
Hip Instability following DHS Fixation Surgery for Unstable Four Part Per-Trochanteric Fracture Femur
Volume 2 | Issue 1 | Jan-Apr 2016 | Page 37-41|Yashwant J. Mahale, Vikram V. Kadu, Abhijeet Deshmukh
Author: Yashwant J. Mahale[1], Vikram V. Kadu [1], Abhijeet Deshmukh[1]
[1] ACPM Medical College , Dhule – 424001 , Maharashtra India.
[2] Mahale Accident Hospital , Dhule, Maharashtra India.
Address of Correspondence
Dr. Vikram V Kadu
C/O Vilas Shamrao Kadu, Plot no. 20, Kadu House, Barde layout, Katol Road, Nagpur – 440013
Email: vikram1065@gmail.com
Abstract
Background: In an ageing population, with resultant osteoporosis hip fractures are common indication for per-trochanteric fracture hip repairs. Various modalities of surgical treatment basically emphasis fracture reduction, fracture immobilization, and rehabilitation as a guide to treatment. Subluxation or dislocation following operative treatment of four part unstable per-trochanteric fracture with Sliding Hip Screw is rare and occasional cases have been reported.
Material and Methods: An observational prospective study carried out at tertiary care hospital from Jan 1997 – Dec 2014. Our operative experience of total 510 patients of which 480 underwent DHS fixation surgery for unstable four part per-trochanteric fracture showed 6 cases of instability as subluxation and dislocation.
Results: We report 6 cases out of 480 DHS fixation showing instability in 3 cases and subluxation and dislocation in 3 cases after 6 weeks of follow-up. These patients were offered arthroplasty and the follow-up results were evaluated after 8 months. Among 6 cases, four had instability after six weeks and remaining two developed dislocation after eight months which were associated with infection. 1 patient refused further investigations & treatment, 3 other died with due course of time, 1 lost to follow -up and One patient with infection underwent excision arthroplasty.
Conclusion: Hip instability following DHS fixation surgery for four part Per-trochanteric fracture femur is a rare complication. Cause of this complication could be mechanical factors (excessive collapse, rotational torque) and infection (superficial or deep) may serve as a contributing factor. Diagnosis was done mainly on the basis of clinical examination and investigations such as X-rays, USG and blood tests. Treatment for such complications consists of Hip arthroplasty. These complications can be prevented with the use of TFN or cemented bipolar prosthesis primarily for treating these type of fractures.
Keywords: Intertrochanteric fracture, hip instability, surgical fixation
Introduction
Per-trochanteric (4 Part) fractures of femur are commonest in elderly people. The incidence is expected to increase in the coming years, with an ageing population resulting in a greater number of traumatic injuries in patients with osteoporotic bone.
DHS fixation is gold standard modality for treatment of such fractures. Various implants used for such fractures are 1) DHS Sliding compression screw and plate devices 2) Intra-medullary devices such as TFN and PFN 3) Enders Nail, 4) Bi-axial plate, 5) External fixator 6) Jewett nail and SP nail. Various Complications of DHS implant are as follows: 1) Implant Failure: a) Cut out of screw b) Proximal or distal migration of screw c) Breaking of plate and screws, 2) Uncontrolled Medialisation of distal fragment and collapse at fracture site, 3) AVN with collapse of head , 4) Infection: Superficial or Deep infection [1)]. However, Hip Instability: Subluxation and Dislocation is very rare [2]. We report, six cases of Hip instability following 480 cases of DHS fixation surgeries for unstable four part Inter- trochanteric fracture.
Materials and Methods
This is a prospective study conducted at our hospital since 1997. We reviewed patients with inter-trochanteric fracture femur treated with various implants. We performed 510 surgeries for Pertrochanteric fracture femur with different modalities DHS (n=480), TFN (n=13), Biaxial Plate (n=15), SP nail (n=1), and Enders Nail (n=1). We found six cases who developed hip instability only after DHS fixation. All available clinical notes and X-rays of these patients were studied to get the relevant information. Of the six cases three were male and two female patients, four had right sided fracture and one had left sided fracture, 4 had infection and 2 had mechanical problems, 1 patient refused further investigations & treatment, 3 other died in due course of time due to unrelated disease complications. 1 lost to follow –up and 1 patient with deep infection underwent excision arthroplasty. Radiological findings of these patients are shown in table 1 and 2.

