Volume 2 | Issue 1 | Jan-April 2016 | Page 28-33|Puneet Maheshwari, Pramod Maheshwari
Author: Puneet Maheshwari[1], Pramod Maheshwari[1]
[1] Maheshwari Nursing Home, 163, Bhagat Singh Marg
Dewas M.P. 455001, India
Address of Correspondence
Dr. Puneet Maheshwari
Maheshwari Nursing Home, 163, Bhagat Singh Marg
Dewas M.P. 455001, India
Email: puneet1984@gmail.com
Abstract
Distal femur fractures are common but complex fractures and often are associated with complications. The cases of failure may be secondary to mechanical failure or biological failure. The current review offers overview of these complications and tips and tricks on how to manage these complications.
Keywords: Distal Femur Fractures, Complications, Surgical management
Introduction
Distal femoral fractures are a common orthopaedic problem in all age groups of patients with and incidence of about 37 per 100,000 person years.(1) Distal femoral fractures since a long time has been considered difficult to treat using traditional implants due to high failure rate and secondary varus collapse. (2)
Distal femoral fractures in young age group is most commonly due to high energy trauma while in older age group it is mostly associated with fall from height or walking along with osteoporosis of bones. Treatment of these fractures can be successfully done with variety of plates(3-6) and retrograde intramedullary nails(7-10).
Early studies of treating distal femoral fractures with locked plates reported excellent out come with non-union rates of 0-14% (mostly less than 6%) (4, 11-21).
However, with the recent data being analyzed and reported the non-union rates are now as high has 17-21% (11, 22, 23). This can be partially attributed to wider variety of fracture morphology and in patients prone for development of non-union.
Definition of Non-union
Non-union definition is based on three factors namely, duration of time since injury, characteristics of fracture on serial x-rays and lastly clinical parameters assessed by the treating surgeon.
Presently, US FDA defines non-union as fracture bone that has not completely healed in 9 months since injury and which has not shown any signs of healing over 3 consecutive months on serial x-rays.(24)
Multiple literatures indicates that optimal time for healing is in between 4 to 12 months, taking into account the type of bone fractured, nature of injury and quality of the soft tissues around the fractured bone. (25-33)
Along with these factors one more important factor is the physiologic capability of the individual in mounting a healing response.
Classification
Distal femur fractures (AO classification)
As per the AO classification the distal femur (33) can be classified in to 3 types namely extra-articular, partial articular and complete articular factures, which are further classified.
Distal femur fractures are:
Type 33A: extraarticular fracture
o A1: simple
o A2: metaphyseal wedge and/or fragmented wedge
o A3: metaphyseal complex
Type 33B: partial articular fracture
o B1: lateral condyle, sagittal
o B2: medial condyle, sagittal
o B3: frontal
Type 33C: complete articular fracture
o C1: articular simple, metaphyseal simple
o C2: articular simple, metaphyseal multifragmentary
o C3: articular multifragmentary
Weber and Cech have classified femoral non-union based on the viability or blood supply of the fracture into two broad groups viable and non-viable types. (24)
Viable type of non-union has an intact blood supply to the fracture area and thus body can mount a healing response to injury. Viable type is further divided into hypertrophic and oligo-trophic non-union.
Non-viable type of non-union is also called as atrophic or avascular non-union. The vascularity of the fracture area is absent and thus it cannot mount a healing response to injury. Type of non-union can be determined on plain x-ray in AP and lateral view or more accurately on bone scans.
Classification of non-union is important not just for documentation purposes but also for management point. In a viable non-union minimally invasive or non-invasive treatment can lead to union and thus saving the patient from another major surgical procedure.
These procedures would be give a questionable healing response in case of atrophic non-union and there the surgeon need to be more aggressive and has to plan a more extensive treatment.
Diagnosis and Evaluation
It is extremely important for the treating surgeon to timely diagnose, evaluate and document a non-union both for management as well as for legal purpose.
Diagnosis begins with a detailed history and examination of the patient and the affected limb. Patient-related risk factors like tobacco addiction, use of analgesics peripheral vascular disease, diabetes should be looked for and documented. Any clinical symptom that may point towards infection (occult/overt) like fever, malaise, night pain or history of wound healing problem should be elicited.
Physical examination should identify and document any deformity, pain over fracture area, soft tissue cover problems, increased local temperature, drainage, abnormal mobility, crepitation, and limb length discrepancy.
