideration several important factors like dislocation, impaction and communition which have significant prognostic value. To address these deficiencies, AO/OTA comprehensive classification of acetabular fractures has been developed in line with the existing system for long bone fractures.
Letournel-Judet Classification[7]
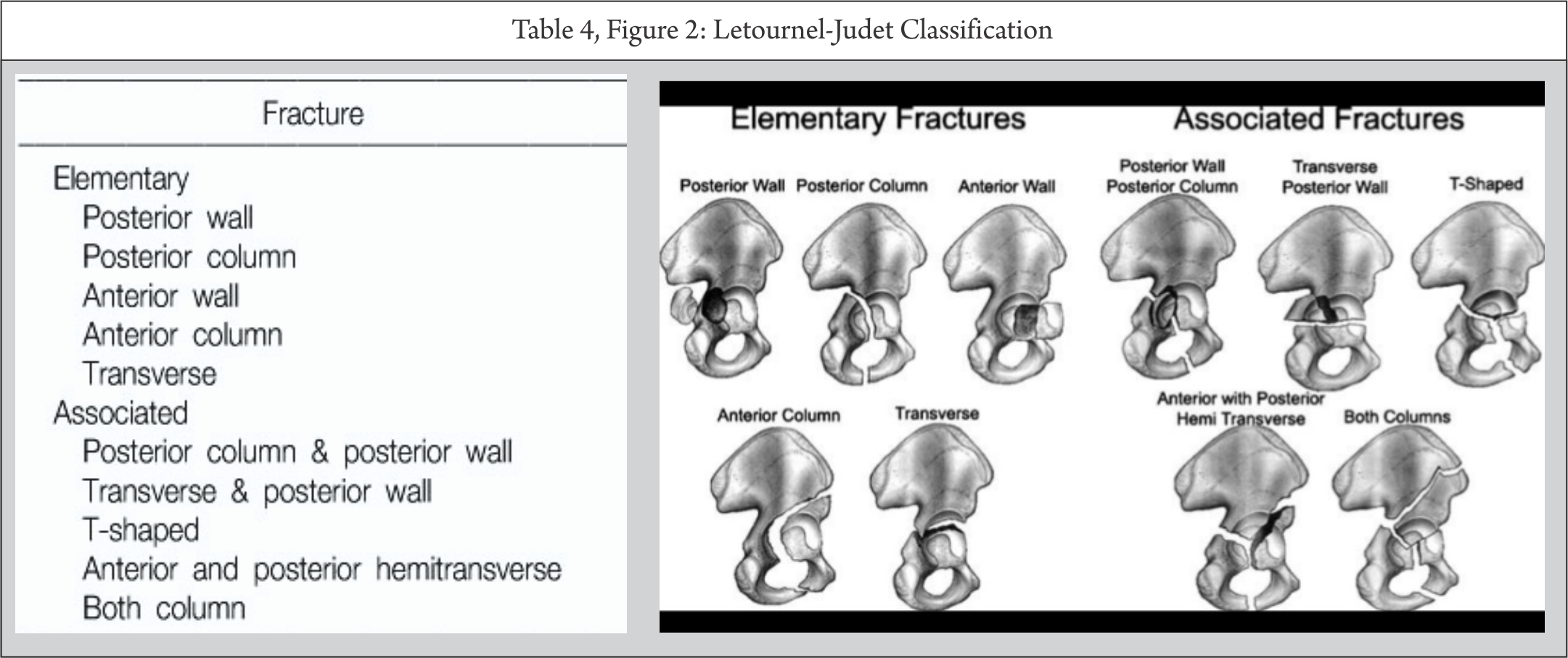
This system classifies acetabular fractures in two groups of elementary and associated fractures based on presence of one and two or more fracture lines respectively. The elementary group thus includes posterior wall, posterior column, anterior wall, anterior column and transverse fracture types, while associated group includes T-type fracture, posterior column with posterior wall, transverse with posterior wall, transverse with anterior wall or column, anterior column or wall with posterior hemitransverse and associated both column fracture. Some of the fractures types like anterior column and transverse fractures have subclassification too (Table 4, Fig. 2).