Table 1: Table showing radiological findings at the diagnosis of instability.
")
Table 2: Table showing radiology of collapse
*Pre-op measurement was done by drawing a straight line from Greater to lesser trochanter n then from the mid point upto the head of femur.
* Collapse of the fragment was calculated from lateral blade plate upto the screw that has back-out.
* The average collapse in the above mentioned cases was 9 mm which was found to be excessive as compared to the distance of lag screw backout with a mean length 8.8 mm.(11)
Case 1:
A 60 yrs old male was admitted to our hospital with history of domestic fall on Right hip. X-Ray Pelvis with both Hips AP View showed four part pertrochanteric fracture of femur (Fig. 1). Patient had previous history of myocardial infarction. He was treated with DHS and 135 degree 5 hole plate. Early post-operative period was uneventful. Immediate Post-operative X-Ray (Fig. 2) showed relatively acceptable valgus fixation , greater trochanter fragment was not fixed . At 6 weeks follow-up, patient complaint of gradual onset deep pain and difficulty in mobilising right hip. There was no history of recent fall, trauma, fever. On examination, limb was shortened, adducted and internally rotated. Patient had no evidence of infection, movements were limited and painful in all direction . X-Ray Pelvis with both Hips AP View (Fig. 3) showed subluxation of hip joint with DHS implant in situ, excessive collapse at fracture site, rotated femoral head, medialisation of shaft with displaced greater trochanter. The dislocation was reduced and abduction brace was given. Routine Blood examination reports WBC counts – 8300 , ESR – 12 , CRP – Non-Reactive. Patient was medically & financially restrained for further management. Hence immobilisation was continued with brace (Fig. 4). Patient died at the end of 3 months at home.