Radiological evaluation should be done with plain x-rays of the affected part in AP, lateral, and both oblique views (45 degrees internal and external views). In majority of patients this will get the accurate diagnosis of nonunion and its subtype. CT scan is a more accurate modality than plain x-rays in diagnosing the non-union.(34)
Infection should be cause in all cases of femoral non-union unless ruled out. Hence proper blood work-up is must which should include complete blood count, ESR and CRP. Deep tissue culture at the time of secondary surgery is the gold standard for diagnosis of infection. (35)
Causes and Risk factors
Main causes of distal femoral nonunion are
Inadequate fracture stabilization leading to motion at fracture site
Avascularity at the fracture ends – due to compound fractures, excessive stripping of soft tissue during surgery
Fracture gap
Infection
Patient related
Surgeon related
Inadequate fracture stabilization leads to micro and macro movements at the fracture site, which may result due to inadequate fixation at the time of primary surgery or due to implant failure.
Avascularity or diminished blood supply to the fracture end results due to compound injury (27), excessive stripping of soft tissue during surgery, comminuted fractures.(36) Decreased blood supply leads to a poor healing response and causes atrophic non-union.
Multiple literature supports that in fractures with significant comminution the soft tissue stripping is more and thus injuring the blood supply.(28)
Presence of gap at the fracture site either due to bone loss or during surgery (fracture fixed in distraction or debridement) also contribute to the occurrence of non-union.(29) Any gap present is usually bridged by the fracture callus, but when the body fails to bridge this gap non union results.
Infection can result as a complication of open injury or surgical treatment. Infection leads to formation of dead necrotic bone in the form of sequestrum, ingrowth of infected granulation tissue, osteolysis and motion at fracture site due to loosening of implant or implant failure.
Patient factors like age, smoking, tobacco use, chronic use of analgesics (NSAIDs), medical comorbidities and obesity to name a few can lead to non-union (22, 37).
Surgeon related factors include technical factors like plate length, screw density of plate, material of implant (titanium vs. stainless steel) and cortical reduction. Studies have shown that use of titanium implants significantly reduces the chances of non-union and thus need for a secondary surgical procedure (22).
In case of implant failure, the most important factor is the length of plate used. Shorter plates are prone to fail earlier than longer plates due to relatively lower fatigue properties because of mechanical disadvantage. Usually, a plate with 9 or more screws are is less liable to give away (37).
Treatment Options
Ultimate aim of the surgeon is to achieve osseous union without complications. Along with this it is important for the surgeon to correct any mal-alignment control infection if present, achieving sufficient muscle strength and rehabilitation.
Currently the accepted method of primary fixation of distal femur fractures is retrograde nail and lateral plating either lateral locked plates or fixed angle plates.
1. Nail dynamisation
2. Exchange nailing
3. Plate osteosynthesis
4. External fixation
5. Adjuvant treatment options
a. Electrical stimulation and ultrasound therapy
b. Bone grafting
c. Bone graft substitutes and biologic agents
d. Bone marrow infiltration
Nail Dynamisation
Nail dynamisation is the term used when the statically locked nail is converted to a dynamically locked plate. This is accomplished by removal of screw/s adjacent to the dynamic hole of the nail.
Mechanism of healing with this technique is that it allows for a controlled axial instability of the bone and implant at the fracture site. This allows transfer of weight bearing forces to non-union site and promotes healing.(38)
Dynamisation is most effective when done at an early stage of non-union or delayed union as judged by serial radiographs. Optimal time for dynamisation is around 3-6 months of injury and primary treatment.(36)
Available literature suggests a success rate of about 50%. Nail dynamisation should be done is axially stable fractures like transverse or oblique fractures.
There are few complications associated with this technique namely shortening, implant failure. Thus a regular follow-up of the patients is a must.
Exchange Nailing
Exchange nailing refers to the surgical technique where an already present nail is removed and a larger diameter and stiffer nail is inserted after reaming. It is desirable that the second nail should be atleast 1-2mm larger than the earlier nail and the reaming should be done until the osseous chatter is heard.