AO/OTA Comprehensive Classification
This classification essentially rearranges the Letournel-Judet classification and further accounts for important prognostic factors under subgroups. The classification broadly follows the outline of classification for periarticular long bone fractures, although it deviates from general system in order to account for complexity and two column concept of acetabular fracture. Furthermore, although this classification attempts to retain the approach of arranging fractures according to prognosis within the group, however this element is not followed throughout the classification.
The pelvis has been designated number 6 and acetabulum is number 2, thus acetabular fractures are designated by number 62. Further types are divided based on involvement of once column (Type A), both columns (Type B) or complete articular fractures (Type C). both type A and B are partial articular fractures where some part of acetabulum is still attached to axial skeleton while type C fractures are complete articular fractures where no part of acetabulum remains in continuity with axial skeleton. Type C will thus include associated both column fractures of Letournel-Judet classification.
In view of extensive use of letournel-Judet classification for clinical decision making and the fact that comprehensive system is its modification recommended for use for recording and comparing results, it is prudent to comprehend this classification while understanding the corresponding classification of comprehensive system. Thus, the following account will describe the old classification while mentioning the matching designation of AO/OTA classification.
Elementary acetabular fractures
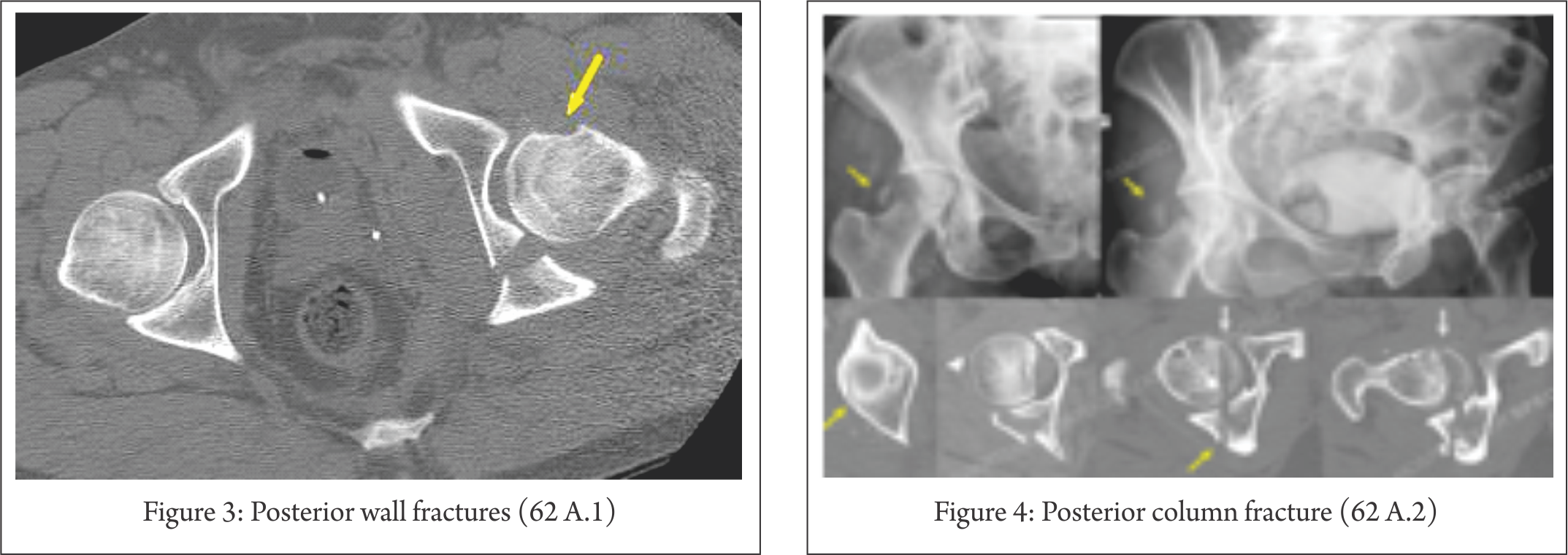
Posterior wall fractures (62 A.1)
These fractures are most common acetabular fracture (30%) and are associated with posterior hip dislocation (Fig 3) . By definition, posterior wall fractures should not involve quadrilateral plate which will make it a posterior column fracture. These fractures are further divided based on presence of single (A.1.1) or multiple fragments (A.1.2) and existence of marginal impaction (A.1.3). All three groups are further subgrouped based on location of fracture as (1) posterior; (2) posterorsuperior or (3) posterosuperior.