Figure 1: pre-operative X-ray showing IT fracture femur right side

Figure 2: immediate post-operative X-ray showing good, stable fixation

Figure 3: At 6 weeks follow-up, X-ray showed subluxation of hip joint

Figure 4: fracture reduced and Abduction brace was provided to maintain the reduction
Case 2:
70 yr old diabetic male referred to our hospital with gradual onset deep pain, difficulty in mobilization since 15 days. He had history of domestic fall on Right hip 8 weeks back. X-Ray right Hip AP View showed four part pertrochanteric fracture of femur. He was treated with DHS and 135 degree 5 hole plate. Immediate Post-operative X-Ray showed stable fixation with DHS implant in situ. Now the patient complained of pain and limp while walking. On examination, limb was shortened, adducted and internally rotated. Patient had infection at operative site and bed sore. Movements were limited and painful in all direction. X-Ray Pelvis with both Hips Ap View showed dislocation of hip joint with DHS implant in situ, excessive collapse at fracture site, rotated femoral head, medialisation of shaft with displaced greater trochanter. Routine Blood examination reports WBC counts – 17,000 , ESR – 88 , CRP – 1:32 (Reactive). Patient was admitted for further investigations and management but Patient developed Septicaemia and diabetic keto-acidosis and died.
Case 3:
70 year old female, known case of hypertension, presented to our hospital with gradual onset deep pain, difficulty in mobilization, discharging sinus from operative site in left hip since last two months. She suffered a domestic fall on Left hip 6 months back. X-Ray left Hip Ap View showed Unstable four part pertrochanteric fracture of femur. She was treated with DHS and 135 degree 5 hole plate. Immediate post -operative X-Ray was satisfactory. Early post-operative period was uneventful. She was mobilised with walker and then full weight bearing at 4 months. After 6 months, She had discharging sinus and limitation of range of movement of left hip for which she was referred to our hospital. On examination, limb was shortened, adducted and internally rotated, local temperature was raised, operative site was discharging pus with granulation tissue. X-Ray left Hip Ap showed dislocation of hip joint with widely displaced greater trochanter and excessive collapse at fracture site with medialisation of distal fragment. Routine Blood examination reports WBC counts – 13,500, ESR – 70, CRP – 1:32 Reactive. Patient was not willing for further treatment and lost to follow up.
Case 4:
70 years old female known hypertensive presented to our hospital with history of domestic fall on Right hip. X-Ray Pelvis with both Hips AP View showed Unstable four part pertrochanteric fracture of femur. She was treated with DHS and 135 degree 5 hole plate. Intra-operatively, femoral head was found to be rotating during reaming and screw insertion. Early post-operative period was uneventful. At 6 weeks follow up Patient presented with gradual onset deep pain and difficulty in mobilising right hip. There was no history of recent fall, trauma, fever, discharging sinus. On examination, patient had no superficial or deep tenderness, movements limited and painful in all direction. X-Ray Rt. hip AP showed dislocated hip with DHS implant in situ, excessive collapse at fracture site, rotated femoral head and medialisation of shaft. Routine Blood examination reports WBC counts – 8300, ESR- 22, CRP – Non-Reactive. Patient was admitted for further management but died due to Cerebrovascular accident.
Case 5:
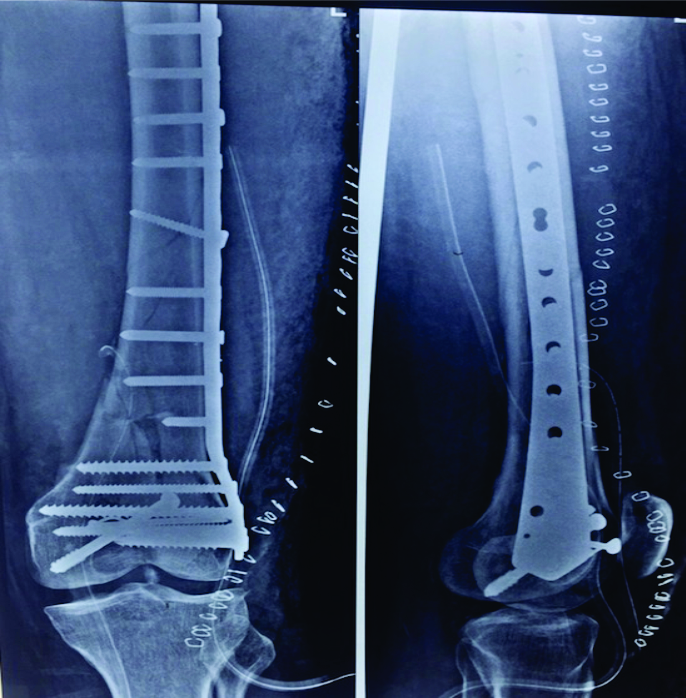
65 years old male, came to our hospital with history of fall over right hip. X-Ray Pelvis with both Hips AP View showed Unstable four part inter-trochanteric fracture of femur (Fig. 5). He was treated with 135 degree DHS with 5 hole plate. Immediate post – operative X-Ray was satisfactory (Fig. 6). The patient came regularly for follow-up. Weight bearing was started at 6 weeks. At 10 months follow-up, the patient presented with discharging sinus. On examination, limb was shortened, adducted and internally rotated. Patient had superficial and deep tenderness, movements were restricted and painful in all direction. X-Ray Pelvis with both Hips AP View at 10 months showed subluxation of femoral head with DHS implant in situ, excessive collapse at fracture site, rotated femoral head, with subluxation of the femoral head (Fig. 7). Routine Blood examination reports WBC counts – 9,800, ESR – 80, CRP – Reactive (1:32).USG was done which reported collection in proximal thigh with extension into the hip joint S/O Joint effusion. Hip aspirate was done and pus aspirated was sent for culture. Patient underwent implant removal and excision arthroplasty. Intra operatively large amount of pus was found (Fig. 8), which was drained and infected soft tissue debridement was done to remove all infected and nonviable tissue. Pus and infected deep soft tissues were sent for immediate Gram’s stain, culture and antibiotic sensitivity tests and the head was sent for histopathology which confirmed the diagnosis of pyogenic infection. A skeletal traction system through proximal tibia was applied. Two staged Total Hip Replacement was planned but the patient refused due to financial restraints and ended up with excision arthroplasty (Fig. 9).

