
Management of Acetabulum Fractures – Basic Principles and Tips and Tricks
Vol 2 | Issue 2 | May – Aug 2016 | page:20-24 | Atul Patil, Ashok Shyam, Parag K Sancheti
Author: Atul Patil [1], Ashok Shyam [1], Parag K Sancheti [1]
[1] Sancheti Institute for Orthopaedic and Rehabilitation, Pune. Maharashtra, India.
Address of Correspondence
Dr. Ashok Shyam,
Sancheti Institute for Orthopaedic and Rehabilitation, Pune. Maharashtra, India.
E-mail address: drashokshyam@gmail.com
Abstract
Acetabulum fractures require systematic approach for understanding the fracture pattern and also for planning the treatment plan. The fractures have to be correctly identified radiologically and clear definition of fracture patterns should be made before planning. The radiological parameters must be kept in mind in planning of surgical approach and also the fixation method. This may require a long learning curve but these basics have to be kept in mind while dealing with acetabulum fractures. There are new techniques like 3d CT, virtual assessment of the fracture, 3D print modelling of the fractures that may help in complex fractures, but the basic principles remain the same. Advancements in technology simply refines the ways and means of interpretation and implementation of the basic principles. The current article is compilation of experience gathered over a period of time. The entire article emphasizes on the basics of understanding and managing acetabular fractures and also includes important tips and tricks that facilitate the treatment.
Keywords: Acetabulum fractures, surgical management, Letournal and judet.
Introduction
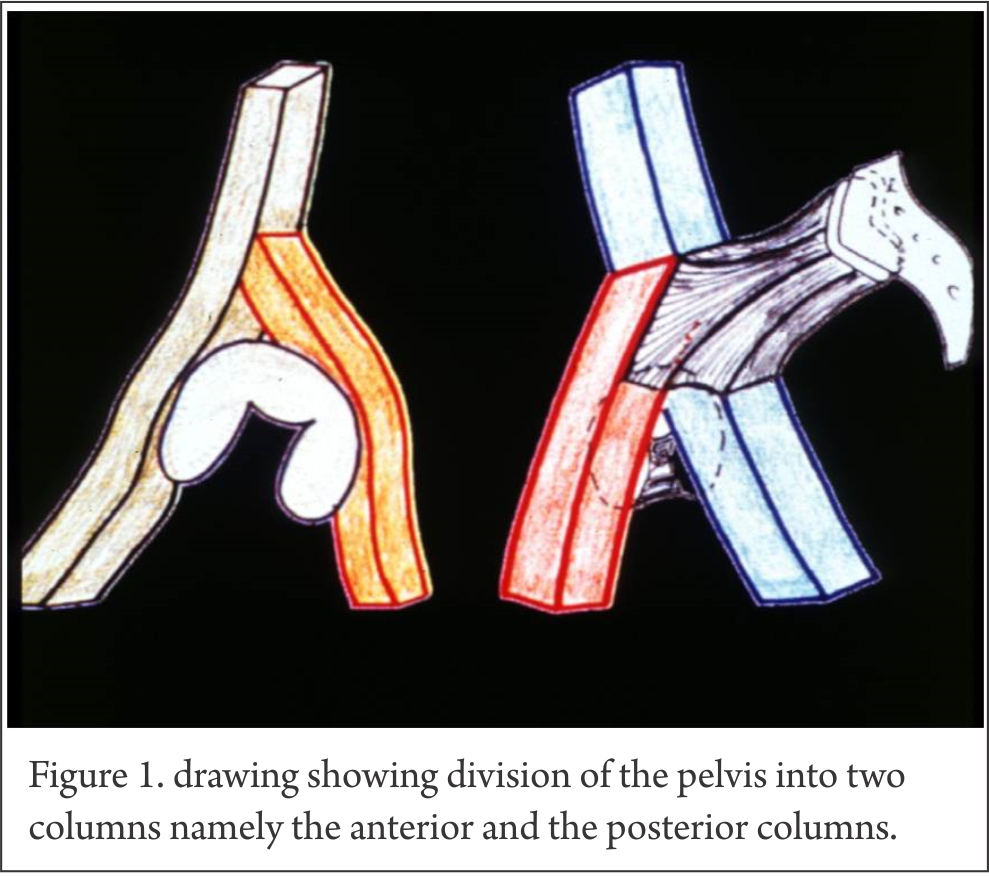
Acetabular fractures are still difficult fractures to manage and are a major challenge to treating orthopaedic surgeon [1]. Pioneering work was done by Letournal and Judet in 1964 [2]. They systematically classified acetabular fractures and developed a logical line of thinking for dealing with these fractures. They improved the understanding of morphology and popularized surgical principles for management of these injuries. Letournal and Judet put forth the two column theory of acetabulum anatomy. They envisioned acetabulum to be made of two columns. Anterior column from below the sacroiliac joint to the ischial tuberosity and posterior column from superior iliac crest to pubic symphysis with both columns attached to the sacrum by thick strut of bone lying above greater sciatic notch and called sciatic buttress [Fig. 1].