This method provides both mechanical and biological stimulus for healing. A larger diameter and stiffer nail provides more mechanical stability along with increased working length of the implant thus decreasing the chances of implant failure. Biologically reaming causes deposition of fresh marrow material in the non-union site and stimulates periosteal reaction.(39) Union rates reported with this technique is variable with some studies showing union rates as high as 97%. (31, 32) Studies show that chances of non-union are more when reaming is not done.(40)
Plate Osteosynthesis
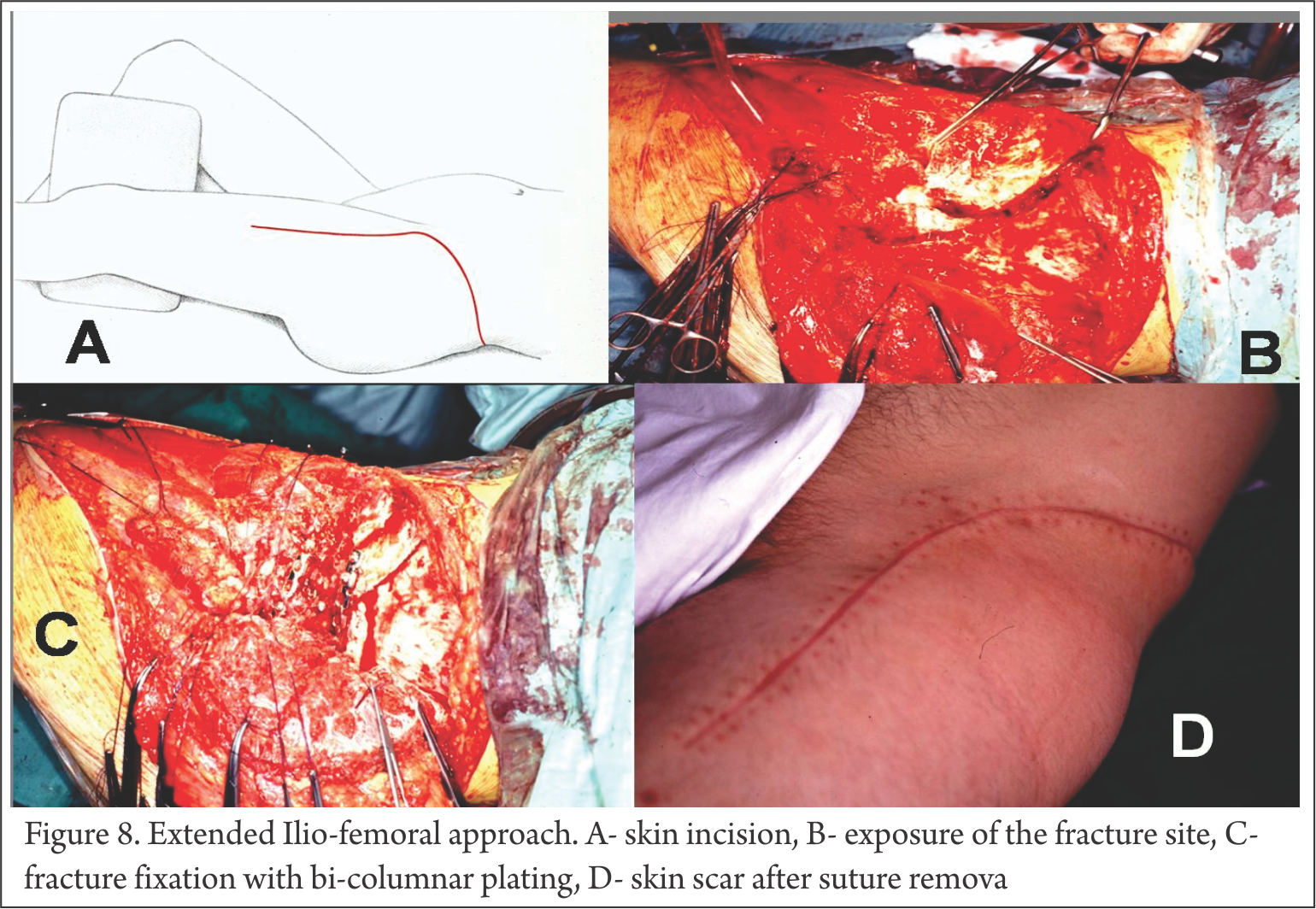
Plate osteosynthesis is the most common and gold standard treatment option in cases of distal femoral non-unions.(37) Plating offers increased mechanical stability to fracture specially in hypertrophic non-unions. Plate osteosynthesis (open reduction and internal fixation) provides an excellent opportunity of the surgeon to correct any associated deformities along with providing an excellent axial and torsional stability. Traditionally fixed angled 95 degree angled blade plate was used for distal femoral fractures, applied on the lateral aspect.(3, 41) The newer locked plates now available are the implant of choice in present scenario.(4, 5, 11-13, 15, 16, 18-20, 42, 43) With the use of compression holes excellent direct compression of the fracture site can be achieved.(44)
Few studies have reported union rates for distal femur non-unions with plate osteosynthesis around 91% to 100%.(45, 46) Even in case of poor bone stock and long standing non-unions the union rates are in range of 95 to 98% (31, 47)
This method of achieving union has its own risks and disadvantages. There is increased risk of infection, blood loss, increased tissue stripping, implant breakage, screw loosening etc. (6, 45, 47-50). Another disadvantage is that patients treated with plate osteosynthesis require strict immobilization for some duration, which may lead to joint stiffness and decreased range of motion of joints along with delay in starting rehabilitation.
Abdel-Aa et al (46) reported in their study that about 13% of patients treated with plate osteosynthesis for distal femoral non union required quadricepsplasty and knee arthrolysis within one year of surgery.
