
Terrorist Bomb Blasts: Emergency department management of multiple incidents
Vol 1 | Issue 1 | July – Sep 2015 | page: 36-40 | Muhammad Saeed Minhas[1], Kashif Mahmood[1], Jahanzeb Effendi[1], Ranjeet Kumar[1], Anisuddin Bhatti[1]
Author: Muhammad Saeed Minhas[1], Kashif Mahmood[1], Jahanzeb Effendi[1], Ranjeet Kumar[1], Anisuddin Bhatti[1]
[1] Jinnah Post Graduate Medical center, Karachi, Pakistan.
Address of Correspondence
Dr Muhammad Saeed Minhas.
Associate Professor Orhopaedics, Jinnah Post Graduate Medical center, Karachi, Pakistan.
Email: orthominhas@hotmail.com
Abstract
Objective: To assess the preparedness of the hospital emergency system and medical personnel’s in dealing trauma victims of terrorist bomb blasts in Accident and Emergency.
Patients and Methods: Four major terrorist bomb blasts incidents occurred in Karachi from December 2012 to May 2014. All patients of these 4 incidents were brought to Accident and emergency of Jinnah Postgraduate Medical Center. Place and type of bomb blast, their initial search and rescue, transfer and transportation noted. Data collected of these patients at Accident and emergency of Jinnah Post Graduate Medical Center, regarding triage, primary and secondary survey with adjuncts performed. Data was also collected from emergency operation theatres, Intensive care unit and admissions in wards. Time taken for early and effective management and disposal to different departments noted.
Results: Total victims of these four bomb blast incidents were 179. Nineteen were brought dead, 8 more died within two hours, due to multiple system involvement which made total deaths 27 (15%). The patients were triaged with color coding, 44% of these patients were red and yellow, and 41% patients were of minor injuries and were labeled green. Total 67 (41.8%) underwent damage control surgery within two hours of arrival at accident and emergency. Most of the admissions were of Orthopedics and Chest surgery.
Conclusion: Effective and early disposal of patients from Accident and Emergency needs collaborative efforts of hospital administration following comprehensive disaster plan & preparedness. Trained triage team with quick surgical response needs trauma training, disaster management courses and drill exercises for doctors and health workers.
Keywords: Terrorist bombing, Preparedness, Triage, mass casualties, management.
Introduction
Pakistan is the most affected country by terrorism in the world after Iraq & Afghanistan, where severity of terrorist incidents is considerably more than these two countries[1]. In the year 2012 alone, Pakistan suffered from 1404 terrorist attacks, surpassing Iraq (1271) and Afghanistan (1023)[2]. On analyses from the year 2001 to 2013, there were 13,721 incidents in Pakistan. The number of suicide bombing between 2001 to 2007 were 15 only, but from 2007 to end 2013, suicide attack jumped to 358 the highest anywhere in the world.[3]
Karachi is the largest and the most populated city of Pakistan which spreads over 3530 Sq. kilometers with disorganized slums and the presence of 1.5 million illegal immigrants. This all makes the Karachi one of the most attractive place for terrorist activities.[3]
Bombs are attractive to terrorists as they are relatively easy to design, assemble, and deliver by changing modalities, and because they are sudden and violent in nature. Large explosions attract media coverage and produce large numbers of casualties, and increases the sentiments and anger of general public resulting in violence & disruption.[4]
Anticipation of disaster and the possibility of an influx of terrorist bomb blast victims are present at any time and day of the year. The number of patients with different grades and severity of injuries and multisystem involvement requiring management by different specialties.[5]This can disrupt the functioning of A&E in providing definitive medical care to all victims. Overcrowding overwhelms hospital resources, a term referred to as Main Gate Syndrome[6] Preparedness and planning for such events is the key to prompt and proper management.[7]Early disposal of all victims from A&E is also important as there is always threat of secondary blast at site and at hospital A&E. [8]
Pre-hospital decontamination of victims, triage and early stabilization or management capabilities are sparse and not coordinated in Karachi and Sindh. Victims are rushed as “Scoop & Run” in private vehicles, public transport and ambulances without trained staff, which further disrupts disaster management. [9]
Security at the hospital’s Accident and Emergency entrance is very important for smooth functioning during disaster management. Media handling is important by providing information and facilitations at one place. For all these tasks prior training & drill of Accident & Emergency staff and the surgical team is very important which enhances collaboration and coordination during the disaster.[10, 11, 12] This study is performed to access the preparedness and effectiveness of the A&E department after series of training workshops and disaster drills carried out for the security personals, media managers, paramedics, medical staff and doctors.