Based on these anatomical factors they suggested the first systematic classification of acetabular fractures.2 Although comprehensive classification is necessary for investigational purposes such as prognosis and outcome studies, it is less important in making decisions on individual cases. Every acetabulum fracture case is different, therefore, trying to force square plug in a round hole is counterproductive. The surgeon must know the basic fracture types, but even more important, he must be able to interpret the radiographs and draw the fracture lines on a dry skeleton. The 3d CT virtual model and 3D print life size models of fractures acetabulum also need the basic understanding of the fracture anatomy and are helpful only when such clear understanding is present. This clarity also helps in selecting the surgical approach. Most of the innovative work was performed by Letournal and Judet and their recommendation is still valid till date [2,3]. Anatomical reduction of the articular fragment and restoration of a congruent and stable hip are the two most important factors in management of acetabular fractures. Fractures reduced to less than 1 mm of articular step have less incidence of posttraumatic hip arthrosis and a better and long lasting functional restoration as compared to fractures reduced with 1 – 3 mm residual articular displacement [4,5].
To meet these goals congruent and stable hip joint, four objectives are to be kept in mind
1. Correct interpretation of the radiographs
2. Identification and understanding the fracture pattern
3. Choosing the appropriate management
4. Striving for best surgical result.
1. Correct interpretation of radiographs-
On the antero-posterior pelvis radiograph, six lines are identified: the ilioischial line, iliopectineal line, the weight bearing dome (sourcil), teardrop, anterior rim (acetabulo-obturator line), and posterior rim (ischioacetabular line) [Fig. 2].
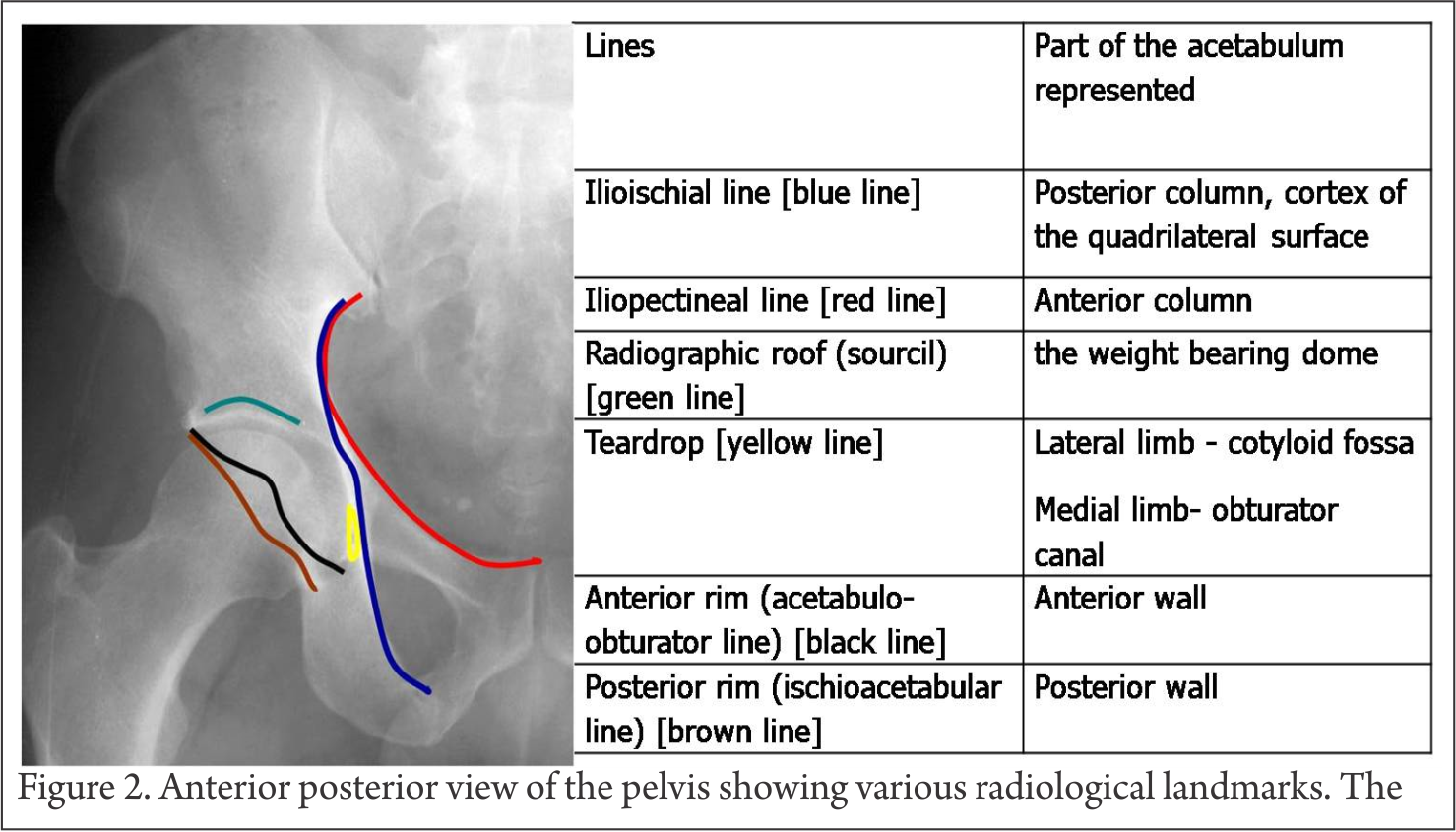
The iliopectineal line represents the anterior column. The ilioischial line is equated with the posterior column but is not actually created by the posterior border of the innominate bone but by the cortex of the quadrilateral surface. Thus fractures that disrupt the quadrilateral plate are seen as discontinuity of the ilioischial line even though these fractures do not disrupt the posterior border. The radiographic roof represents the cranial portion of the acetabular articular surface namely the weight bearing dome of the acetabulum. The lateral limb of the teardrop represents the floor of the cotyloid fossa while the medial limb represents the lateral wall of the obturator canal. Splitting of tear drop is seen when fracture line transverses through these areas. The anterior and posterior rims give some idea about the wall fractures however they are better diagnosed on Judet views.