Another technique has been described in literature where both nail and plate are used simultaneously in achieving union. In this technique with an intramedullary implant in situ, a plate is fixed in compression mode at the fracture site. This method provides positive points of both the techniques in the form of early weight bearing, fracture fixed in direct compression thus chances of early union, improved torsional and rotational stability. If required bone grafting can also be done at same time to further increase the osteogenic potential and to fill up any bony defects if present. In studies using this method there has been a union rate of 100% within one year of surgery.(49, 51, 52)
External Fixation
Multiplanar (Ilizarov technique) and uniplanar external fixation for treatment of non-union of femur has been reported in literature with modest success (53, 54). Compression and distraction at non-union site has been demonstrated to show signs of healing(55). However, with the high complication rate (eg osteomyletitis, severe pain requiring opiod anagesics, septic arthritis, pin failure, joint stiffness etc.) use of external fixation for non-union healing is restricted to small number of patients. Along with this, the technical complexity and cost factor also restricts its use to tertiary level centres (54).
Adjuvant Treatment
These treatment options can be used as an isolated treatment option or as a supplementary treatment for achieving union.
Electrical Stimulation
Multiple studies show that mechanical forces, electrical forces, magnetic forces and ultrasound waves have variable level of effect on bone healing and growth (56-59). Electrical stimulation is thought to be effective non-invasive modality for promoting fracture healing and in treatment of non-unions.
Generation of electrical potentials around bone occurs when mechanical stress is applied(60, 61). Electronegative and electropositive potentials are generated with compression and tension respectively (62). It has been proven that in electronegative potential bone growth occurs and with electropositive potential bone is resorbed (63).
There are three techniques of electrical stimulation, namely, direct electric current, capacitive coupling and inductive coupling.
Direct electrical current is an invasive technique involving one or more cathode electrodes being implanted in the bone and an anode usually placed on the skin over the fracture site(64). In a case series by Brighton et al. (65) out of 168 fractures, 76% showed good bony union by 12 weeks of electrical stimulation therapy.
Capacitive coupling is a noninvasive technique where two electrodes are placed over the skin such that fracture site lies in between the electrodes. Here alternating current (AC) is used and an electric field is generated in and around the fracture site. It is a dose dependent technique whereby the greater electrical field leads to more osteoblastic cell response along with increased time of exposure leading to increased osteoblastic cell proliferation (66, 67).
Inductive coupling uses the principle of Pulsed Electromagnetic Field (PEMF) generation using specific device. The device is placed over the skin (non-invasive) over the fracture site. Passing current in the device generates the magnetic field. This magnetic field induces an electrical field, which leads to a bone healing response. This time-varying electrical field simulates normal response of osteoblastic cells to mechanical stimuli (68).
Bone Grafting, bone marrow aspirate and biologic agents
These procedures and materials can be used as an isolated or adjuvant treatment depending of the non-union type.
Autogenous bone grafts are considered gold standard for grafting procedures(69). Autologous bone grafting in past has got a bad review mainly due to donor site complications(70). With advances in harvesting techniques there is a renewed interest in this procedure(71-73).
Biologic agents like Bone Morphogenic Proteins (BMP) have been studied in detail both in animals and in humans and gives promising results.
Bone Morphogenic Proteins are part of the Transforming Growth Factor-Beta (TGF-B) superfamily and with a cascade sequence of events leads to bone healing via chondrogenesis, osteogenesis, angiogenesis and extracellular matrix remodeling (74). There are more than 20 BMP identified in humans. Studies in animals and in-vitro have shown BMP -2,4,6,7,9 have high osteogenic potential (75-78). Recombinant BMP-2 and 4 are in use clinically (74) but with questionable safety and efficacy profile(79-82).
Summary
Every surgically managed fracture is a race between bony union and implant/biological failure leading to non-union. Management of acute distal femur fracture with a nail or plate has good union rate or more than 90%. But when non-union occurs, it becomes a challenging task for the surgeon and patient both. It presents a significant mental, emotional and financial implication on the patient and his/her family.
Careful history taking and meticulous examination during routine follow-ups can help a surgeon to diagnose a delayed union or non-union in early stage and can modify the management as per the need to achieve bony union. Established non-union requires a well planned out management protocol to be decided before hand. Surgeon should decide the management plan (either non-invasive or invasive) on case-to-case basis to achieve union, correction of deformities. Surgeon should also take care of the patient modifiable risk factors like use of NSAIDs, smoking, medical co-morbidities and nutritional status of patient.
References
1. Zlowodzki M, Bhandari M, Marek DJ, Cole PA, Kregor PJ. Operative treatment of acute distal femur fractures: systematic review of 2 comparative studies and 45 case series (1989 to 2005). J Orthop Trauma. 2006;20(5):366-71.