Figure 5: pre-operative X-ray showing IT
fracture femur right side

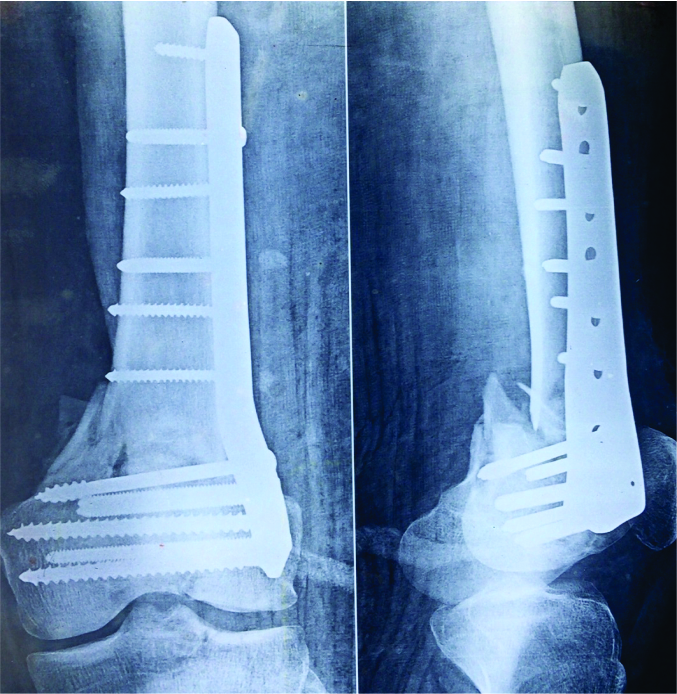
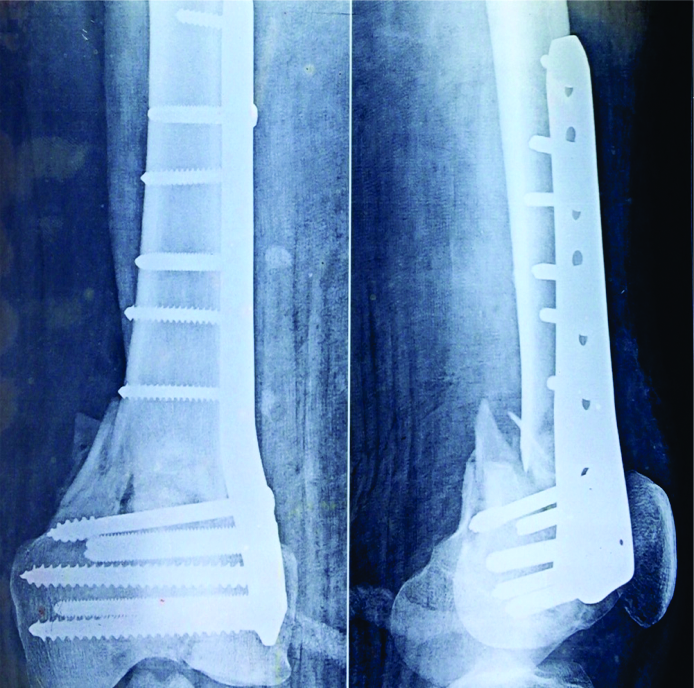
Figure 6: immediate post-operative X-ray showing good, stable fixation

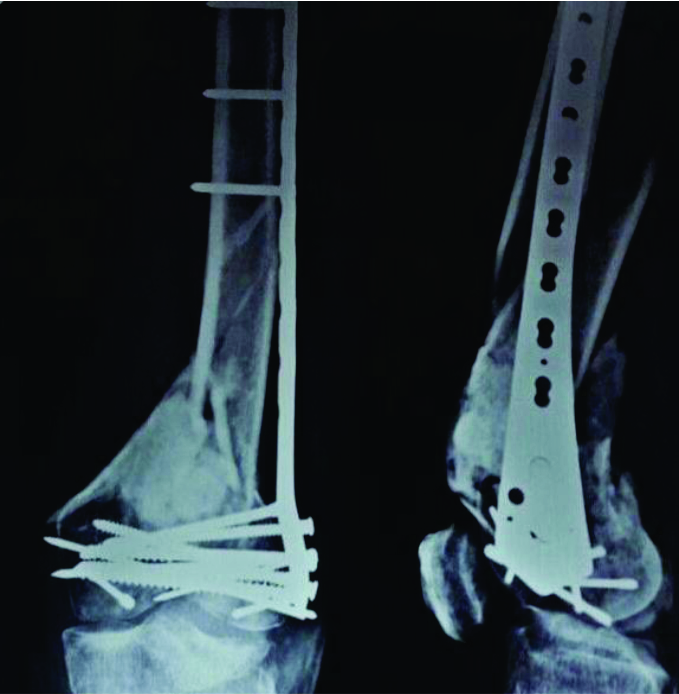
Figure 7: At 10 months follow-up, X-ray showed subluxation of hip joint

