
New totle
Vol 3 | Issue 1 | May – June 2017 | page:41-42 | Neeraj Bijlani, Ashok Shyam
Author: Neeraj Bijlani [1], Ashok Shyam [2]
[1] OrthoTech Clinic and Sai Baba Hospital, Mumbai, India
[2] Indian Orthopaedic Research Group, Thane & Sancheti Institute of Orthopaedics and Rehabilitation, Pune, India.
Address of Correspondence
Dr.Neeraj Bijlani
OrthoTech Clinic, 405, Shubham Atlanta, RC Marg, Chembur East, Mumbai 400071.
Email: drbijlani@gmail.com
Abstract
Mobile apps have been an integral part of our lives since the App Store was launched in 2009. Now after the Mobile Apps Revolution, Medical Apps have also been an integral part of our Lives. To begin with this series we present to you an app which makes Review of Literature, Reading Articles and Abstracts on the go and Following topics, Journals and Specialities very easy at the tap of a finger.
Introduction:
The iPhone App Store was launched in July 2008 and was followed by the Google Play store in 2012. The above ones are the most popular mobile operating sys-tem in the world till date. The mobile apps have changed our lives and the way we com-municate with each other and go about doing things. So is the world of Medical and Orthopaedic Apps which have been on the forefront since last few years.
Here we present you a series of review of few Medical Apps which we regularly use and make a difference in our lives and the way we practice Orthopaedics and increase productivity.
Review:
Read by QxMD is a free app available to download from the iPhone App Store and Google Play Store and can also be used as a Web App from the Windows Platform and Computer.
It is like Twitter for Medical Literature. As soon you install the app on your mobile device, you get a screen (Fig. 1) to Sign Up or Login (if you already have an account). After you tap Sign up You are taken to a Personalisation Page (Fig. 2) which is self-explanatory. After you have completed the sign up process fill up very few fields. So in profession I filled up Physician and Speciality – Orthopaedics and Location – India that is where we are from (Fig. 3).
After that there are some other specialities which you can follow so I follow Sports Medicine. Then the next screen takes you to Keywords (which can be words like Rotator Cuff Tears, Distal Radius Fracture, and VTE prophylaxis. Then there are collections which you can follow which could be accumulated articles which someone has made for example I follow Trauma and Elbow. (You can also create your own collection which someone may follow (something like a trending topic on twitter or Facebook). The last important point is Journals to follow- Here multiple journals can be added ; For Example I have added Journal of Bone and Joint Surgery – American Volume, Bone and Joint Journal British , Journal of Shoulder and Elbow Surgery, Arthroscopy and Journal of Paediatric Orthopaedics ( Fig. 4,5). After Clicking on next, we have an option of either filling up a small form with name, email and then we are taken to something called as featured papers which is like the twitter feed or Facebook timeline. (Fig. 6)
It also gives you push notifications about reading for papers and also you can get CME Credits (which we are yet to use) but a feature more useful in USA.
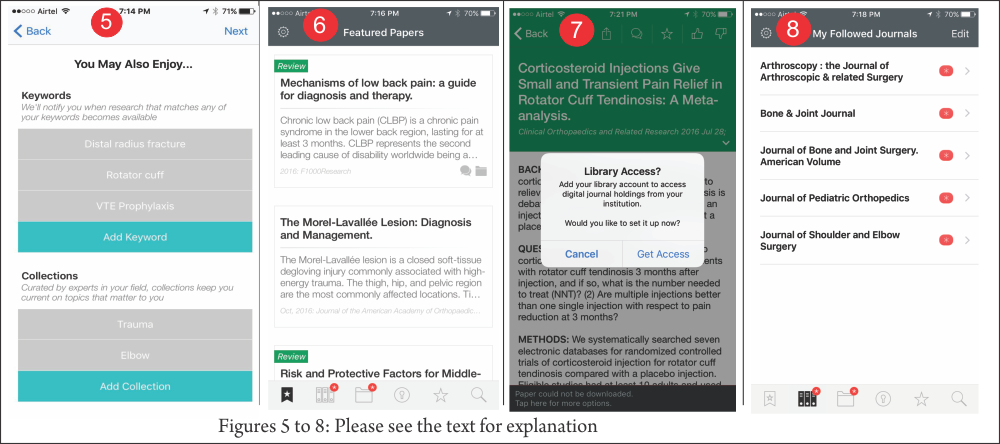
After the registration process you get the following screen options below as shown here (Fig. 7):-Featured papers; My Followed Journals; My Followed Collections; My Followed Keywords; Recently Viewed Papers; Search
My Followed Journals show all the latest articles journal wise and date wise with abstracts. My Followed Collections show the collection of articles (abstracts) which you can read. Here you also have an option of gaining library access in the app (Fig. 8) if you have off campus library access you can enter your library username and password and the app will automatically download the pdf for you if available from your library during you reading from the app. My Followed Keywords will show you relevant articles from the topics which you have been following. Recently Viewed Papers will show you your downloaded papers. Search is also very good where you can either search for papers or topics. Example: Osteoid Osteoma Search gave me very good results.
Salient Features
Things to mention here
- PDFS are available easily inside app is you have subscription or Library Access.
- Papers are Searchable
- Favourite Journals and Topics are easy to follow.
- You can always change settings and follow new journals or new topics and un-follow topics and journals which you followed earlier.
Conclusion:
Read by QxMD is one of my essential go to apps for daily reading on my interested Orthopaedic topics as well as helps me in review of literature. It helps me keeping abreast of Latest knowledge by sending me push notifications of trending articles and articles of my favourite journals and keywords. I surely recommend it to start using it now. The best part it is totally free to use and is AD- Free.
| How to Cite this article: Bijlani N, Shyam AK. Most Essential Mobile App for Trauma Surgeon – Episode 1 – Review of Mobile app – Read by QxMD. Trauma International Jan – April 2017;3(1):41-42. |
(Abstract) (Full Text HTML) (Download PDF)
Digastric Trochantric Flip OsteDigastric Trochantric Flip Osteotomy When and How to do it in Acetabular Fractures-?otomy When and How to do it in Acetabular Fractures-?
Vol 2 | Issue 2 | May – Aug 2016 | page:9-16 | U K Sadhoo
Author: U K Sadhoo [1]
[1] Nayati Hospital, Mathura, U.P. 281003
Address of Correspondence
Dr. U K Sadhoo
Nayati Hospital, Mathura, U.P. 281003
Email: uksadhoo@yahoo.com
Abstract
Acetabulum is one of the most anatomically complex regions of the body. Fractures in this area are difficult to visualise due to complex anatomy and overlaping of radiological shadows. Plain radiology od acetabular and pelvis fractures require detailied understanding of the imaging techniques and anatomy. Newer advances like 3-D CT etc have added new dimensions to the radiological assessment of acetabular fractures. Current review focusses on basic radiological principles to help the readers understand and categorised acetabulam fractures an also plan the surgical intervention.
Keywords: Acetabular fractures, radiological asessement, CT Scan.
Introduction
Acetabulum is a major weight-bearing joint, connecting Axial skeleton to lower limbs. Therefore a fracture of Acetabulum has implications for the mobility and disability for rest of life. Until the pioneering work of Judet and Letournal (1), these injuries were poorly understood and inadequately treated. Now this sub-specialty has come of age. The difficulty in understanding the nature of these injuries is the complex shape of Pelvis anatomy. Radiology not only provides an accurate assessment, it also gives a pointer to the approach and definitive treatment. Judet and Letournal classification is based on the lines produced by xray beams on the cortical surfaces in AP and two 45 degree oblique projections. Though advent of CT has enhanced our understanding, this classification remains the de facto standard. The other classifications are AO/OTA classification and the CT based Harris et al classification (3,4)
Anatomy
Acetabulum is formed by confluence of Ilium, Ischium and Pubis into an inverted horse-shoe shaped structure that is deficient inferiorly, bridged by Transverse Acetabular Ligament. The central non-articular part is known as cotyloid fossa which houses fat (Pulvinar) and Ligamentum Teres (Fig 1). Bony Acetabulum has inclination of 55-60 degrees to horizontal. This is deepened by Labrum, a soft fibro-cartilagenous structure not unlike meniscus. This increases the load-sharing area and provides additional check against dislocation.