2. Davison BL. Varus collapse of comminuted distal femur fractures after open reduction and internal fixation with a lateral condylar buttress plate. American journal of orthopedics. 2003;32(1):27-30.
3. Merchan ECR, Maestu PR, Blanco RP. Blade-Plating of Closed Displaced Supracondylar Fractures of the Distal Femur with the AO System. The Journal of Trauma: Injury, Infection, and Critical Care. 1992;32(2):174-8.
4. Haidukewych G. Results of Polyaxial Locked-Plate Fixation of Periarticular Fractures of the Knee. The Journal of Bone and Joint Surgery (American). 2007;89(3):614.
5. Kregor PJ, Stannard JA, Zlowodzki M, Cole PA. Treatment of Distal Femur Fractures Using the Less Invasive Stabilization System. Journal of Orthopaedic Trauma. 2004;18(8):509-20.
6. Vallier HA, Hennessey TA, Sontich JK, Patterson BM. Failure of LCP Condylar Plate Fixation in the Distal Part of the Femur: A Report of Six Cases. The Journal of Bone & Joint Surgery. 2006;88(4):846-53.
7. Thomson AB, Driver R, Kregor PJ, Obremskey WT. Long-Term Functional Outcomes After Intra-Articular Distal Femur Fractures: Orif Versus Retrograde Intramedullary Nailing. Orthopedics. 2008;31(8):748-50.
8. Handolin L, Pajarinen J, Lindahl J, Hirvensalo E. Retrograde intramedullary nailing in distal femoral fractures—results in a series of 46 consecutive operations. Injury. 2004;35(5):517-22.
9. Hartin NL, Harris I, Hazratwala K. RETROGRADE NAILING VERSUS FIXED-ANGLE BLADE PLATING FOR SUPRACONDYLAR FEMORAL FRACTURES: A RANDOMIZED CONTROLLED TRIAL. ANZ J Surg. 2006;76(5):290-4.
10. Singh SK, El-Gendy KA, Chikkamuniyappa C, Houshian S. The retrograde nail for distal femoral fractures in the elderly: High failure rate of the condyle screw and nut. Injury. 2006;37(10):1004-10.
11. Syed AA, Agarwal M, Giannoudis PV, Matthews SJE, Smith RM. Distal femoral fractures: long-term outcome following stabilisation with the LISS. Injury. 2004;35(6):599-607.
12. Ricci AR, Yue JJ, Taffet R, Catalano JB, DeFalco RA, Wilkens KJ. Less Invasive Stabilization System for treatment of distal femur fractures. American journal of orthopedics. 2004;33(5):250-5.
13. Fankhauser F, Gruber G, Schippinger G, Boldin C, Hofer H, Grechenig W, et al. Minimal-invasive treatment of distal femoral fractures with the LISS (Less Invasive Stabilization System) A prospective study of 30 fractures with a follow up of 20 months. Acta Orthopaedica. 2004;75(1):56-60.
14. Schutz M, Muller M, Kaab M, Haas N. Less invasive stabilization system (LISS) in the treatment of distal femoral fractures. Acta chirurgiae orthopaedicae et traumatologiae Cechoslovaca. 2003;70(2):74-82.
15. Schütz M, Müller M, Regazzoni P, Höntzsch D, Krettek C, Van der Werken C, et al. Use of the Less Invasive Stabilization System (LISS) in patients with distal femoral (AO33) fractures: a prospective multicenter study. Arch Orthop Trauma Surg. 2005;125(2):102-8.
16. Weight M, Collinge C. Early Results of the Less Invasive Stabilization System for Mechanically Unstable Fractures of the Distal Femur (AO/OTA Types A2, A3, C2, and C3). Journal of Orthopaedic Trauma. 2004;18(8):503-8.
17. Wong M-K, Leung F, Chow SP. Treatment of distal femoral fractures in the elderly using a less-invasive plating technique. International Orthopaedics (SICOT). 2005;29(2):117-20.
18. Ricci WM, Loftus T, Cox C, Borrelli J. Locked Plates Combined With Minimally Invasive Insertion Technique for the Treatment of Periprosthetic Supracondylar Femur Fractures Above a Total Knee Arthroplasty. Journal of Orthopaedic Trauma. 2006;20(3):190-6.
19. Kolb W, Guhlmann H, Windisch C, Marx F, Kolb K, Koller H. Fixation of Distal Femoral Fractures With the Less Invasive Stabilization System: A Minimally Invasive Treatment With Locked Fixed-Angle Screws. The Journal of Trauma: Injury, Infection, and Critical Care. 2008;65(6):1425-34.