Figure 8: intra-operatively pus was present at the operative site and the head was completely deformed

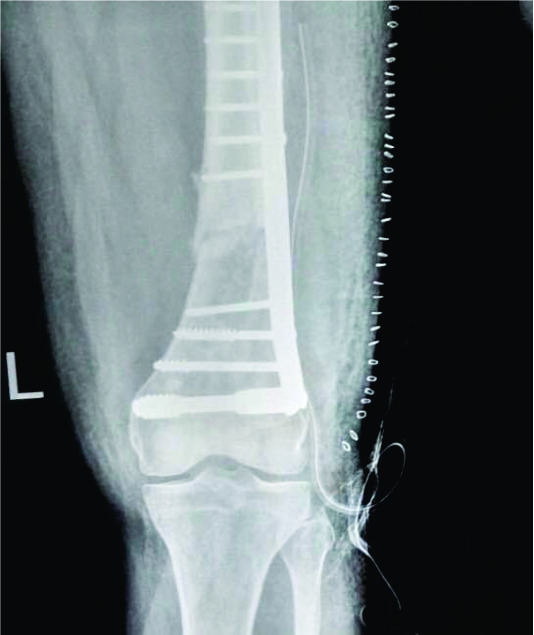
Figure 9: At 6 weeks follow-up after excision arthroplasty
Case 6:
55 years old male k/c/o diabetes and hypertension, came to our hospital with history of fall over right hip. X-Ray Pelvis with both Hips AP View showed Unstable four part inter-trochanteric fracture of left femur (Fig. 10). He was treated with 135 degree DHS with 5 hole plate. Immediate post – operative X-Ray was satisfactory (Fig. 11). The patient came regularly for follow-up. At 6 weeks follow-up, the patient presented with discharging sinus. On examination, limb was shortened, adducted and internally rotated. Patient had superficial and deep tenderness, movements were restricted and painful in all direction. X-Ray Pelvis with both Hips AP View at 6 weeks showed subluxation of femoral head left with DHS implant in situ, excessive collapse at fracture site, rotated femoral head, with subluxation of the femoral head (Fig. 12). Routine Blood examination reports WBC counts – 11,800, ESR – 67, CRP – Reactive (1:32). USG was done which reported collection in proximal thigh with extension into the hip joint S/O Joint effusion. Hip aspirate was done and pus aspirated was sent for culture. The hip was reduced. Patient was not willing for further treatment so was treated by giving abduction brace. The patient died with due course of time due to comorbid conditions.
Discussion
Hip subluxation / dislocation is very rare complication after DHS surgery for four part inter-trochanteric fracture. The present series revealed incidence of 1.04% of 480 DHS suegeries performed. On review of literature occasional case reports of hip instability have been reported [1,2,3,4,5]. Our patients did not undergo further management after making diagnosis of instability for various reasons (3 died, 1 lost to follow up, 1 refused for further management, 1 underwent Excision arthroplasty); (see table no. 3). Various etiopathologies of dislocation / subluxation are on the basis of clinical examination, X-ray, Investigations and review of literature. In these cases it appeared that the factors responsible for instability could be mechanical factors but in some cases presence of pyogenic infection states that infection can be a major contributing factor.