Radiology
X-rays (Fig. 3):
Look for 6 landmarks :
1. Post. Wall : Lateral-most projection on AP and Obturator view x-ray. Seen clearly because of anteverted Acetabulum.
2. Ant. Wall : Superimposed on post. Wall, still visible as undulation line on good quality x-ray.
3. Dome : weight-bearing area of acetabulum.
3 variants :
TransTectal : through weight-bearing area
Juxta Tectal : at roof of cotyloid fossa where it joins articular area
Infra Tectal : Through floor Cotyloid fossa. Juxta and infra-Tectal don’t involve weight bearing surfaces so rarely need operative measures.
4. Tear Drop : Not an anatomical structure. Seen on AP projection. Lateral wall represents inferior-most Acetabulum articular surface, medial boundary by Quadrilateral plate.
5. Ilio-Ischial line : representing Posterior column
6. Ilio-Pectineal line : representing Anterior column
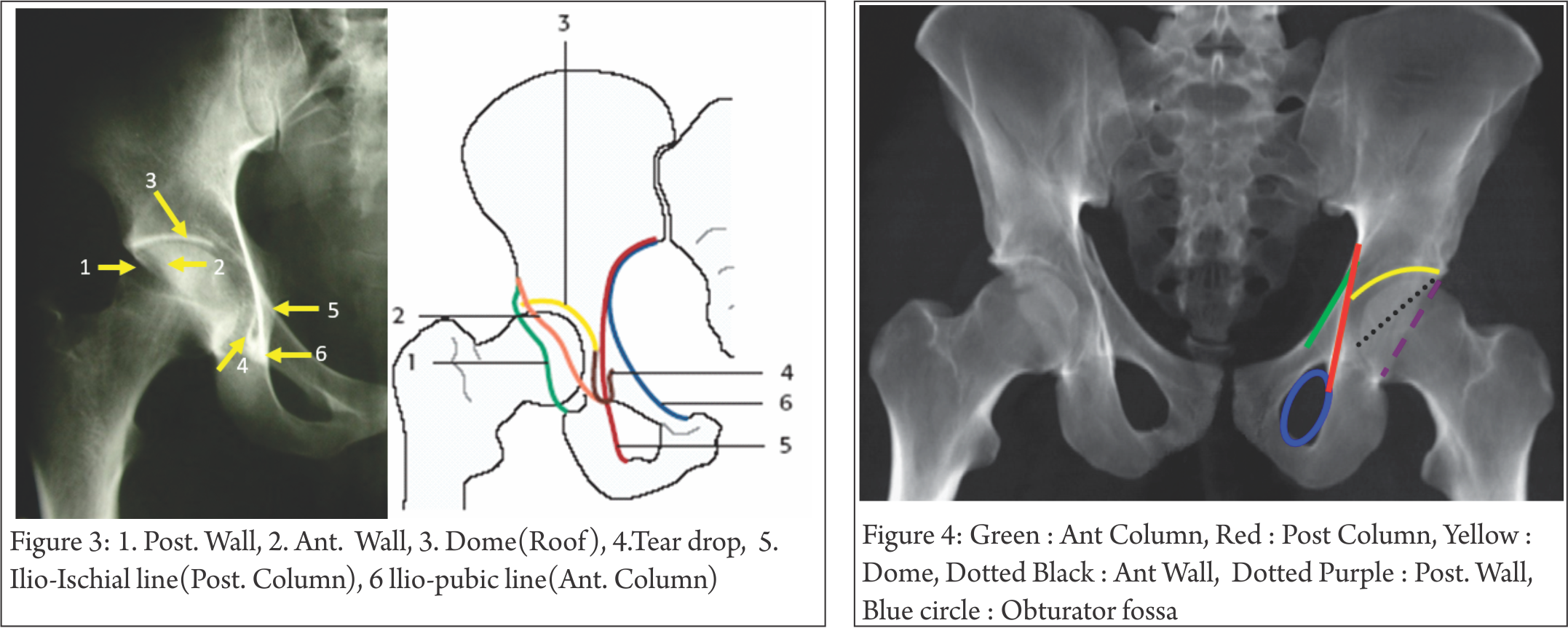
AP View 1-minute assessment (Fig. 4) : Basic, quick, cheap investigation. Look at 4 lines, 1 curve, 1 circle; it gives lot of information, enough to make a considered decision about the severity of injury and urgency of treatment. It may not pick up subtle fractures, small intra-articular fragments, marginal impaction. There is virtually nil to be deduced from x-ray about the soft tissue component of injury.
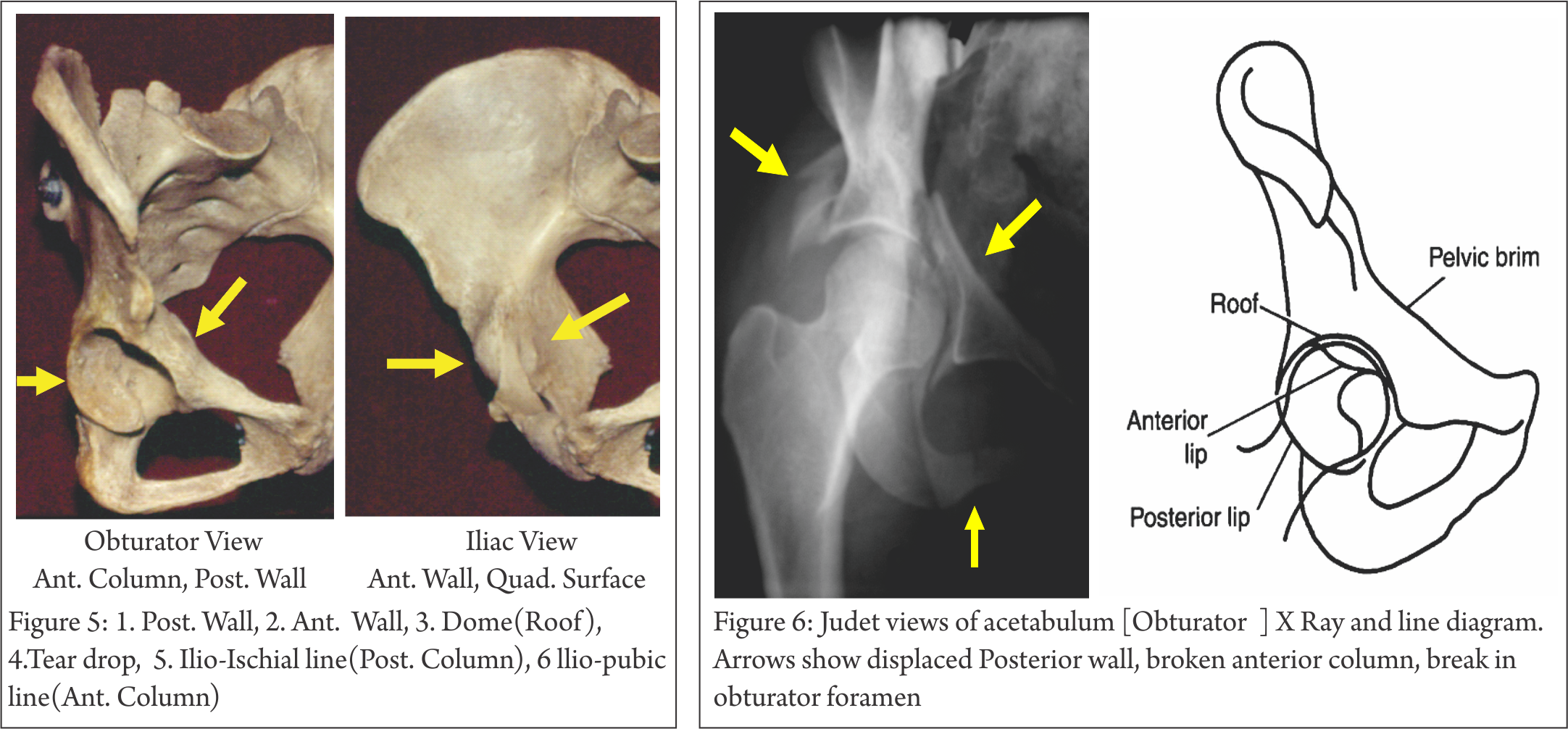
Judet Views (Fig. 5,6,7) : Patient is tilted 45 degree to horizontal, once with injured side up, then normal side up, at right angle to each other. The x ray beam is perpendicular to Horizontal, focused on affected hip in both views.
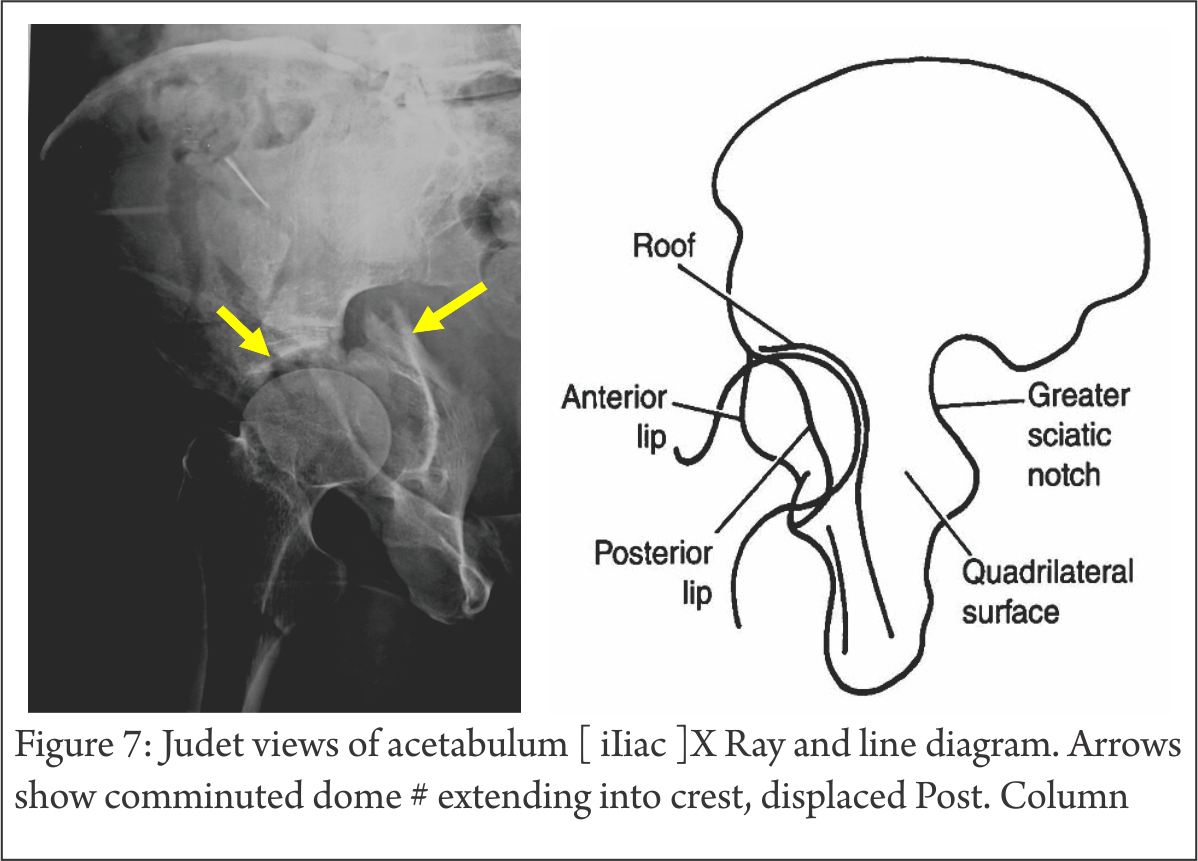
Obturator : shows Iliac wing seen end-on, Obturator foramen in full profile. (highlights Anterior column, Posterior Wall)
Iliac : shows Iliac blade, Posterior column, Ant. wall (most lateral projection), Sciatic notch, Quadrilateral plate.
Sometimes, it is not possible to do Judet views because of patient discomfort. In such cases, angiographic C-arm can be tilted, instead of the patient, to gain necessary information (7).
Planar CT scan (Fig 8,9,10) : Thin-slice scans, axial, coronal and sagittal, are invaluable tool for complete evaluation of Acetabulum fractures. It can show marginal impaction, intra-articular fragments, subtle fracture lines, and posterior Sacro-Iliac injury. It thus complements the information gained on x-rays. In addition, soft tissue injury like Morell-Lavalle lesion can be picked up on CT (or MRI).