Methods
This is the study of four major events of bomb blast which occurred in last sixteen months in Karachi. All victims of these four bomb blast were transferred immediately from scene of blast to A&E by “scoop & run” in different vehicles mainly ambulances without any treatment on the way to hospital.
Incident 1: All 50 victims of an incident of terrorist bomb blast in a bus at Karachi Cantonment Station on 29th December 2012, at 1530 hours, reached JPMC within 10 minutes by ambulances and private vehicles. The bomb was placed at the roof of stationary bus with few passengers. Victims were mostly hawkers and shopkeepers. Blast site was within 1 km of hospital, blast was heard & felt in A&E and preparation started. All patients were triaged at A&E department entrance, categorized in four groups and directed to pre-designated areas for further management. (Table I)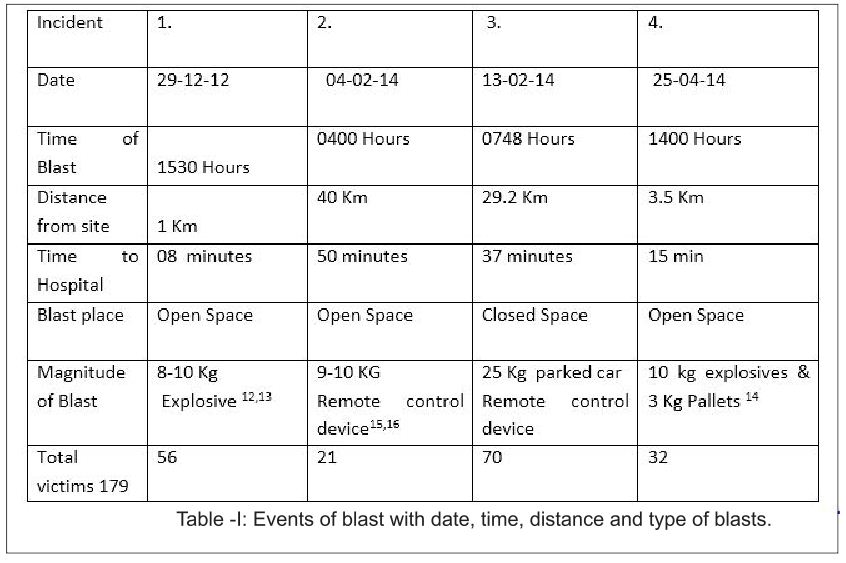
Incident 2: A bomb blast at Ghaghar railway track on 4th February 2014 at 0400 hours resulted in 20 casualties. Distance from site to JPMC is 40 km (24.85 Miles). Casualties started coming to A&E after 50 minutes. (Table I) All the staff from security personal to surgeons & anesthetist were prepared. In next ten minutes all patients were triaged, primary survey was performed and patients were immediately shifted to designated areas.
Incident 3: Seventy Special Security Unit (SSU) personnel of police going for duty in a bus were struck with an Improvised Explosive Device (IED) implanted in a roadside vehicle on 13th February 2014 at 0748 hours near Police Training Centre. The distance from police training centre to JPMC is 29.2 km (18.02 Miles) and travel time is approximately 37 minutes. The first wave of casualties began to arrive in A&E in ambulances (Table 1). All specialties staff & consultants were available in A&E when first patient reached hospital.
Incident 4: Delhi Colony Bazaar blast took place on 25th April 2014 at 1400 hours. The distance of the blast site from JPMC is 3.5 Km (2.17 Miles). The first casualties started reaching after 10 minutes. 29 injured and 3 dead victims were received at the A&E. (Table I).