Table 3: Patients demographics indicating age, sex, type of fracture, associated injuries, causative factors and fixation used.
Four part per-trochanteric fracture is generally caused by direct fall on the greater trochanter. This direct force as well as the muscular avulsion force leads to the damage of the capsule, surrounding soft tissues and ligaments and also greater and lesser trochanter are separated making the head rotate freely without any attachment left to it. It is well accepted practice of extraction of femoral head during hemi-arthroplasty procedures. While doing DHS we found out that the femoral head undergoes rotational torque atleast three times (during reaming, tapping and screw insertion ) specially when derotation wire is not used. In all the above mentioned cases the derotation wire was not used. This may cause damage to the remaining soft tissue attachments leading to instability. In right-sided fractures, the screw insertion causes the head fragment to rotate clockwise causing the head fragment to rotate into an extended position at the hip joint. Whereas, in left-sided fractures, the screw insertion causes the head to rotate clockwise leading to head and neck fragment into flexion at the hip and extension of the fracture site leading to potentially unstable construct [8], thereby increasing the soft tissue damage.
Lateral wall plays a key role in stabilisation of unstable pertrochanteric fractures by providing buttress for proximal fragment and its deficiency leads to excessive collapse [6], (table no.2) almost complete resorption of neck causing head to be stabilised against most lateral support which may force femoral head out of acetabulum . Therefore, maintaining the integrity should be important objective in all stabilisation procedures. In patients with four part pertrochanteric fracture femur, if there is gross comminution of posterior & medial cortex , in such patients, femoral head may go into retroversion and varus after fixation due to excessive collapse which may lead to posterior & lateral subluxation of head with progressive weight bearing or stress , finally resulting into dislocation of such hip. Thus lateral wall deficiency, excessive collapse, valgus fixation and postero-medial comminution plays a vital role in determining the instability of the femoral head. All the above mentioned factors are seen in our case series. (table no. 1 and 2).
Patient factors such as mental retardation, poor patient compliance, alcoholic patients, infection and neurogenic causes may lead to dislocation [7]
In our study, 3 cases had infection of which 2 had early and 1 late infection. In early stages of acute infection [4] instability of femoral head may be accounted because of destruction of soft tissue, such as capsule, ligaments and spasm of the adductors. In late stages i.e. chronic infection, the head is damaged asymmetrically in addition to above mentioned factors leading to instability [3] as seen in case 5.
This complication has not been reported with SP nail plate, Jewett nail, TFN, Biaxial plate etc. This may be because rotational torque is not required in fixation of fractures with these implants. However, in case of enders nailing 1 case report has been found leading to dislocation which they claimed was because of perforation of the capsule due to migration of nails in the posterior joint capsule(2). And the other case in which internal fixation of femoral neck fracture was done, concluded that possibly some rotation of the proximal fragment was inadvertently caused, when the fracture was reduced, resulting in twisting of capsule previously torn by trauma [1] suggesting that capsular damage also plays a vital role in instability of hip.
Once dislocation develops; clinical examination of patients, and investigations such as X-rays, CBC, ESR, CRP should be carried out to find out the causes. MRI / CT [10] is not advisable due to implant in situ and may not give the desired result. USG may help to show collection followed by aspiration leading to the diagnosis of infection. Hip arthroplasty would be appropriate option for such complications (Partial, Total, Excisional) depending upon the willingness, associated medical co-morbidities and financial status of the patients.
All the 6 cases who suffered complication were treated with DHS. Mechanical problem during fixation of DHS, loss of lateral femoral wall integrity are definite indicator of DHS implant failure with infection playing a major contributing role. With such fractures, role of DHS must be guarded, augmented with trochanteric stabilisation plate or intra medullary fixation such as TFN or cemented bipolar prosthesis should be considered. While reaming, tapping and screw insertion, additional derotation guide wire must always be used. Greater trochanter should be fixed and head should not rotate intra-operatively after fixation.
References
1. Melton JT, Yates P, Middleton RG. Dislocation of hip following valgus fixation of unstable peri-trochanteric fractures : A complication. Injury Extra 2006,
2. Iwegbu CG. Dislocation of the hip following Ender nailing. A case report. J Bone Joint Surg [Am] 1981;63:839-41.
3. Munjal S, Krikler SJ. Dislocation of the hip following intertrochanteric fracture. Injury 1995;26(9):645-6.
4. Infective Failure of Internal Fixation for Intertrochanteric Femoral Neck Fracture Presenting as Hip Joint Subluxation: A Case Report Rohit Rambania, c, Helen Ribeeb, Peter Bobakb; J Med Cases 2010;1(2):51-54.
5. Derek Younge, MD, FRCSC; Patrick A. Loisel, MD, FRCSC. A rare case of hip dislocation after internal fixation of femoral neck fracture without infection; JCC, Vol. 40, No1, février 1997.
6. Gotfried Y. The lateral trochanteric wall: a key element in the reconstruction ofunstable pertrochanteric hip fractures. Clin Orthop Relat Res 2004;425:82–86,
7. Mahoney CR, Pellicci PM. Complications in total hip arthroplasty: avoidance and management of dislocations. Instr Course Lect 2003;52;247-55.
8. Mohan R, Karthikeyan R, Sonanis SV.Dynamic hip screw: does side make a difference? Effects of clockwise torque on right and left DHS. Injury. 2000 Nov;31(9):697-9.
9. Speed JS, Knight RA. Postoperative infections following internal fixation for fractures of the hip. Ann Surg 1956;143(5):651-657; discussion, 657-659.
10. Moorman CT 3rd, Warren RF, Hershman EB, et al. Traumatic posterior hip subluxation in American football. J Bone Joint Surg Am 2003;85A(7):1190-1196.
11. T6-10 APOA 2009 Trauma & Infection,Taipei : The Average Distance of Lag Screw Backout in Unstable Intertrochanteric Fracture After DHS Fixation with Trochanteric Stabilizing.
| How to Cite this article: Yashwant J. MahaleYJ, KaduVV, Deshmukh A. Hip Instability Following Dhs Fixation Surgery for Unstable Four Part Per- Trochanteric Fracture Femur. Trauma International Jan-Apr 2016;2(1):37-41. |
 Dr Yashwant Mahale |
 Dr. Vikram V. Kadu |
 Dr. Abhijeet deshmukh |