3D CT (Fig.11): It is a reformatted image from thin sections into 3D surface-rendered images. These images are easy to understand, easy to manipulate in any direction, with or without femoral head in acetabulum. No doubt finer details like intra-articular bone pieces, impaction, and fine fracture lines are lost but it remains a powerful tool to have a bird’s eye-view of a very complex anatomy and injury. One major advantage is the ability to process data into reformatted images (Fig.12) to appear as planar AP or Judet views without the need to move or tilt the patient (5).

CT can show fracture in coronal or sagittal planes; it can also be used with artefact-suppression software for post–op evaluation of adequacy of reduction, intra-articular metal or loose bone pieces (Fig 13). The fracture lines through the Dome need understanding to interpret the diagnosis correctly (Fig 14).
Proximal 10mm of Axial CT also corresponds to the weight-bearing Dome (6). Therefore, if a fracture does not involve the proximal 10mm of Acetabulum, conservative treatment is indicated.

Judet and Letournal Classification:
Before discussing Classification, it is important to keep the following points in mind:
-Fractures are described with respect to a lateral-facing Acetabulum (Fig 1). This is quite different from real-life situation in which Acetabulum is tilted anteriorly and inferiorly. Therefore, a Transverse fracture orients in oblique-sagittal plane in a Pelvis-AP x-ray than a horizontal line.
-Walls are part of the column (Fig 2). Therefore, it is possible to break either wall or column or both simultaneously. For a column to break, exit line is through Obturator oval in most, but not all, cases. Add to this, part or complete Transverse # element and many possibilities emerge.

10 fracture patterns are recognized (fig. 15, 16); 5 elementary and 5 associated which are combination of one or more of elementary pattern. All of them are based on the walls getting separated from columns and columns getting broken at Sciatic buttress, with transversely oriented fracture through Acetabulum completing the picture.

5 elementary types are Anterior Wall, Anterior Column, Posterior Wall, Posterior Column and Transverse fracture (Fig. 15).
5 Associated patterns (Fig. 16), as name suggests, are combination of two or more Elementary patterns. These are: Posterior wall and Column fracture, Transverse with Post Wall, T Shaped, Ant Wall/Column with Posterior Hemi-transverse and associated both column. Not every fracture can be pigeon-holed in these 10 patterns, but it is as good a working classification as any.
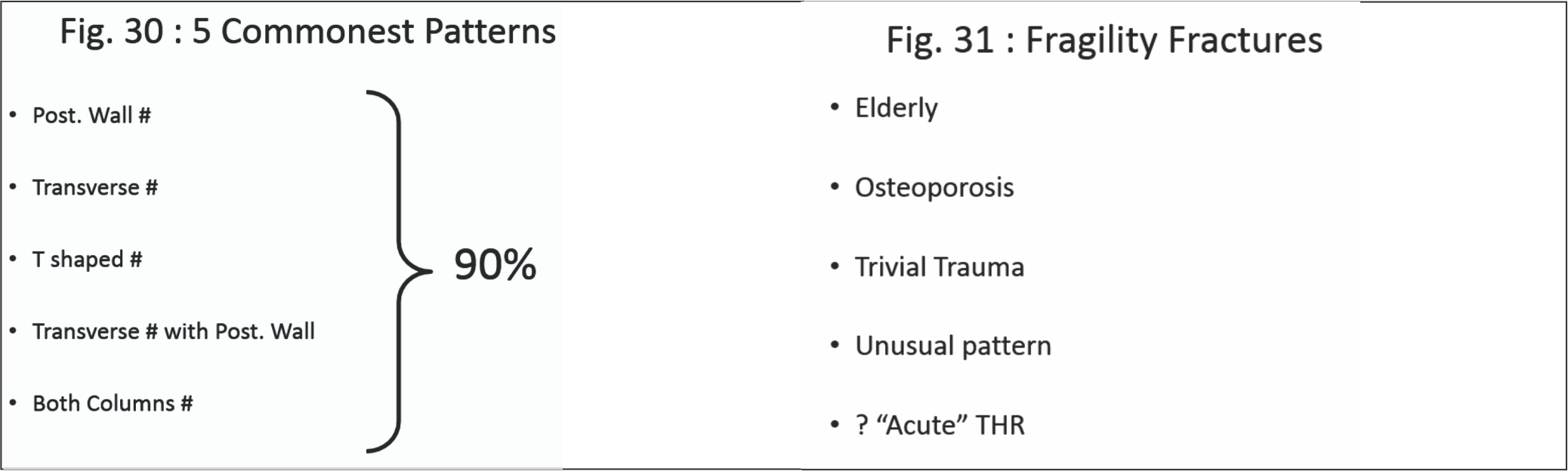
5 patterns of these 10 constitute 80% of all Acetabulum fractures: Post Wall, Transverse, Transverse with Post wall, T shaped and Both Columns (Fig. 30).(5,6)
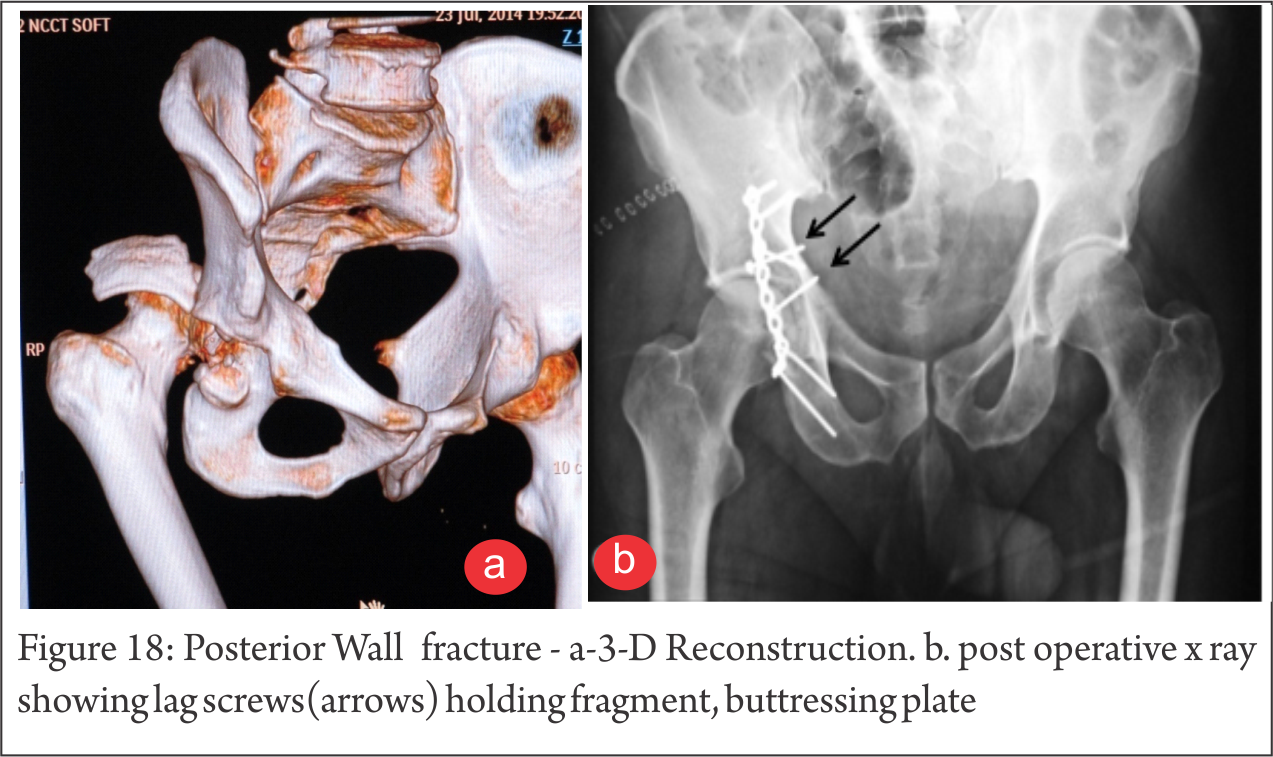
Post. Wall ( Fig.17,18) : A part of the rim with articular surface is broken. Often, it is displaced with subluxed/dislocated head Femur and best seen on Judet Obturator view (Fig 5,6). Comminution is not uncommon. Sciatic involvement is not infrequent and subtle injury even more common. On CT, marginal impaction can be picked up easily (Fig. 8).
Ant. Column (Fig 19) : Uncommon. Pure Ant. Wall fracture is even less common. It generally is a hallmark of elderly, osteoporotic individuals.