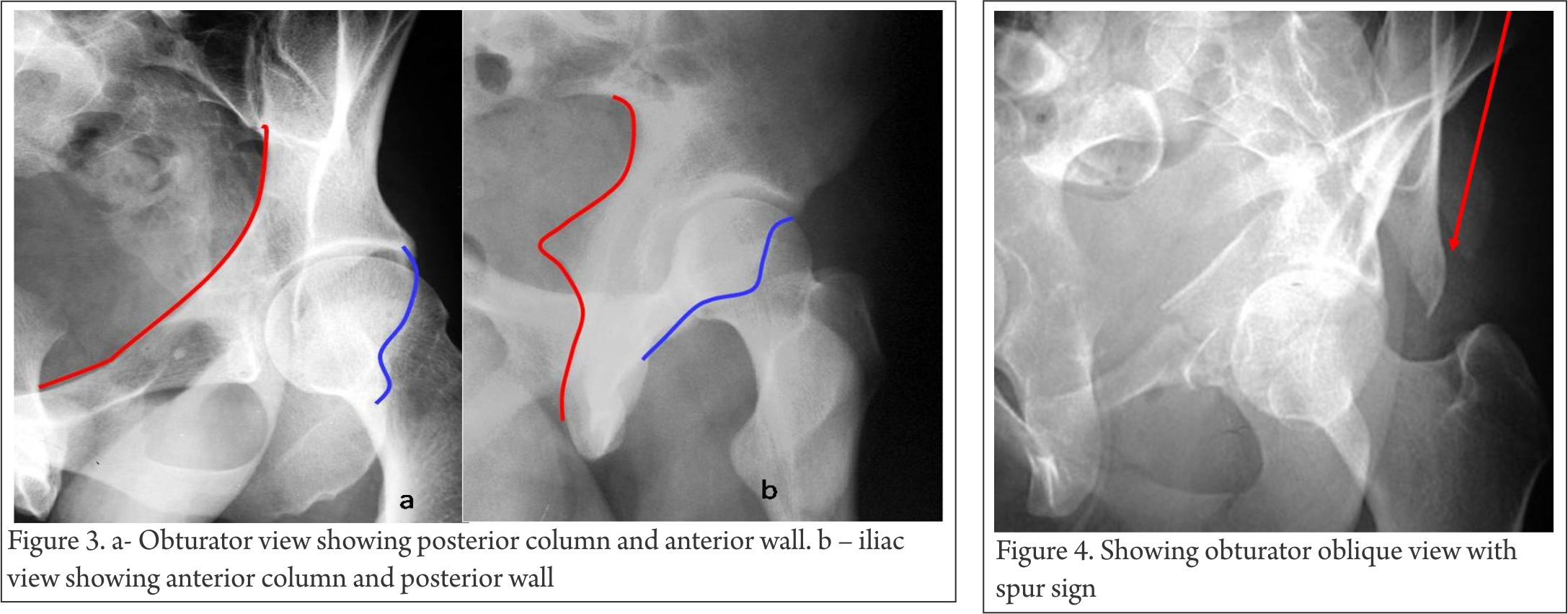
Obturator view- is taken with injured side up and pelvis tilted 45 degrees. The posterior column and the anterior wall are visualized well (Figure 3a).
Iliac view – taken with pelvis tilted 45 degrees and injured side down. The posterior column and the anterior wall are visualized well (Figure 3b).
2. Identifying and understanding the fracture pattern-
According to Brander and Marsh [6], answers to following eight questions about the radiographic observations are used to determine the acetabular fracture pattern:
A) Is a fracture of the obturator ring present? If the obturator ring is broken then the fracture is either a column type of’ fracture or a T-shaped fracture.
B) Is the ilioischial line disrupted? Disruption of the ilioischial line occurs in fractures involving the posterior column or fractures in the transverse group.
C) Is the iliopectineal line disrupted? Disruption of the iliopectineal line indicates anterior column involvement or one of the transverse-type fractures.
D) Is the iliac wing above the acetabulum fractured? Iliac wing fractures are observed in fractures involving the anterior column, anterior column with posterior hemitransverse or both column fractures.
E) Is the posterior wall fractured? Posterior wall fractures may occur in isolation or in combination with posterior column or transverse fractures.