Hospital administration and A&E department got immediate blast incidents information through media. Emergency plan for bomb blast were activated immediately, information conveyed to surgical specialties and departments through hospital operator. Security came into action; they controlled the designated spots as per plan. Space was created in A&E by sending the existing patients to respective wards. As soon as triage was performed, patients were assessed with primary survey, all adjuncts were performed in resuscitation bay and secondary survey of every patient done as soon as patient got stable after primary survey. Urgent procedures performed immediately in A&E in few red tagged patients & others shifted to operation theatres. Yellow tagged patients requiring surgery were also shifted to operation theatre recovery room; other patients were admitted in wards for care. All dead bodies were kept at one place for medico legal proceedings away from working area. It was noted that most of the trained A&E staff was speaking the same language and managing patient according to trauma course protocol.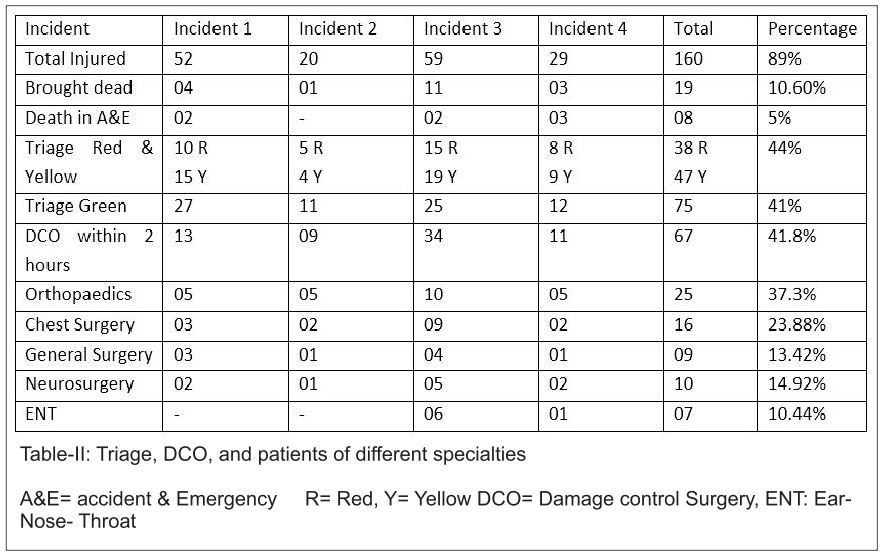
Results
All one hundred sixty patients presented with wounds of splinters, shrapnel or burns along with specific injuries to different body parts. Nearly all patients required wound debridement and wound dressings. Sixty seven patients underwent damage control surgery within next two hours. Orthopedic surgery was the busiest specialty, and common procedures performed were wound debridement, amputations, putting Steinman pin and application of external fixator in 37.33% of patients. (Table II) Next common involvement was of chest and sixteen patients required chest tube insertion for open & closed chest injuries. Nine patients required laparotomy. Eight patients died in A&E department within 2 hours of their arrival. They were having multi system involvement and having more than 70% burns in three patients. 75(41%) patients in green category were detained and managed with dressings of minor and medium size wounds. Secondary survey of all the patients was performed. It had been observed that around 15% of the victims of bomb blast died at site or within two hours, 44% of patients were in red & yellow category and 41% in green. All the patients who were labeled green were also kept under observation for at least six hours. Administration displayed & circulated computerized lists of all the victims of the blast and their place of admission. It was noted that after arrival of last patient of the incident, emergency was free of all the patients of bomb blast incident in thirty minutes time.