Transverse # (Fig. 20) : The fracture runs obliquely and can exit through weight-bearing Dome, at junction with Cotyloid fossa or through fossa itself. The distal fragment displaces medially and rotates. Both these factors need to be taken into account at ORIF. Though the fracture line traverses both Ilio-Pectineal and Ilio-Sciatic line, thus involving Anterior AND Post Columns, it still is not a “Both Column” Fracture, a term reserved for

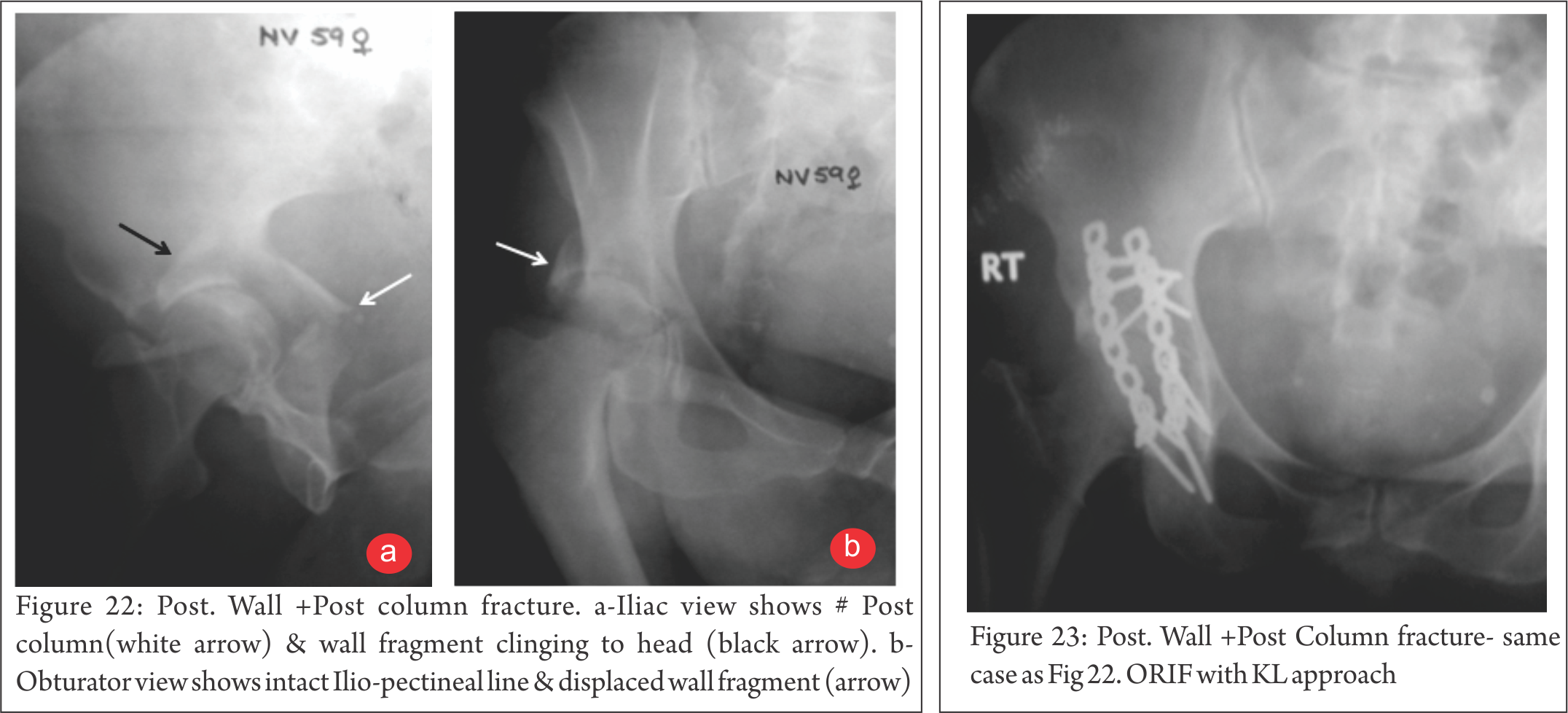
Post Wall and Column # (Fig 22, 23) : Post. Column break can occur in isolation or may be accompanied by Wall fracture. Column component exits proximally, Sciatic notch and distally, Obturator foramen. This is an unstable situation and at ORIF, Sciatic Nerve and Superior Gluteal neurovascular bundle are at risk.

Ant. Column with Post. Hemitransverse # (Fig. 24) : Not to be confused with Transverse or T #. The fracture line of Ant. Component exits obliquely compared to the straight line in Transverse #.
T-shaped # (fig. 25, 26) : The transverse component has additional break in Obturator fossa. This essentially separates Anterior and Posterior components. Therefore choosing appropriate approach is of paramount importance. Generally, the more displaced fragment decides approach. The other component is then reduced and held indirectly. Sometimes, two approaches may necessary.

Transverse with Post. Wall # (Fig. 27, 28) ; As name indicates, the post wall component makes the head displace posteriorly, often with communition.

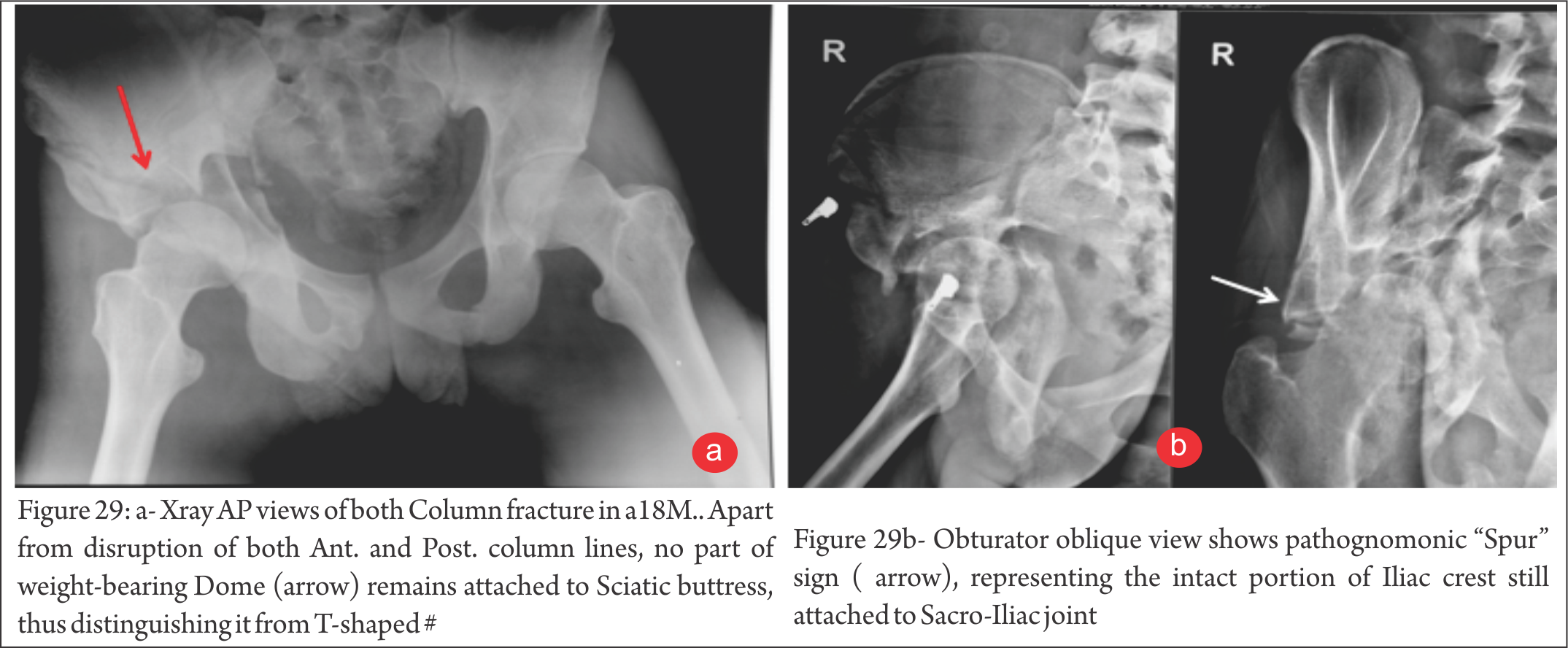
Both Column # (fig. 29) : No part of the weight-bearing Dome is connected to the Sciatic buttress. On Obturator view, “Spur” sign is characteristic of this pattern.