F) Does the fracture divide acetabulum into front and back halves or front and bottom halves? T type fracture divides pelvis into top and bottom halves while a column type divides pelvis into front and back halves
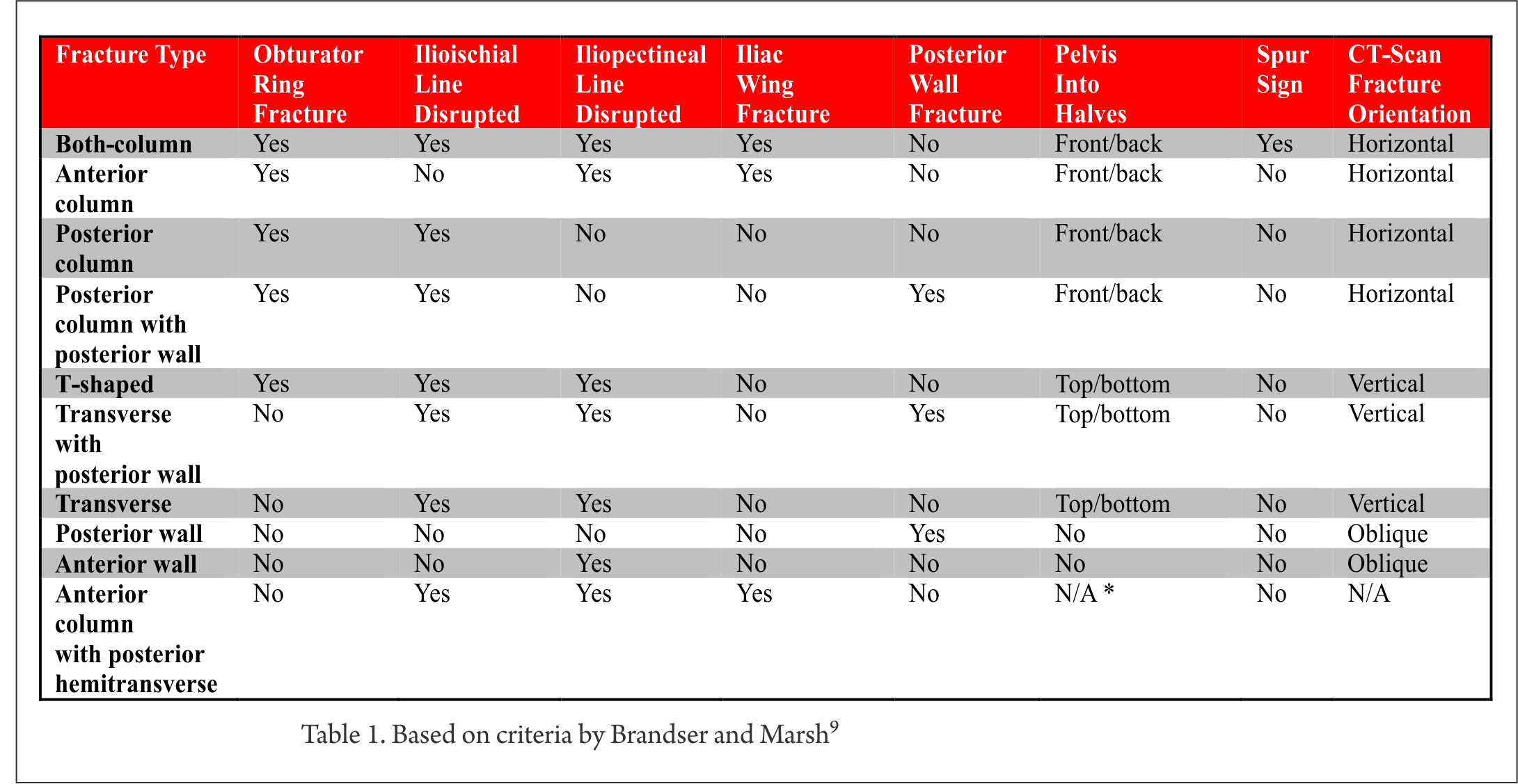
G) Is the spur sign present? The spur sign is observed exclusively in the both-column fractures. The spur is a strut of bone extending from the sacroiliac joint. Usually, this strut of bone connects to the articular surface of the acetabulum. In the both-column fracture, this connection is disrupted; a fractured piece of bone that resembles a spur remains. The spur sign is best depicted on the obturator oblique view [Fig 4]
H) What is the orientation of major fracture line on CT scan?