20. Kao FC, Tu YK, Su JY, Hsu KY, Wu CH, Chou MC. Treatment of Distal Femoral Fracture by Minimally Invasive Percutaneous Plate Osteosynthesis: Comparison Between the Dynamic Condylar Screw and the Less Invasive Stabilization System. The Journal of Trauma: Injury, Infection, and Critical Care. 2009;67(4):719-26.
21. Fulkerson E, Tejwani N, Stuchin S, Egol K. Management of periprosthetic femur fractures with a first generation locking plate. Injury. 2007;38(8):965-72.
22. Rodriguez EK, Boulton C, Weaver MJ, Herder LM, Morgan JH, Chacko AT, et al. Predictive factors of distal femoral fracture nonunion after lateral locked plating: a retrospective multicenter case-control study of 283 fractures. Injury. 2014;45(3):554-9.
23. Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh JL. Locking Plates for Distal Femur Fractures: Is There a Problem With Fracture Healing? Journal of Orthopaedic Trauma. 2011;25:S8-S14.
24. Brinker MR. Nonunions: Evaluation and Treatment. In: Trafton PG, editor. Skeletal Trauma: Basic Science, Management, and Reconstruction. 3 ed. Philadelphia: W.B. Saunders; 2003. p. 507-604.
25. Furlong AJ, Giannoudis PV, DeBoer P, Matthews SJ, MacDonald DA, Smith RM. Exchange nailing for femoral shaft aseptic non-union. Injury. 1999;30(4):245-9.
26. Giannoudis PV, MacDonald DA, Matthews SJ, Smith RM, Furlong AJ, De Boer P. Nonunion of the femoral diaphysis. The Journal of Bone and Joint Surgery. 2000;82(5):655-8.
27. Malik MH, Harwood P, Diggle P, Khan SA. Factors affecting rates of infection and nonunion in intramedullary nailing. The Journal of bone and joint surgery British volume. 2004;86(4):556-60.
28. Noumi T, Yokoyama K, Ohtsuka H, Nakamura K, Itoman M. Intramedullary nailing for open fractures of the femoral shaft: evaluation of contributing factors on deep infection and nonunion using multivariate analysis. Injury. 2005;36(9):1085-93.
29. Pihlajamäki HK, Salminen ST, Böstman OM. The Treatment of Nonunions Following Intramedullary Nailing of Femoral Shaft Fractures. Journal of Orthopaedic Trauma. 2002;16(6):394-402.
30. Wu C-C. The Effect of Dynamization on Slowing the Healing of Femur Shaft Fractures after Interlocking Nailing. The Journal of Trauma: Injury, Infection, and Critical Care. 1997;43(2):263-7.
31. Kempf I, Grosse A, Rigaut P. The Treatment of Noninfected Pseudarthrosis of the Femur and Tibia with Locked Intramedullary Nailing. Clinical Orthopaedics and Related Research. 1986;&NA;(212):142???54.
32. Webb LX, Winquist RA, Hansen ST. Intramedullary Nailing and Reaming for Delayed Union or Nonunion of the Femoral Shaft. Clinical Orthopaedics and Related Research. 1986;&NA;(212):133???41.
33. Weresh MJ, Hakanson R, Stover MD, Sims SH, Kellam JF, Bosse MJ. Failure of Exchange Reamed Intramedullary Nails for Ununited Femoral Shaft Fractures. Journal of Orthopaedic Trauma. 2000;14(5):335-8.
34. Bhattacharyya T, Bouchard KA, Phadke A, Meigs JB, Kassarjian A, Salamipour H. The Accuracy of Computed Tomography for the Diagnosis of Tibial Nonunion. The Journal of Bone & Joint Surgery. 2006;88(4):692-7.
35. Gristina AG, Naylor PT, Webb LX. Molecular mechanisms in musculoskeletal sepsis: the race for the surface. Instructional course lectures. 1990;39:471-82.
36. Lynch JR, Taitsman LA, Barei DP, Nork SE. Femoral Nonunion: Risk Factors and Treatment Options. J Am Acad Orthop Surg. 2008;16(2):88-97.
37. Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ. Risk Factors for Failure of Locked Plate Fixation of Distal Femur Fractures. Journal of Orthopaedic Trauma. 2014;28(2):83-9.
38. Yokota H, Tanaka SM. Osteogenic potentials with joint-loading modality. J Bone Miner Metab. 2005;23(4):302-8.
39. Reichert ILH, McCarthy ID, Hughes SPF. The Acute Hemodynamic Response to Intramedullary Reaming of the Intact and Osteotomized Tibia: An Experimental Investigation with Radiolabeled Microspheres in the Ovine Tibia. Techniques in Orthopaedics. 1996;11(1):28-34.
40. Society COT. Nonunion following intramedullary nailing of the femur with and without reaming: Results of amulticenter randomized clinical trial. The Journal of bone and joint surgery American volume. 2003;85-A(11):2093-6.