Fragility Fractures : (Fig. 31, 32) : With increasing longevity, the fracture patterns are also changing due to osteoporosis. Anterior wall, column injuries are common and many injuries are because of trivial fall on Greater Trochanter.

“Gull wing” sign, which shows a depressed/punched-in part of weight bearing area, is a bad prognostic indicator.
Some of these fractures can be picked only on MRI and if, despite negative X-ray, a strong suspicion prevails, MRI is indicated.
Conclusion
Acetabulum fractures need evaluation comprehensively by X-rays and CT Scans. Only then can this complex injury to a complex region be understood. Radiology not only provides assessment of injury, it helps choose best possible approach for stabilization, if indicated..
References
1. Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res 1980;(151):81–106.
2. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium: 2007—Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21(10 suppl):S1–S133.
3. Harris JH Jr, Lee JS, Coupe KJ, Trotscher T. Acetabular fractures revisited: part 1—redefinition of the Letournel anterior column. AJR Am J Roentgenol 2004;182(6):1363–1366.
4. Harris JH Jr, Coupe KJ, Lee JS, Trotscher T. Acetabular fractures revisited: part 2—a new CT-based classification. AJR Am J Roentgenol 2004;182(6):1367–1375
5.Leschka S, Alkadhi H, Boehm T, Marincek B, Wildermuth S. Coronal ultra-thick multiplanar CT reconstructions (MPR) of the pelvis in the multiple trauma patient: an alternative for the initial conventional radiograph. Rofo 2005;177(10):1405–1411.
6. Olson SA, Matta JM. The computerized tomography subchondral arc: a new method of assessing acetabular articular continuity after fracture (a preliminary report). J Orthop Trauma 1993;7(5):402–413
7. Geijer M, El-Khoury GY. Imaging of the acetabulum in the era of multidetector computed tomography. Emerg Radiol 2007;14(5):271–287
8. Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum: a meta-analysis. J Bone Joint Surg Br 2005;87(1):2–9
9. Patel NH, Hunter J, Weber TG, Routt ML Jr. Rotational imaging of complex acetabular fractures. J Orthop Trauma 1998;12(1):59–63.
| How to Cite this article: Makker H. Digastric Trochantric Flip Osteotomy –When and How to do it in Acetabular Fractures-? Trauma International Jan – April 2017;3(1):24-26. |