According to the answers of these eight questions, the fractures can be classified using Letournal and Judet classification as shown in Table 1
3. Choosing the appropriate management pathway:
Need for surgical intervention can be determined by following two criteria’s
Fracture criteria’s – Unstable hip [the femoral head and acetabulum are non congruent on AP radiograph], Roof arc angle is less than 45°, Intraarticular fragments, Marginal impaction, Unreduced fracture dislocation
Patient factors – Age [>50 yrs think of conservative treatment and later date Total Hip arthroplasty when arthritis develops], Severe co morbidities [ASA grade III or more – Cx], pre existing hip arthritis [Cx and THA later], severe osteopenia, patients with psychiatric disorders, patients with restricted pre injury mobility.
First decide whether radiograph will require surgery, and then assess the patient for feasibility of surgical intervention. If answer to any of the above question is negative the fracture is treated conservatively.
Few Tips in patient assessment –
Morel-Lavalle´lesions contain liquefied hematoma and have been known to be culture positive nearly 30-50% of times. In such cases drain the hematoma and perform delayed surgery.
Complete neurological examination and documentation is necessary especially in posterior dislocation as it is associated with high incidence of sciatic nerve injuries [20%] which if discovered later gives unsatisfactory result to the patient and may lead to legal issues.
In case the surgery is delayed, skeletal traction is essential

4. Striving for best surgical result.
This involves a definite learning curve. Surgical approach is determined based on the fracture classification. There are four main approaches used for acetabular fractures viz.
A. Kocher-Langenbeck: Posterior wall, Posterior column, Transverse, Transverse PW, Posterior column PW, T shaped [Fig 5, 6].
B. Ilioinguinal: Anterior wall, Anterior column, Anterior Posterior Hemitransverse, Both- column fractures, Transverse (rare) [Fig 7].
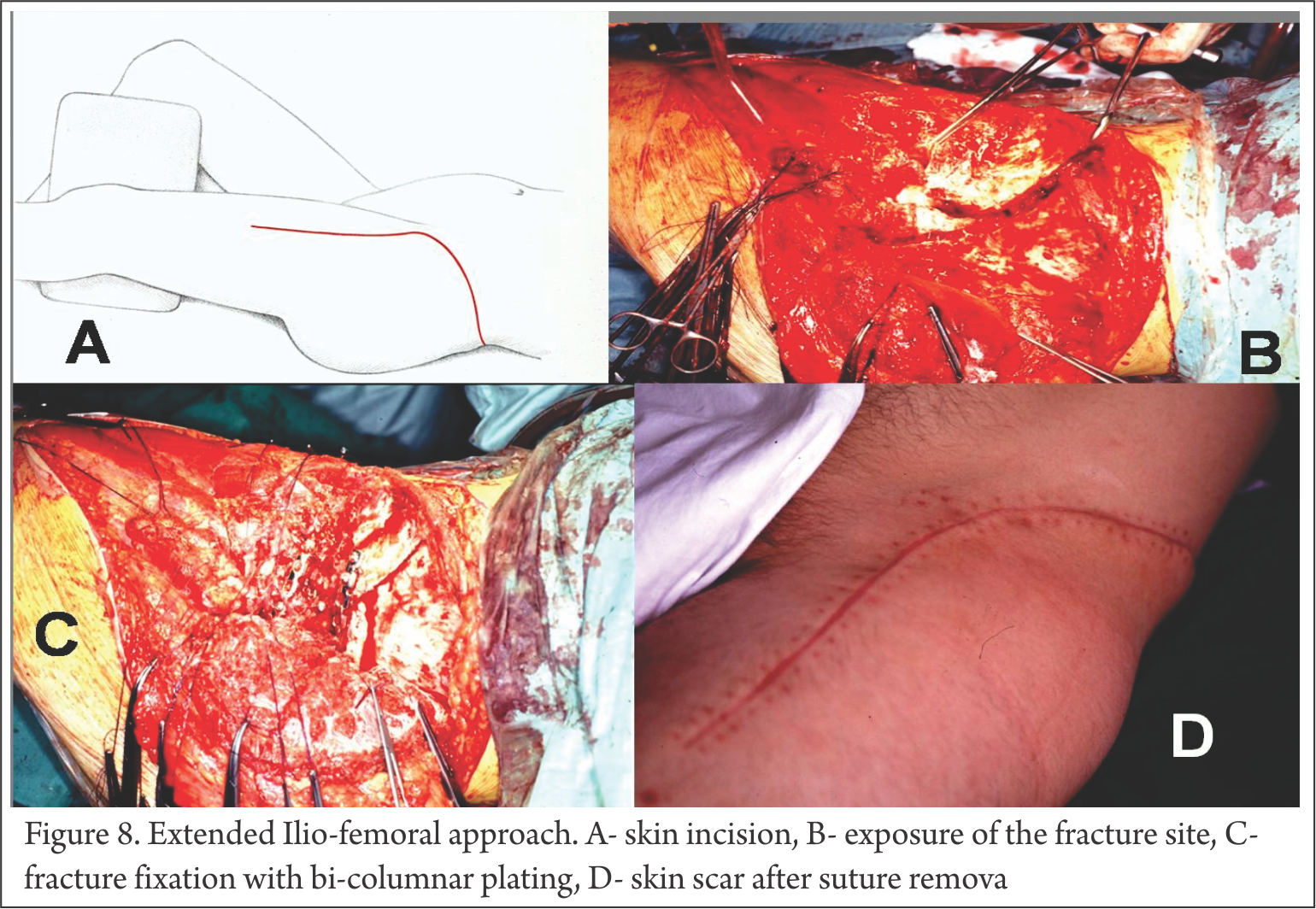
C. Extensile iliofemoral approach: Both-column fractures, T shaped, Transverse PW, Fractures > 3 weeks involving both columns [Fig 8]