When associated with other fractures like transverse, T-type or both column fracture, presence of posterior wall fracture which compromises stability of hip joint essentially dictates surgical approach and reduction technique.
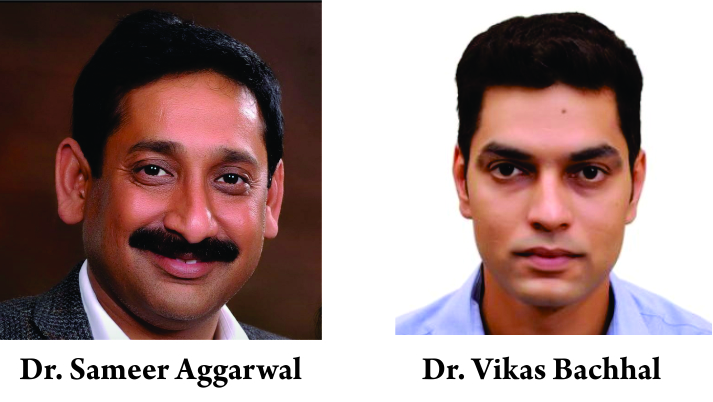
Posterior column fracture (62 A.2)
Isolated posterior fracture accounting for 3-5% cases involves separation of ischial portion of acetabulum from the rest. A fracture line runs from high up in sciatic notch across the cotyloid fossa to ischiopubic ramus (Fig. 4). These are highly unstable fractures requiring surgical intervention. Typical posterior column fractures exit at sciatic notch very close to the site where superior neurovascular bundle come in close contact with bone thereby putting them at high risk during initial injury and surgical intervention. The subgroups of this fracture includes a variant of posterior wall fracture which extends into column (it has part of quadrilateral plate attached) technically making it posterior column fracture (A.2.1). The fractured segment remains within the ischium and thus has breach of posterior rim at two places. Subgroup A.2.2 is the typical posterior column fracture starting at greater sciatic notch and exiting at ischiopubic ramus. The fractures of posterior column associated with posterior wall fractures are subgrouped as A.2.3.
Anterior partial articular fractures (62 A.3)
These fractures include anterior column/wall fractures with intact posterior column (Fig 5). Unlike posterior fractures, anterior fractures are seldom associated with hip dislocation and have significantly better prognosis. Subgroup classification differentiates anterior wall fracture (A.3.1) from anterior column fracture (A.3.2, A.3.3).
Superior pubic ramus fracture involving part of anterior wall occur frequently in pelvic ring injuries and have to be differentiated from anterior wall fractures which are very rare (1-2%).
Anterior column fractures are further divided into four subtypes depending on location of superior extent of fracture:
A.3.3
Very low: fracture exits trough rim of anterior wall.
Low: fracture exits at or below anteroinferior iliac spine (in the region of psoas fossa).
A.3.2
Intermediate: fracture exits between anteroinferior and anterosuperior iliac spines.
High: fracture exits at iliac crest.
Transverse fractures (62 B.1)
These fractures account for 5-17% of acetabular fractures where acetabulum is divided into a superior and inferior part. Direction of fracture line is variable in coronal and saggital planes (Fig. 6). Based on the level of fracture line compared to cotyloid fossa, transverse fractures are divided into three types:
Infrathecal: fracture through cotyloid fossa (B.1.1).
Juxtathecal: fracture through superior extent of cotyloid fossa (B.1.2).
Transthecal: fracture superior to cotyloid fossa and involves weight bearing dome (B.1.3).