(Abstract) (Full Text HTML) (Download PDF)
Effectiveness of Trauma System implementation and its impact on Patient Survival Rates
Volume 2 | Issue 1 | Jan-Apr 2016 | Page 12-16|Majed Al-Mourgi1
Author: Majed Al-Mourgi[1]
Address of Correspondence
Abstract
Purpose: The purpose of this study is to assess the effectiveness and impact of trauma care system, according to the survival in the case of trauma. The main focus of this study is to evaluate the patient survival rates caused by trauma and checking either it is increasing or decreasing due to trauma system. Methods: In this research study, the quantitative data analysis approach is used to examine by the use of different statistical tools. Multiple linear regressions used to find the effect of independent variable on the dependent variable. Results: The results that obtained from the multiple statistical and different important tools must predominantly recognize the effectiveness of trauma system implementation and its impact on patient survival rates. The p-value is found to be significant as it is less than the predefined level of significance. Conclusions: The results defined the effects of trauma care system is used to increase the survival rates. With the development of trauma care center the survival rates is significantly increase and the effectiveness of the trauma care system is depending on the response time taken for trauma injury
Keywords: Patient, Quantitative Research, Survival Rates, Trauma Care System.
Introduction
Trauma is found to be the significant cause of permanent disability and death throughout the world. In USA, a wide study was conducted in order to assess the effectiveness of trauma care system in suburban and urban areas. In the study, patients were originally identified from database of discharge on basis of codes and also stratified according to the severity and type of injury, age and gender [1]. The study provides the detailed results on significant covariates known to cause the risk of death. From 5191enrolled patients were selected in the study from the total of 18,198 trauma patients who are able to meet the inclusion criteria [2]. It is found that the survival rates were significantly increased in patients by getting treatment from trauma care center than in patients getting treatment at a non- trauma care center [3].
According to the nature of trauma, the outcomes of trauma can be improved by developing certain trauma systems which is internationally known as “Trauma Care System” [4]. There are 5000- 6000 trauma patient die according to the report of RTA (Recorded Trauma Accident) [5]. For each person who dies, there are numerous thousand more persons are injured and most of them with permanent sequelae. It is also realized that 48% of the total mortality rate are caused by car accidents. These are the significant increment found in health related problems due to injury throughout the world. From the past history of trauma centre it is observed that every day death of approximately 16,000 people is realized caused by injuries. Approximately 16% of global burden of diseases is caused by injuries [5]. From which less than 90% of the total injuries burden mostly occurs within middle income and low income countries. Another significant cause of mortality in the western countries is patient’s ages from 1 to 44; however trauma strikes at all ages.
The registries of trauma play a significant role in the trauma care system, although the success of such system is hard to compute by means of related official and publications use for quality control. From the report of King Abdullah International Medical Research Center in Saudi Arabia, Trauma is the major sources of suffering, not only cause the patients leading to loss of their life but also cause temporarily or permanently disability in the patients. It is also cause to major economic loss. There is high probability for Trauma found in the young and working age adults, but it is also realized that if injury strikes at geriatric age the mortality ratio is much higher [6].
Background
Inclusive trauma system is found to be the most severe cases which are transferred to a trauma center [6]. In 2006, Utter et al. conducted a study for 2001 severe trauma patients which used inpatient databases in order to identify all severe trauma patients from 24 US states. From these 24 US states, 8 states where classified as ‘exclusive’, also another 8 states were classified as ‘more inclusive’ and the remaining 8 states were classified as ‘most inclusive’. In this study, from the total 61,496 patients with an ISS of 16 or higher were enrolled [13].
After the London bombings, analysis of resource and response studied by Aylwin et al. in 2005. This study showed a test for the trauma care system from the large resource of consumption for a very short period. In this study, researcher realized approximately 775 casualties and total 56 deaths from which approximately 53 were death at the scene. 55 patients were triaged as priority 1 and 2 severely injured. From these 55priority 1 and 2, twenty were critically injured. The realized over- triage rate was 64% and it is also observed that 3 patients died in hospital [14].
In Saudi Arabia, trauma is considered as a major problem related to public health which increases the rates of mortality and morbidity. For the socioeconomic burden, trauma causes the emotional and psychological stress on families, depletion of human resources and the healthcare facilities. In order to minimize these impacts of trauma, a national trauma care system has to be developed and implemented before it is too late to manage the further complexities of trauma in the future.
Research Design
For this study, the research design is used to define the objective of the research study. It is also defined as an effective approach that used to define the nature of research study. Past studies are significantly used to assemble the data in order to identify the nature of research study. The major aim of this research study is to assess the impact of trauma care system and its effectiveness on survival rates. Accidents are the major source of injuries or trauma. Therefore, different descriptive analysis tools are used to evaluate the occurrence of research in order to recognizing and describing the need of competitor analysis [3].
Research Questions
For this study, the research questions are used to explain the problems cause by trauma and implication of trauma care system. Inferential statistical tools are significantly used to solve these problems by collecting and analyzing the secondary data [1].
The primary objective of this population based research study is to evaluate the implication of the trauma system and its impact. For this study, the underlying research problem is to evaluate the effectiveness of the trauma care center with respect to the survival rates. The impact of trauma system for injured patients is found to be a positive sign with respect to previous researches. The major aim of this study is to analyze the impact and effectiveness of trauma care center with respect to the survival rates. For that purpose various descriptive research approaches were used to analyze the occurrence of injuries [11].
· Question 1: Does general team response in the trauma care system play an important role?
· Question 2: Are survival rates significantly increasing by the development of trauma care centers?
Research Hypothesis
In this research study, research hypothesis is used to analyze the stated problem and research design by the uses of the research hypothesis for implication of trauma management. For speculation about the research and experiment, therefore the hypothesis are stated for trauma in order to check the hypothesize research and experiment results [12]. In this study, a systematic approach is developed in a systematic way in which data is collected for the study to address the research question.
For this research study, different statistical approaches are used in order to check the research hypothesis by means of specification, prediction and testable data. The purpose of the state hypothesis is to develop a summary and also to develop the need in operational term and frame work of research [10]. For the study, the hypotheses are stated in order to check the speculation is either confirmed or rejected with the help of the statistical model. The study based on the following hypotheses:
· H1: The general team response does not play an important role of trauma care system.
· H1A: The general team response plays an important role of trauma care system.
· H2: Survival rates are not significantly increasing by the development of trauma care centers.
· H2A: Survival rates are significantly increasing by the development of trauma care centers.
Materials and Methods
Methodology is one of the most significant elements for this research study because author wants to analyze the effect of trauma care system with the help of systematic approach of research. The methodology of a research study is used to draw a design by which the study received help in executing the research. It also provides helped to complete information in an organized manner and realized proper flow to gather all the necessary information which can help to conclude the research hypotheses. Conversely, the research methodology for a specific research study provides a systematic technique in which data is collected and on the basis of collected data research questions can be evaluated or the research hypothesis can be assessed.
In this study, quantitative research methodology is used with an aim to get appropriate outcomes. The research methodology for this study refers to draw the outline in a systematic way in which the data is collected for the study with an aim to provide the valid conclusion about the research questions [6]. It can be more simply defined as the research methodology is a comprehensive plan that incorporates such procedures in order to formulate and state the research question to check the hypothesis [1].
This study is conducted with an aim to get positive increment in the survival rate after implementing trauma care system. Its effectiveness evaluated from the population based study. This study used trauma care center data which is collected throughout the year on monthly bases. The responses provided by the patients are on their traumatic experiences are collected as the quantitative data. The collected data is used to investigate by using multiple statistical techniques that provides appropriate results [12].
Data Collection
In this research study, the secondary quantitative data is used to analyze the research problem. The quantitative data analysis used to examine the effectiveness of trauma system implementation and its impact on patient survival rates. For that purpose the selected data is explained on monthly bases.
The quantitative approach based research study gives serious solutions that are important to identify the main problems of research [9]. In order to estimate appropriate results, the quantitative research is used to identify the importance of statistical significant and contract with numerical data. It totally informs the practical values of various theories that define numerous structures.
Results
Correlation
In statistics, correlation is a technique that is used to show whether and how strongly set of variables are associated with each others. Conversely, it is used to check the effect of one variable on the other variable as increase in one unit how it is affected to other variable. Correlation is defined as the degree by which two variables for the same group of elements explains a tendency to differ to each other [5].
From the outcome of table 1, the strong and positive association found between the team general response and other variables. However, there is a moderate association between the team general response and gastric tube but it is also found that the result is insignificant because the p value is greater than the predefined level of significance i.e., 0. 05.
Regression
In this study, the regression analysis tool is used in order to estimate the relationship between the variables. It is also used to analyze and forecast the post value of general team response in the trauma system on the base of past values [7].
From table 2, the model summary explains that the value of R square is near to 1 which tells us that the fitted linear regression model is accurately stated.
From table 3, the regression coefficient explains the linear relationship between the dependent and independent variable. From the table, there is a negative association found between the dependent variable and independent variable. All estimated results are significant on the bases of p value.
ANOVA
ANOVA (analysis of variance) is defined as the collection of statistical models in order to analyze the association procedure and difference between the groups means [4].
From table 4, the F stat is 779. 325 and the p value is less than the predefined level of significance therefore, the null hypotheses are rejected and conclude that the general team response for the trauma in the trauma care system play an important role and survival rates are significantly increasing by the development of trauma care centers.
Discussion
Trauma has been considered as the most leading cause of injuries and mortality among individuals particularly to those with the age below 45 years. According to this research study, the effectiveness of the trauma care system in hospitals is highly depending on the response of team. It has been observed from the above study that the excessive variables are highly effectual in defining the response time to operate trauma in the trauma care system and its impact for increasing survival rates. The correlation table portrays the positive impact of the response time because of the strong positive strong correlation realized among the selected variables. The results showed that all of these variables were positively associated with the effective team management. Also, the P value is less than the predefined level of significance i.e., 0. 05, therefore the results are significant [8]. The obtained results and statistical outcomes defined on the bases of A&E other roles and functions, Gastric Tube, Hypo/Hyper Thermia machine, Diagnostics -Radiology, Initial Vital Signs, Diagnostics -Lab, Diagnostics Fast, Diagnostics CT Scan.
Conclusion
From the above research results, according to the obtained results the increment of survival rate trauma care system plays a significant role. The study found that for severe injury case there is a very small probability of survival. The goals developed by the mutual and developed from research methodology, there are significant relationship found between the variables. In this study, the effectiveness after implementing trauma care system is realized and also its impact on patient survival rates are also found significant. From the research results there is a significance found in the effectiveness and impact of trauma system in increasing the survival rates. The different variables were analyzed to conclude the hypothesis and study provide the enough evidence to conclude that trauma care centers is significantly increasing the survival rates. The study also concludes that the early response from the team is highly effective for the trauma care system.
References
1. Barisa, M. T. , Dahdah, M. N. , Schmidt, K. , Barnes, S. A. , Dubiel, R. , Dunklin, C. , . . . & Shafi, S. . Comparative effectiveness of traumatic brain injury rehabilitation: differential outcomes across TBI model systems centers. The Journal of head trauma rehabilitation, 29(5), (2014), 451- 459.
2. Lu, M. , Althausen, P. L. , Thomas, K. C. , Shannon, S. F. , Biagi, B. N. , & Boyden, E. M. . Implant standardization for hemiarthroplasty: implementation of a pricing matrix system at a level II community based trauma system. The Journal of arthroplasty, 29(4), (2014), 781- 785.
3. Unsworth, A. , Curtis, K. , & Asha, S. E. . Treatments for blunt chest trauma and their impact on patient outcomes and health service delivery. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine,23(1), (2015), 17.
4. Porter, A. , Wyrick, D. , Bowman, S. M. , Recicar, J. , & Maxson, R. T. . The effectiveness of a statewide trauma call center in reducing time to definitive care for severely injured patients. Journal of trauma and acute care surgery, 76(4), (2014), 907- 912.
5. Cole, E. , Davenport, R. , Willett, K. , & Brohi, K. . Tranexamic Acid Use in Severely Injured Civilian Patients and the Effects on Outcomes: A Prospective Cohort Study. Annals of surgery, 261(2), (2015), 390- 394.
6. Bodnar, D. , Rashford, S. , Hurn, C. , Quinn, J. , Parker, L. , Isoardi, K. , . . . & Clarke, B. . Characteristics and outcomes of patients administered blood in the prehospital environment by a road based trauma response team. Emergency Medicine Journal, 31(7), (2014), 583- 588.
7. Church, E. C. , Selassie, A. W. , Cao, Y. , Saunders, L. L. , & Krause, J. . Accelerated death rate in population- based cohort of persons with traumatic brain injury. The Journal of head trauma rehabilitation, 29(3), (2014), E8- E19.
8. Bulger, E. M. , Fox, E. E. , del Junco, D. J. , Holcomb, J. B. , Brasel, K. J. , Hoyt, D. B. , . . . & ROC Investigators. (2015). Collider bias in trauma comparative effectiveness research: The stratification blues for systematic reviews. Injury. (2015).
9. Lansink, K. W. , & Leenen, L. P. . Do designated trauma systems improve outcome?. Current opinion in critical care, 13(6), (2007), 686- 690.
10. Yeung, H. H. , Rainer, T. H. , Gabbe, B. J. , Yuen, K. Y. , Ho, H. F. , Kam, C. W. , . . . & Graham, C. A. . A Comparison of Functional Outcome in Patients Sustaining Major Trauma: A Multicentre, Prospective, International Study. PloS one, 9(8), (2014), e103396.
11. Chiu, Y. L. , Allen, B. B. , Gerber, L. M. , Ghajar, J. , & Greenfield, J. P. . Age- specific cerebral perfusion pressure thresholds and survival in children and adolescents with severe traumatic brain injury. Pediatric critical care medicine: a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 15(1), (2014), 62.
12. Jurkovich, G. J. . Focusing on the New Reality in Trauma Care. Annals of surgery, 260(1), (2014), 22.
13. Utter, Garth H. , Ronald V. Maier, Frederick P. Rivara, Charles N. Mock, Gregory J. Jurkovich, and Avery B. Nathens. Inclusive trauma systems: do they improve triage or outcomes of the severely injured?. Journal of Trauma and Acute Care Surgery 60, no. 3 (2006): 529-537.