41. Bolhofner BR, Carmen B, Clifford P. The Results of Open Reduction and Internal Fixation of Distal Femur Fractures Using a Biologic (Indirect) Reduction Technique. Journal of Orthopaedic Trauma. 1996;10(6):372-7.
42. Kayali C, Agus H, Turgut A. Successful results of minimally invasive surgery for comminuted supracondylar femoral fractures with LISS: comparative study of multiply injured and isolated femoral fractures. Journal of Orthopaedic Science. 2007;12(5):458-65.
43. Liu F, Tao R, Cao Y, Wang Y, Zhou Z, Wang H, et al. The role of LISS (less invasive stabilisation system) in the treatment of peri-knee fractures. Injury. 2009;40(11):1187-94.
44. Meyer RW, Plaxton NA, Postak PD, Gilmore A, Froimson MI, Greenwald AS. Mechanical Comparison of a Distal Femoral Side Plate and a Retrograde Intramedullary Nail. Journal of Orthopaedic Trauma. 2000;14(6):398-404.
45. Bellabarba C, Ricci WM, Bolhofner BR. Results of Indirect Reduction and Plating of Femoral Shaft Nonunions After Intramedullary Nailing. Journal of Orthopaedic Trauma. 2001;15(4):254-63.
46. Abdel-Aa AM, Farouk OA, Elsayed A, Said HG. The Use of a Locked Plate in the Treatment of Ununited Femoral Shaft Fractures. The Journal of Trauma: Injury, Infection, and Critical Care. 2004;57(4):832-6.
47. Ring D, Jupiter JB, Sanders RA, Quintero J, Santoro VM, Ganz R, et al. Complex Nonunion Of Fractures Of The Femoral Shaft Treated By Wave-plate Osteosynthesis. The Journal of Bone and Joint Surgery. 1997;79(2):289-94.
48. Rozbruch RS, M??ller U, Gautier E, Ganz R. The Evolution of Femoral Shaft Plating Technique. Clinical Orthopaedics and Related Research. 1998;354:195-208.
49. Ueng SWN, Chao E-K, Lee S-S, Shih C-H. Augmentative Plate Fixation for the Management of Femoral Nonunion after Intramedullary Nailing. The Journal of Trauma: Injury, Infection, and Critical Care. 1997;43(4):640-4.
50. Cove JA, Lhowe DW, Jupiter JB, Siliski JM. The Management of Femoral Diaphyseal Nonunions. Journal of Orthopaedic Trauma. 1997;11(7):513-20.
51. Ueng SWN, Shih C-H. Augmentative Plate Fixation for the Management of Femoral Nonunion with Broken Interlocking Nail. The Journal of Trauma: Injury, Infection, and Critical Care. 1998;45(4):747-52.
52. Choi YS, Kim KS. Plate augmentation leaving the nail in situ and bone grafting for non-union of femoral shaft fractures. Int Orthop. 2005;29(5):287-90.
53. Brinker MR, O’Connor DP. Ilizarov Compression Over a Nail for Aseptic Femoral Nonunions That Have Failed Exchange Nailing: A Report of Five Cases. Journal of Orthopaedic Trauma. 2003;17(10):668-76.
54. Patil S. Management of complex tibial and femoral nonunion using the Ilizarov technique, and its cost implications. Journal of Bone and Joint Surgery – British Volume. 2006;88-B(7):928-32.
55. Inan M, Karaoglu S, Cilli F, Turk CY, Harma A. Treatment of Femoral Nonunions by Using Cyclic Compression and Distraction. Clinical Orthopaedics and Related Research. 2005;&NA;(436):222-8.
56. Fukada E, Yasuda I. On the Piezoelectric Effect of Bone. Journal of the Physical Society of Japan. 1957;12(10):1158-62.
57. Duarte LR. The stimulation of bone growth by ultrasound. Archives of Orthopaedic and Traumatic Surgery. 1983;101(3):153-9.
58. Kenwright AGaJ. The influence of induced micromovement upon the healing of experimental tibial fractures. Bone & Joint Journal. 1985;67-B:650-5.
59. Valchanou VD, Michailov P. High energy shock waves in the treatment of delayed and nonunion of fractures. International Orthopaedics. 1991;15(3).
60. Becker RO, Bassett, C.A.L., Bachman, C.H. Bioelectric factors controlling bone structure. In: Frost H, editor. Bone biodynamics. Boston: Little, Brown & Company; 1964. p. 209–32.
61. Yasuda I. Fundamental aspects of fracture treatment. J Kyoto Med SOC. 1953;4:392.
62. Otter M, Goheen S, Williams WS. Streaming potentials in chemically modified bone. Journal of Orthopaedic Research. 1988;6(3):346-59.