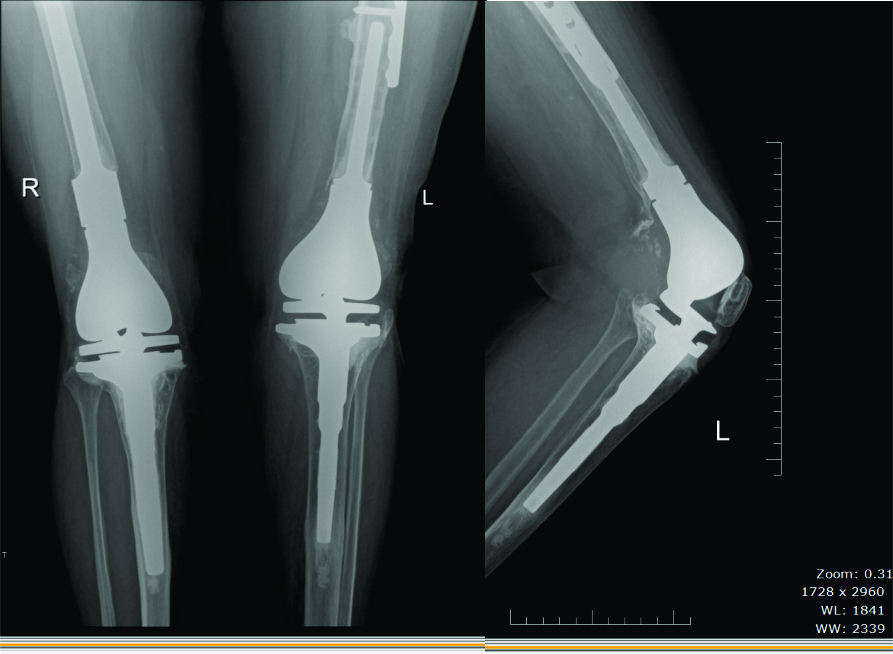





 and shaft (32B2.2) fractures with a DHS-retrograde nail combination Fig 4A Pre-operative x-rays Fig 4B Immediate post-operative x-rays")