14. Aylwin, Christopher J. , Thomas C. Konig, Nora W. Brennan, Peter J. Shirley, Gareth Davies, Michael S. Walsh, and Karim Brohi. Reduction in critical mortality in urban mass casualty incidents: analysis of triage, surge, and resource use after the London bombings on July 7, 2005. The Lancet 368, no. 9554 (2007): 2219-2225
| How to Cite this article:.Al-Mourgi M. Effectiveness of Trauma System implementation and its impact on Patient Survival Rates. Trauma International Oct-Dec 2015;1(2):12-16. |
(Abstract) (Full Text HTML) (Download PDF)
Intramedullary Fibula with Rigid Osteosynthesis in Revision of Neglected & multiple times Operated Non Union of Long Bones
Volume 2 | Issue 1 | Jan-Apr 2016 | Page 12-16|
Author:
Address of Correspondence
Abstract
Background: Plates with Intramedullary Fibula as Strut graft(IFSG) in Non- union of long bone fractures provide most stable construct overall as fibula acts as second implant, screws have better anchorage and Very High Pull Out strength due to penetration of four cortices and Osteogenic property of the fibula is most helpful.
Aims: re-focus the importance of Non-vascularised intramedullary fibula as a second internal biologic stable splint along with rigid osteosynthesis for the treatment of difficult & neglected non -union of long bones.
Methods and Material:
15 cases (13 :2,M f) of revision surgery for the neglected & multiply operated non-union of the long bones were treated with the debridement, decortication & shingling of the fracture site with addition of the trimmed fibula (as strut) and addition of profuse bone grafting sub periosteally followed by Stable & rigid Internal Osteosynthesis by using LCP. DASH Score was used for upper limb & VAS for lower limb for assessment.
Results: Union was achieved in all patients in 12 months (Av.9-12 Months). Preoperative DASH score averaged 40.86(range 42.6-52.6). DASH score at the last follow-up averaged 20.38 points (range 16.4-24.2).difference was significant. (p=0.0001)
Conclusions: Intra medullary fibula almost works mimicking double plate & adds in the stability as it works as second plate & osteogenic property helps in the healing, not only at the fracture site but proximal & distal to it also thus avoiding SLOW-UNION at the ends of bone which are usually avascular because of the lysis. Screws have a better hold around osteoporotic bones due to four cortices hold in presence of fibula. Strong bony union can be successfully achieved in almost all cases with rigid compression at the fracture site & additional extensive cancelleous bone grafting.
Key-words: Intra- medullary Fibula ,revision Non Union,rigid Osteosynthesis
Introduction
Non -union, of Multiple times operated Long Bone fractures, poses the extreme challenge to the orthopaedic surgeons
Surgical treatment of proxiamal humeral non unions and malunions are technically challenging. Osteosynthesis with bone grafting for the treatment of nonunions is indicated in young, active patients with adequate bone stock in the proximal fragment and preservation of the glenohumeral articular surfaces[2]
Vascularised bone grafting requires surgical experience and equipment not readily available in every hospital. The technique is demanding of time and resources, and vascular thrombosis may compromise the result [5]
Iliac crest cancellous bone graft has no mechanical strength to withstand stresses prior to solid union of the fracture site and also is associated with quite significant graft harvest site morbidity. The fibula transmits one eighth of body weight and can be as useful as vascularised or non-vascularised graft in reconstruction of bony defects.
Compression plating with autogenous grafting is accepted as the gold standard method so has yielded satisfac¬tory results, with 92 to 100% healing rates
Operative treatment can be very successful when the techniques of plate-and-screw fixation are modified to address osteopenia and relative or absolute loss of bone. Healing of the fracture substantially improves function and the degree of independence[6]
Subjects and Methods: 15 patients of multiply operated non union of long bones (13 humerus, 1 femur and one distal tibia non union) were included in a study. All were treated by open reduction of the fracture, debridement and excision of the fibrosis, SHINGLING of the bone both proximally and distal to fracture site.
& osteosynthesis with strut non vascularised fibular graft and LOCKING COMPRESSION PLATE with few locking screws and rest of all are cortical screws to make it RIGID & STABLE CONSTRUCT with extensive cancelleous bone grafting 3600 surrounding the fracture site.
All patients were assessed at final follow up using D.A.S.H score for upper limb and Visual analogue score for lower limb.
All patients were followed up for 4 to 36 (average mean months is 20 months) except two patient, who are under study with last two-two and half months.
Out of 15 patients,13 were male and 2 were female. Out of 15, 13 patients had humerus non union,two had femoral mid shaft non union and remaining one had lower third distal tibia non union.
Out of the 13 humerus cases 4 had proximal humerus, 7 had mid shaft to lower third humerus(M3-L3RD) non union & two patient has non union of segmental shaft humerus fracture.
All were closed fractures except one open fracture and all had eventual atrophic non-union upon presentation. The patients had mild pain, tenderness and abnormal mobility at the non-union site (except distal tibia and middle femur), and limitation of activities of daily living. All patients had stiff¬ness of shoulder and elbow to varying degrees.
The patients with femoral non unions have constant pain at the fracture site and difficulty while bearing weight.
distal tibia non union patient had not started bearing weight as he was on fixator for three months following the Gun shot injury operated in other country.
Surgical technique:
We discussed, here (figure 1 A,1B) is a case of 52 years old male, who was operated 4 times within last 10 years & presented to us with this latest x rays showing atrophic gap Non union of the Proximal humerus.
Fracture site is exposed using previous scar in all cases as to avoid cosmetic ugly scar. The fibrous non-union and any devitalised bone were thoroughly excised and the medullary canal opened via sharp thinner humerus awl and 3.5-4.5 mm drill bits.
• 3. Preparation of the medullary canal: The humeral medullary canal was prepared to accept the bone graft. Fibrous and pseu¬doarthrosis tissue were removed completely and the medullary cavity reconstituted both proximally and distally by curettage, drill or the use of serial hand reamers (6mm-9mm). Dilate humerus medullary cavity mainly to measure the cavity
• Uniformly expanded medullary cavity by the reamers was prepared to put in the graft.(FIGU 2A,2B)
• 4. preparation of fibular graft: The mid-shaft of the fibula was then harvested under tourniquet control with care taken to identify and protect the superficial peroneal nerve. The fibular shaft of ex¬cess length was harvested so that it could be trimmed as neces¬sary. The fibula graft was trimmed so as to enable it to telescope snugly into the fragments across the fracture site. Size of fibula graft will be one smaller than Last reamer used.
If the thickness did not permit its use, it was conversely bevelled at one of the ends leaving behind proximal wider part in hollow cavity of proximal humerus and remaining part in the distal shaft. Generally in humerus ,it necessary to split fibula in the center, with oscillating saw or reciprocating saw or large bone cutter instruments to reduce the size (FIG 3C & 3D)
5. Insertion of the fibular graft: The fibular autograft was pushed into one of the fracture fragments and the exact length of graft that need¬ed trimming was assessed. Once the final shaping of the graft was done, the fracture was reduced with the intramedullary fibu¬lar graft spanning the fracture site. Confirm it is movable in the humerus medullary cavity on both sides of # easily.
• Plate fixation: Reconfirm graft moving in canal push it up all the way proximally(fig 5 A,B,C& D)
• Reduce # , distract ,hold fibula end and slowly push it distally(fig 4A,4B)
• Compress # maximally. Load cancellous graft after shingling (Fig 4 c & 4 D)
How to achieve compression at the fracture with intramedullary graft:
It is safer to do compression by Muller’s device as it is applied at the end of the bone and maximum compression can be achieved by this device. If one chooses to compress by D C P holes. Fix screw on one side of fracture , and for opposite side D C P hole should be used which is not going thru the fibula , as if fibula is fixed it will not allow compression. So under C arm see the end of fibula and go beyond it to put other D C P screw and compress . Generally one hole compression is not enough in this non union set up, so it will have to be reapeted also on 2nd hole . so it is suggested to use muller’s device or a webers device to do compression of the fracture.
A LCP was used with quadricortical screw fixation till fibula is extending. Each screw hole was drilled and tapped through four cortices, two in the fractured bone and two in the intact fib¬ula and 4. 5 mm cortical screws were inserted. End of the bone screws were from parent bone and few locking screws were used for osteoporosis.
Shoulder and elbow exercises were started a day after the opera¬tion. Lifting of weights using the operated limb was deferred for a period of three to four months or until osteo-integration of the fibular ends or fracture healing. After hospital discharge, patients were observed on a monthly basis until healing of the fracture. All pa¬tients were examined both clinically and radiologically. Fracture union was considered radiographically if callus formation was seen in three of four cortices on AP and lateral views. Clinical union was considered when the fracture site was painless.
Data collected retrospectively included grip strength, range of motion, radiographic parameters, and functional outcomes as measured by the DASH (Disabilities of the Arm, Shoulder and Hand) questionnaire.
Results: Patients were followed-up for an average of 1.5-2 years (range 1-2 years). Union was achieved in all patients in 12 months (range9-12 months ) and patients were very satisfied with the treatment. There were no perioperative complications such as wound infection, radial nerve palsy, hematoma formation. Post op two patient had discomfort over the fibular graft harvest site, and one has ASIS graft site morbidity in the form of pain mainly. One patient has persistent fracture line visible on fresh x ray at the shaft of humerus at one year follow up, but still fracture seems to be “ CLINICALLY UNITED “ as patient has painless arm movement.
Preoperative DASH score averaged 40.86(range 42.6-52.6). DASH score at the last follow-up averaged 20.38 points (range 16.4-24.2).(p=0.0001)[Table 1] V.A.S (visual analogue scale) in one patient was improved from 6-7 to 2 at the last follow up.[table 1] There was an average loss of 10-20˚ abduction and 15-20˚ flexion of the shoulder. . Range of motion of adjacent joint (knee in lower limb and elbow in upper limb) was restricted in all patients because of history of multiple surgeries and immobilization periods, but was within the functional limit in all except two patients. There was no change in shoulder rotations following surgery on the contrary three patient had pain free rotation of shoulder who had atrophic proximal humerus non union. One patient with preoperative fixed flexion deformity of elbow to varying degrees had persistence of a similar deformity at the last follow-up.
Discussion: Non -union of the long bone, after repeated surgery with multiple failed attempts poses challenging reoperation.
Healing is challenge & unpredicted with any kind of surgery and may have sub-optimal result .
We have done 15 cases of previously operated multiple times with failed union
As we have used massive mixed cortico-cancelleous auto graft in almost all cases circumferentially at the non-union site –the reason why it unites in each cases is not definite what worked out of these procedure is not predictable, like shingling & solid compression at the fracture site+cancelleous autograft Vs IMSF autograft.
Before we conclude, that fracture is united, we need evidence of circumferential callus formation , and osteo-integration, which takes long time , to be observed . Though patient is using arm almost normally, probably due to good long bony rigid fixation, and hence clinical signs of union are not convincing. This is observed most often in such multiple times operated cases only after 12 months and so we feel, 12 months minimum time should be considered for union.
The main weakness of our study is
1. Very few number of cases(only 15 cases)-so difficult to judge trend of results
2. What exactly helped union , out of everything we did.
The main strength of our study:
Our procedure can not only salvage the “function less –atrophic non united bone “—-it can even have profound effect on the overall compliance of the patient, reduce repeated morbidity from the lengthy & costly treatment like illizarov, which has frustrated outcome and at the same time gives pain free extremity function up to its fully maximum ability.
We did not seen any complication like post op infection, radial nerve palsy, implant cut through, not even
fracture of the fibula graft in any case. Two patient had fibula graft site pain, which subsided within 6 months and another female patient had ASIS graft site pain mainly which also settled within a year.
The reason for low complications in all cases may be we were lucky .
Osteoporosis, either as a result of disuse or due to
generalised metabolic causes, compounds the choice of surgical treatment in these patients. It significantly reduces the pull out strength of the screws thus increasing the chance of implant failure. Humeral nonunion in osteoporotic bone presents a reconstructive challenge for the treating orthopaedic
surgeon [3,4].
In case of non-union, mechanical stability at the fracture site and biologic re¬vitalization are keys for the management.
A non-union of a diaphyseal fracture of the humerus can present a major functional problem even in the elderly population. Advances in operative exposures combined with newer techniques of achieving stable internal fixation even in the presence of pathologic bone have enabled the surgeon to successfully treat even the most complex non unions [7]
Approximately 10% of all long-bone fractures occur in the humerus. Although primary treatment usually is successful, humeral nonunion can lead to marked morbidity and functional limitation. Complications include joint contractures of the shoulder and elbow, especially with periarticular pseudarthrosis. Marked osteopenia or bone loss, or both, often occur after fracture and after failure to achieve union. Retained implants often break, impeding fixation and requiring removal. Soft-tissue deficits and incisions from the original injury or prior surgeries also may complicate reconstruction, as can intra-articular fractures and associated nerve palsies. Successful surgical management of humeral nonunion requires stable internal fixation that allows early joint motion and uses autogenous bone graft to promote healing [8,9]
DCP with cancellous bone graft is a reliable and an effective treatment for revision of aseptic nonunion of humeral shaft fracture after surgical treatment [10,11]
We have used LCP in all 15 cases.
.There are four main indications reported in the literature for use of LCP in fractures:1)osteoporoticbone,
2) comminution, 3) intra-articular fracture, and4) short segment periarticular fracture [12,13]
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Locked plates may increasingly be indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone. Conventional plates may continue to be the fixation method of choice for periarticular fractures which demand perfect anatomical reduction and to certain types of nonunions which require increased stability for union.[14]
Conclusion:
Non-vascularised intramedullary fibula(along with debridement, decortication & shingling ) as a second internal biologic stable splint along with rigid osteosynthesis can achieve excellent Union for treatment of revision of difficult & neglected non -union of long bones.
References
1.Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, et al. Distal femoral fractures: current concepts. Re- view. J Am Acad Orthop Surg 2010;18(10):597–607
2.Agarwal A. Open reduction and internal fixation of the distal femur. In: Wiesel SW, editor. Operative techniques in orthopaedic surgery, vol. 1. Philadel- phia: Lippincott Williams & Wilkins; 2011. p. 582–4.
3.Haidukewych GJ. Temporary external fixation for the management of complex intra- and periarticular fractures of the lower extremity. J Orthop Trauma 2002;16(9):678–85.
4.SinghAK,RastogiA,SinghV.Biomechanicalcompar- ison of dynamic condylar screw and locking compres- sion plate fixation in unstable distal femoral fractures: an in vitro study. Indian J Orthop 2013;47(6):615–20.
5.Henderson CE, Lujan TJ, Kuhl LL, et al. 2010 mid- America Orthopaedic Association Physician in Training Award: healing complications are common after locked plating for distal femur fractures. Clin Orthop Relat Res 2011;469(6):1757–65.
6.Stoffel K, Dieter U, Stachowiak G, et al. Biomechanical testing of the LCP–how can stability in locked internal fixators be controlled? Injury 2003;34(Suppl 2):B11–9.
7.Prayson MJ, Datta DK, Marshall MP. Mechanical comparison of endosteal substitution and lateral plate fixation in supracondylar fractures of the femur. J Orthop Trauma 2001;15(2):96–100.
8.Beltran MJ, Gary JL, Collinge CA. Management of distal femur fractures with modern plates and nails: state of the art. J Orthop Trauma 2015;29(4):165–72.
9.Basci O, Karakaslı A, Kumtepe E, et al. Combination of anatomical locking plate and retrograde intrame- dullary nail in distal femoral fractures: comparison of mechanical stability. Eklem Hastalik Cerrahisi 2015; 26(1):21–6.
10.Suk M, Desai P. Supracondylar femur fractures. In: Archdeacon MT, editor. Prevention and manage- ment of common fracture complications. Thorofare (NJ): Slack; 2012. p. 236.
| How to Cite this article:. Bagaria V, Shah S, Sharma G. Distal Femoral Fractures: Complications and How to Avoid them?. Trauma International Jan-Apr 2016;1(2):12-16.a |
(Abstract) (Full Text HTML) (Download PDF)
Academic Partners