D. Combined: A single approach is always preferred however combined approaches may be needed for more complex fractures involving both columns.

4. Striving for anatomical reduction.
This is by far the most important variable affecting the outcome of acetabular surgery along with severity of initial trauma. It has a long learning curve and this aspect is highlighted by Matta and Merritt in their study of their first 100 acetabular fracture fixation cases [7]. They grouped the surgical reductions chronologically in groups of 20 consecutive patients and clearly established that with increased experience the ability to achieve anatomical reduction improved along with ability to avoid unsatisfactory results.
Tips and pearls for acetabular surgery
§ Keep three points in mind – Avoid Devascularization of Fragments, remove all intra-articular fragments, and try to achieve anatomical reduction.
§ After exposure, open and clean the fracture site and get intraarticular visibility by a wide capsulotomy which will help in assessing the intraarticular reduction. Keep a low throeshold for widening the exposure
§ Special instruments in form of reduction clamps etc must be kept ready and used when necessary to hold reduction and achieve provisional K wire fixation
§ Reduction of the fragments – this will require two things – traction to the femur and opening through the fracture.
-Traction can be applied by a traction table or direct traction via a corkscrew through femoral neck or a hook on greater trochanter might work as well.
– Open the fracture by removing the major piece out of the way and appreciate the impacted fragments. These fragments have to be reduced to achieve best result.
– In cases where there is a major posterior fragment [high transverse and major T – type], a Schantz pin with a T-handle can be introduced into the ischial tuberosity to manipulate the reduction.
§ Provide stable fixation – most reliable fixation is a lag screw compression. Achieve reduction of the fracture fragments and provisionally fix them with K wires. The fragment can be predrilled first, then reduced and held with two 1.6-mm smooth Kirschner wires. Then each wire is then sequentially replaced by lag screws. This method will prevent shift/toggle of the fracture fragment while insertion of the lag screws.