63. Rubinacci A, Black J, Brighton CT, Friedenberg ZB. Changes in bioelectric potentials on bone associated with direct current stimulation of osteogenesis. Journal of Orthopaedic Research. 1988;6(3):335-45.
64. Black J. Electrical Stimulation: Its Role in Growth, Repair, and Remodeling of the Musculoskeletal
System. New York: Praeger; 1987.
65. Brighton CT, Black J, Friedenberg ZB, Esterhai JL, Day LJ, Connolly JF. A multicenter study of the treatment of non-union with constant direct current. The Journal of bone and joint surgery American volume. 1981;63(1):2-13.
66. Korenstein R, Somjen D, Fischler H, Binderman I. Capacitative pulsed electric stimulation of bone cells. Induction of cyclic-AMP changes and DNA synthesis. Biochimica et Biophysica Acta (BBA) – Molecular Cell Research. 1984;803(4):302-7.
67. Wang Z. Up-Regulation of Bone Morphogenetic Proteins in Cultured Murine Bone Cells with Use of Specific Electric Fields. The Journal of Bone and Joint Surgery (American). 2006;88(5):1053.
68. Nelson FR, Brighton CT, Ryaby J, Simon BJ, Nielson JH, Lorich DG, et al. Use of physical forces in bone healing. J Am Acad Orthop Surg. 2003;11(5):344-54.
69. Giannoudis PV, Dinopoulos HT. Autologous bone graft: when shall we add growth factors? Foot Ankle Clin. 2010;15(4):597-609.
70. Oakley MJ, Smith WR, Morgan SJ, Ziran NM, Ziran BH. Repetitive posterior iliac crest autograft harvest resulting in an unstable pelvic fracture and infected non-union: case report and review of the literature. Patient Saf Surg. 2007;1(1):6.
71. Newman JT, Stahel PF, Smith WR, Resende GV, Hak DJ, Morgan SJ. A New Minimally Invasive Technique for Large Volume Bone Graft Harvest for Treatment of Fracture Nonunions. Orthopedics. 2008;31(3):257-61.
72. Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: A systematic review. Injury. 2011;42:S3-S15.
73. Herscovici JD, Scaduto JM. Use of the reamer-irrigator-aspirator technique to obtain autograft for ankle and hindfoot arthrodesis. The bone & joint journal. 2012;94-B(1):75-9.
74. Lissenberg-Thunnissen SN, de Gorter DJ, Sier CF, Schipper IB. Use and efficacy of bone morphogenetic proteins in fracture healing. Int Orthop. 2011;35(9):1271-80.
75. Xiang L, Liang C, Zhen-Yong K, Liang-Jun Y, Zhong-Liang D. BMP9-induced osteogenetic differentiation and bone formation of muscle-derived stem cells. J Biomed Biotechnol. 2012;2012:610952.
76. Kang Q, Sun MH, Cheng H, Peng Y, Montag AG, Deyrup AT, et al. Characterization of the distinct orthotopic bone-forming activity of 14 BMPs using recombinant adenovirus-mediated gene delivery. Gene Ther. 2004;11(17):1312-20.
77. Luu HH, Song WX, Luo X, Manning D, Luo J, Deng ZL, et al. Distinct roles of bone morphogenetic proteins in osteogenic differentiation of mesenchymal stem cells. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2007;25(5):665-77.
78. Cheng H, Jiang W, Phillips FM, Haydon RC, Peng Y, Zhou L, et al. Osteogenic activity of the fourteen types of human bone morphogenetic proteins (BMPs). Urologic Oncology: Seminars and Original Investigations. 2004;22(1):79-80.
79. Burks MV, Nair L. Long-Term Effects of Bone Morphogenetic Protein- Based Treatments in Humans. Journal of Long-Term Effects of Medical Implants. 2010;20(4):277-93.
80. Carragee EJ, Hurwitz EL, Weiner BK. A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned. Spine J. 2011;11(6):471-91.
81. Carragee EJ, Ghanayem AJ, Weiner BK, Rothman DJ, Bono CM. A challenge to integrity in spine publications: years of living dangerously with the promotion of bone growth factors. Spine J. 2011;11(6):463-8.
82. Mroz TE, Wang JC, Hashimoto R, Norvell DC. Complications related to osteobiologics use in spine surgery: a systematic review. Spine (Phila Pa 1976). 2010;35(9 Suppl):S86-104.
How to Cite this article: Maheshwari P, Maheshwari P. Non Union Distal Femur Fracture: Causes and Management Options. Trauma International Jan-Apr 2016;1(2):28-33.
|

Dr. Pramod Maheshwari

Dr. Puneet Maheshwari