Indian Orthopaedic Research Group
The mission of the Indian Orthopaedic Research Group (IORG) is to promote orthopaedic research in India by helping individual orthopaedic surgeons and clinical departments throughout the country. The focus of the group is to:
– Help publish research studies in various international and national peer-reviewed journals
– Design and conduct research studies
– Establish academic research divisions in institutions that will initiate and sustain research projects
– Conduct high quality basic and clinical research studies through collaboration with various institutions and industries
– Publish peer-reviewed journals to provide a platform for Indian Orthopaedic researchers to publish their work

Sancheti Institute for Orthopaedic & Rehabilitation was established in 1965 & Sancheti Hospital for Specialized Surgery was started in 2008. Sancheti Hospital has state of the art infrastructure and equipments to conduct all the Specialities and Super-specillities services.
At Sancheti Hospital, we render highly specialized services in all areas of orthopaedic, which include Joint Replacement, Arthroscopy, Spinal Surgery, Rheumatology and Arthritis, Shoulder Surgery, Plastic and Reconstructive Surgery, Neurology, Hand and Microvascular Surgery, Faciomaxillary and Dental Surgery, Sports Injuries, Anaesthesiology and so on. “it’s a comprehensive orthopaedic super specialty hospital with all sub specialties of orthopaedic available under one roof ”
Sancheti Hospital is a final destination and a tertiary reference centre for most complicated cases in orthopaedic across the country. It was also the official reference centre for the Commonwealth Youth Games 2008-responsible for rendering all required medical services to athletes, coaches, support staff and spectators.
“Sancheti Hospital’s Sports Medicine Division caters to all the national and international teams in various sports, hence Sancheti acted as a medical partner for Commonwealth Games 2010 held in New Delhi, and the World Series Hockey held in 2012 at Pune.”
Today it stands as one of the most important centres for quality orthopaedic care, education and research. The fruits of research are seen in the form of products such as the Indus Knee Joint, India’s first completely indigenous knee implant that has helped arthritic patients, across the country to achieve pain free mobility at an affordable price.
Asia’s Leading Single Speciality Hospital for Orthopedics and Advanced Surgeries
It has received accolades worldwide for its services. According to The Week magazine, One of the top three Orthopaedic Hospitals in India. Sancheti Hosptial has been enriching lives, not only through treatment in the hospital, but through various Social Activities as well. A number of free medical camps and other social initiatives are organized on a regular basis to benefit the poor and needy.
Achievements / Awards
“Sancheti hospital “Honoured with the “Healthcare Leadership Award” citation. 20th November 2019
A Post without Image
Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.
Lorem ipsum dolor sit amet, consectetur adipisicing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
LICENSE
![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X