Discussion
Terrorist are using different and newer methods, places and timings for bomb blast activities. It is sudden and tends to disrupt the functioning of Accident & emergency department. To combat and to give best medical relief to the bomb blast victims; planning, preparation & drills are key elements.[11,12] Communications and coordination with security, media and local administration is important for smooth functioning. Hospital administration is an integral part of the in-hospital response to a major incident and is involved in training exercises with a clear chain of command and communication. An operational room, along with telephone switch room is set up for coordinating the in-hospital response and liaison with other hospital and other emergency services as per disaster plan. [13] Hospital security is immediately enhanced after a terrorist bomb blast, as hospitals themselves may become targets for terrorism8. This also makes sure that all the Emergency Department staff is working with full concentration without any fear or pressure of mob or violence directed towards them. Significant overcrowding is also noted in Accident & emergencies which can be controlled at gate, early shifting of patients to concerned units, creation of a holding unit in OPD or recovery rooms and active inter-facility transfer. [14]
Patients triage on site and transfer under supervision of trained ambulance staff is sparse in our country and most patients reach hospital in ambulance or in private vehicles as “Scoop & Run”.[15] This has been seen in most of the urban disasters, as in Bali 2002 and New York 2001 blasts, where patient with significant injuries and burn leave the scene quickly and reach hospital on their own.[13] It is very important that experienced and trained senior medical officer perform the triage of blats victims at A&E entrance and from there flow of triaged cases should be uni directional.[16] Frequent reassessment of the victims by senior surgeon enhances the detection of missed injuries and diagnosis of pulmonary blast injuries.[13] In this series of events triage was performed and supervised by Primary trauma Care (PTC) and Hospital Preparedness for Emergencies (HOPE) course graduates and Instructors. A study conducted in Karachi, in July 2008, at two major hospitals, including the Jinnah Postgraduate Medical Center, to evaluate the preparedness and self-identified deficiencies of doctors involved in massive trauma and casualty management, 7 revealed that only 3.3% of doctors working in accident & emergency department were confident about their management of bomb blast victims. No simulated drills or courses had been conducted for disaster management in the emergency department of the surveyed hospitals5. After this survey 12 two day courses & workshops of PTC and HOPE were conducted for doctors and nurses working in Jinnah Post Graduate Medical Center Karachi.[17,18] One hundred doctors and twenty nursing staff were trained for triage and golden hour management. This was stated in a similar study that Trauma course like ATLS also improves the outcome of victim’s management in mass casualty events.[19, 20]It is also observed that simplified triage scheme and table top exercises for Emergency staff, enhances their performance in multiple casualty incidents. [21]
During the four reported bomb blast incidents, a media staging area was designated, where regular updates were provided by the concerned officials. This media relation with hospital administration also improves patient’s management. It was observed that man power resources like OT staff, nurses, surgeons and anesthetist were always adequate as most live within hospital compound and everybody respond within 10-15 minutes.
Primary survey, stabilization of patients and documentation started at the same time. 15% of patients of blast injuries were brought dead or died within two hours of their arrival during management; this corresponds to figure in most of the series.[9, 16]Those who required immediate surgery were shifted to operation theatres. All the other patients were dealt accordingly in Accident and Emergency Department, and within 30 minutes of arrival of last patient of the blast incident, these patients were shifted to respective departments according to the nature of their injuries. Immediate & early deaths in A&E, operation room and ICU were around 5%, which corresponds to other studies in similar circumstances.[15, 22]All data was recorded and analyzed. Complete list of the victims, their status and place of admission were displayed at a prominent place in hospital and briefed to media as well. Quick disposal of patients is very important from the Accident and Emergency Department as this can be a soft target for a secondary blast.[4, 22] Also, city wide riots can start in response to a bomb blast and new influx of patients start coming to the department[8]. It is also noted that clinical manifestation of pulmonary barotraumas may take time to appear. In this series of incidents also 16 patients underwent Chest tube insertion due to detection of blast lungs. Minimally Injured patients (Green) also require a minimum of 6 hours observation before being discharged[13]. All the measures taken in A&E department were for best management of patients of terrorist bomb blast; smooth functioning of hospital and utilization of resources effectively.
Conclusion
Early and effective management at A&E needs collaboration of different agencies, pre event planning and preparation. A collaborative effort in a mass casualty incident can be achieved by repeated training courses and drill exercises for trauma, triage & disaster which results in reduced morbidity and mortality of the victims. Emergency medical technicians should be trained in on-site triage and following an Incident Command System. A centralized hospital communication can limit the burden of trauma on one particular A&E and the patients may be taken to other tertiary and trauma centers. The coordinated team achieves quick disposal of patients from A&E in 25-30 minutes and can save lives in the event of a second disaster.
References
1. Prommersberger KJ, Fernandez DL. Nonunion of distal radius fractures. Clin Orthop Relat Res. 2004 Feb;(419):51-6.
2. McKee MD, Waddell JP, Yoo D, Richards RR. Nonunion of distal radial fractures associated with distal ulnar shaft fractures: a report of four cases. J Orthop Trauma. 1997 Jan;11(1):49-53.