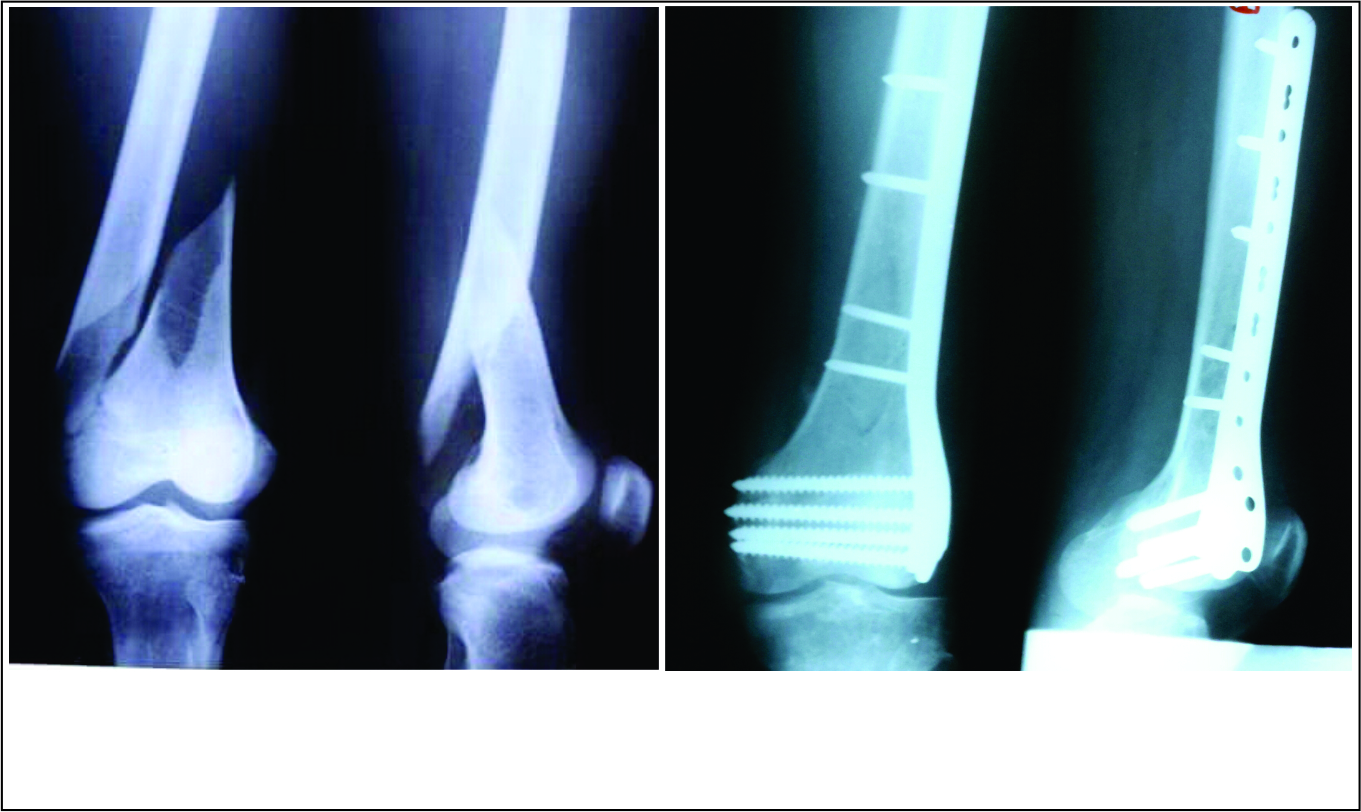
 occurring below a hip prosthesis, with pre-existing gonarthrosis Fig 7A,B Pre-operative x-rays, showing a spiral fracture line with a wedge fragment anterodistally Fig 7C,D Immediate post-operative x-rays after open, compression plating with DF-LCP, overlapping the plate over the hip stem")







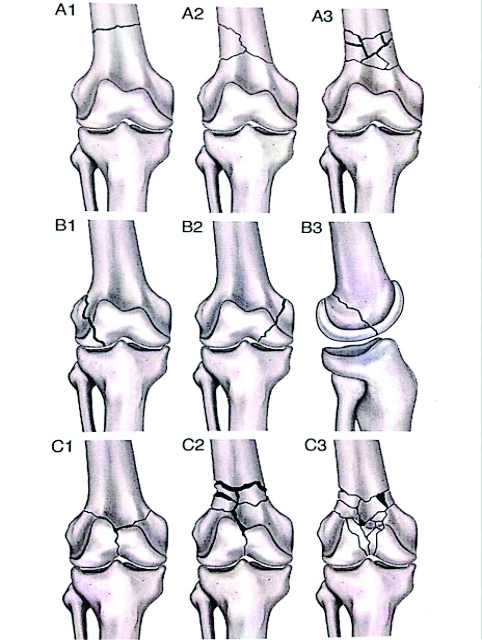
![Table 3: The recommended Surgical treatment option based upon the type of the Muller's classification is[ 12,13 ]](http://traumainternational.co.in/wp-content/uploads/2016/05/tab3.jpg "Table 3: The recommended Surgical treatment option based upon the type of the Muller's classification is[ 12,13 ]")