To account for fractures with associated posterior wall fractures, modifier designated as “a” is added as follows:
a1: without posterior wall fracture
a2: with single fragment posterior wall fracture
a3: with multifragmentary posterior wall fracture
a4: with multifragmentary posterior wall fracture and marginal impaction
T-type fracture (62 B.2)
These fractures are similar to transverse variety with another vertical fracture line separating anterior and posterior segment of inferiorly. T-type fractures account for upto 7% acetabular fractures and when associated with posterior wall fracture, it carries worst prognosis of all subgroup of acetabular fractures. Posterior column with anterior hemitransverse fractures are also classified as T-type fractures.
The group classification and modifier for T-type fractures is similar to transverse variety thereby classifying them as infrathecal (B.2.1), juxtathecal (B.2.2) and transthecal (B.2.3) and all groups are further subgrouped based on location of vertical limb posterior (1), through (2) or anterior (3) to obturator foramen. A modifier “a” is added similar to transverse fractures to include associated posterior wall fracture (see above).

Anterior with posterior hemitransverse (62 B.3)
These are essentially variants of T-type fractures where anterior wall or column fracture is associated with transverse fracture in posterior half which is often undisplaced and almost always less displaced than anterior fracture. Frequently occurring in geriatric age group, these account for 7% cases of acetabular fractures. This fracture type frequently exibit marked anteromedial displacement which is significantly more than isolated anterior fractures. Furthermore, medial impaction of intact acetabular roof is often observed (gull wing sign) which imparts poorer prognosis.
These fractures are subgrouped according to type of anterior fracture as:
Anterior wall fracture (B.3.1)
High anterior column (B.3.2)
Low anterior column (B.3.3)
A modifier “a” is added to account for single (a1), two (a2) or multiple (a3) fragments of anterior segment.
Both column fracture (62 C)
These are complete articular injuries where no part of acetabulum maintains continuity with axial skeleton (floating acetabulum) (Fig. 7). Accounting for upto 23% of acetabular fractures, these are most common type of associated fracture of Letournel-Judet classification. Further group classification is based of level of anterior column fracture as high (C.1) or low (C.2) and involvement of sacroiliac joint by posterior column fracture (C.3). C.1 and C.2 are further subgrouped according to fractured segments in columns as single fragment in each segment (C.1.1 & C.2.1); two fragments in anterior segment (C.1.2 & C.2.2); and separate posterior wall fragment (C.1.3 & C.2.3). The group C.3 is subgrouped as C.3.1 with single fragment of posterior column; C.3.2 & C.3.3 with multiple fragments of posterior column with high or low anterior column respectively.
Conclusion
Fractures around hip joint are one of the most common and debilitating entities requiring intervention . These fractures encompass fractures of the pelvis and acetabulum. Health care providers must be trained and educated with scope of this problem as well as the basic types of these fractures and treatment they warrant. The clear distinction between energy levels of the injuries leading to these fractures should be understood and treatment given accordingly. This article briefly amalgamates these issues and gives pictorial examples to illustrate the specific points.
References
1. Bucholz RW, Ezaki M, Ogden JA. Injury to the acetabular triradiate physeal cartilage. J Bone Joint Surg Am. 1982 Apr;64(4):600-9.
2. Pennel GF, Davidson J, Garside H, et al. Results of treatment of acetabular fractures. Clin Orthop 1980;151:115–23.
3. Burgess AR, Eastridge BJ, Young JW, Ellison TS, Ellison PS Jr, Poka A, Bathon GH, Brumback RJ. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. 1990 Jul;30(7):848-56.
4. Tile M. Acute Pelvic Fractures: I. Causation and Classification. J Am Acad Orthop Surg. 1996 May;4(3):143-151
5. Helfet D, Tile M, Kellem J, et al. Comprehensive classification of fractures:pelvic fractures.Berne:Maurice E. Muller foundation; Fractures and fracture compendium. J Orthop Trauma 1996;10(Suppl 1):66-69
6. Müller E, ed. Comprehensive Classification of Pelvis and Acetabulum Fractures. Bern, Switzerland, Maurice E. Müller Foundation, 1995.
7. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. J Bone Joint Surg [Am] 1964;46:1615–46.
| How to Cite this article: Aggarwal S, Bachhal V. Classification of Pelvis and Acetabulum Injuries Trauma International May- August 2016;2(2):4-8. |
{kind=link}