§ It is desirable to have two points of fixation for each fragment, however this may not be possible because of small size although use of mini screws may be considered
§ After this a neutralization plate is applied to augment the fixation. Here one should keep in mind that lag screws should always be placed along the rim of posterior wall fragments, and care should be taken to ensure that the plate buttressing the posterior wall are positioned as lateral as possible. Applying the buttress plate too medially, especially without rim lag-screw fixation, might result in loss of stabilization of the posterior wall
§ Keep in mind two points while fixing the fractures -Avoid over-contouring of the plate, put in more lag screws rather than a bigger plate
§ In cases with bi-columnar fractures the anterior fragment is fixed with lag screw in first stage. While reducing the posterior column sometimes the anterior column screw needs to be backed out to help get the best reduction after which the screw is re-tightened.
A word of caution about the posterior approach:
The sciatic nerve must be identified and protected by knee flexion. Muscle belly of short rotators should be used to protect the nerve while retraction. Sciatic nerve may vary with respect to its relationship with pyriformis but always lies behind the quadratus muscle and is best identified by this relationship.
. Superior gluteal artery and nerve lie in the greater sciatic notch in close relationship with the bone. They can be injured while stripping of the the periosteum and can retract into the pelvis where they can bleed profusely and are difficult to handle.
. Retraction of the hip abductors might be required for visualization of superior acetabulum; however this may cause traction injury to the superior gluteal nerve which supplies the major hip abductors and the gluteus medius and minimus muscles.
Risk of iatrogenic osteonecrosis of the posterior wall fracture fragments is caused by excessive stripping of their soft-tissue attachments. Every attempt should be made to maintain the capsular attachments to these posterior wall fragments.
Recent Advances
Rapid prototyping and 3D printing are fast coming up as refined diagnostic and planning tool for acetabulum fractures [8,9]. These techniques help in visuospatial visualization of fracture fragments and also determine the best approach and fixation methods and implants. Trajectories of the lag screws can be determined on the virtual 3D models and the same can be utilized during surgery. However the role will be limited to more complex fractures and further refinement of the procedure will help in establishing its role in definitive management of acetabular fractures.
References
1. Tile M, Helfet D, Kellam J. Fractures of the Pelvis and Acetabulum. Baltimore. Lippincott Williams & Wilkins; 3rd edition, 2003.
2. Judet R, Judet J, Letournel E. Fractures of the acetabulum: Classification and surgical approaches for open reduction. J Bone Joint Surg. 1964;46A:1615-38.
3. Letournel E. Fractures of the acetabulum. A study of a series of 75 cases. 1961. Clin Orthop Relat Res 1994;(305):5-9.
4. Letournel E, Judet R. Fractures of the acetabulum, 2nd ed. Berlin: Springer-Verlag, 1993.
5. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78(11):1632-45.
6. Brandser E, Marsh JL. Acetabular fractures: easier classification with a systematic approach. AJR Am J Roentgenol. Nov 1998;171(5):1217-28.
7. Matta JM, Merritt PO: Displaced acetabular fractures, Clin Orthop Relat Res 230:83, 1988.
8. Zeng C, Xing W, Wu Z, Huang H, Huang W. A combination of three-dimensional printing and computer-assisted virtual surgical procedure for preoperative planning of acetabular fracture reduction. Injury. 2016 Oct;47(10):2223-2227.
9. Duncan JM, Nahas S, Akhtar K, Daurka J. The Use of a 3D Printer in Pre-operative Planning for a Patient Requiring Acetabular Reconstructive Surgery. J Orthop Case Rep. 2015 Jan-Mar;5(1):23-5.
| How to Cite this article: Patil A, Shyam AK, Sancheti PK. Management of Acetabulum Fractures – Basic Principles and Tips and Tricks. Trauma International May-Aug 2016;2(2):20-24. |