3. Segalman KA, Clark GL. Un-united fractures of the distal radius:Areport of 12 cases. J Hand Surg. 1998;23A:914–919
4. Gómez EA, Mena RV. [Treatment of distal radius non-union in a three-stage procedure. Case report]. Acta Ortop Mex. 2009 Jan-Feb;23(1):26-30
5. Prommersberger KJ, Fernandez DL, Ring D, Jupiter JB, Lanz UB. Open reduction and internal fixation of un-united fractures of the distal radius: does the size of the distal fragment affect the result? Chir Main. 2002 Mar;21(2):113-23
6. Watson-Jones R. Fractures and other bone and joint injuries. 2nd edition. Edinburgh: Livingstone; 1942.
7. Karuppiah SV, Johnstone AJ. Sauvé-Kapandji as a salvage procedure to treat a nonunion of the distal radius. J Trauma. 2010 May;68(5):E123-5
8. Hamada G. Extra-articular graft for non-union in Colles’s fracture. J Bone Joint Surg 1944;26:833-835.
9. Bacorn RW, Kurtzke JF. Colles’ fracture: a study of two thousand cases from the New York State Workmen’s Compensation Board. J Bone Joint Surg 1953;35A:643-658.
10. Harper WM, Jones JM. Non-union of Colles’ fracture: report of two cases. J Hand Surg 1990;15B:121–3.
11. Saleh M, Ribbans WJ, Meffert RH. Bundle nailing in nonunion of the distal radius: case report. Handchir Mikrochir Plast Chir 1992;24:273-275.
12. Smith VA, Wright TW. Nonunion of the distal radius. J Hand Surg Br. 1999 Oct;24(5):601-3
13. Fernandez DL, Ring D, Jupiter JB. Surgical management of delayed union and nonunion of distal radius fractures. J Hand Surg 2001;26A:201–9.
14. Grecco Marco Aurélio Sertório, Angelini Luis Carlos, Oliveira Marcelo Tavares de, Trombini Nelson, Martins Francisco Carlos, Barbosa Sônia Maria de Almeida Pacheco. Treatment of nounion in the third distal of the radio. Acta ortop. bras. 2005;13(2): 95-99.
15. Ring D. Nonunion of the distal radius. Hand Clin. 2005 Aug;21(3):443-7
16. Crow SA, Chen L, Lee JH, Rosenwasser MP. Vascularized bone grafting from the base of the second metacarpal for persistent distal radius nonunion: a case report. J Orthop Trauma. 2005 Aug;19(7):483-6
17. De Baere T, Lecouvet F, Barbier O. Breakage of a volar locking plate after delayed union of a distal radius fracture. Acta Orthop Belg. 2007 Dec;73(6):785-90.
18. Villamor A, Rios-Luna A, Villanueva-Martínez M, Fahandezh-Saddi H. Nonunion of distal radius fracture and distal radioulnar joint injury: a modified Sauvé-Kapandji procedure with a cubitus proradius transposition as autograft. Arch Orthop Trauma Surg. 2008 Dec;128(12):1407-11.
19. Cao J, Ozer K. Failure of volar locking plate fixation of an extraarticular distal radius fracture: A case report. Patient Saf Surg. 2010 Nov 25;4(1):19.
20. Koo Siu-Cheong Jeffrey Justin, Ho Sheung-Tung, Non-union of Fracture of Distal Radius: A Case Report and Literature Review, Journal of Orthopaedics, Trauma and Rehabilitation, June 2011; 1(1):21-24
21. Nusem I, Moghaddam AK. Darrach’s ulnar resection and ulna intercalary bone graft for non-union of the distal radius: two birds one shot. Eur J Ortho Surg Traumatol 2011;21:345-349
22. Rappo TB, Kanawati AJ. Non-Union Of Fractured Distal Radius Treated With A Volar Locking Plate: A Case Report. The Internet Journal of Orthopedic Surgery. 2012 Volume 19 Number 2.
| How to Cite this article: Minhas M S, Mahmood K, Effendi J, Kumar R, Bhatti A . Terrorist Bomb Blasts: Emergency department management of multiple incidents. Trauma International July-Sep 2015;1(1): 36-40 |


{kind=link}