
Distal femur AO type A fractures – Surgical options, techniques, results and complications
Volume 1 | Issue 2 | Jan-April 2016 | Page 12-16|Anuj Agrawal
Author: Anuj Agrawal[1]
[1] Dept. of Orthopaedics, Sri Aurobindo Institute of Medical Sciences,
Indore (MP), India.
Address of Correspondence
Dr. Anuj Agrawal,
63, Moonpalace colony,
Indore (MP), India- 452009.
Email: anuj_aiims@yahoo.co.in
Abstract
Background: Distal femur fractures are challenging injuries, frequently resulting in complications like non-unions, malunions, knee stiffness and infections. This article reviews the current concepts in the surgical management of extra-articular (AO/OTA type A) fractures of the distal femur, with an evidence-based approach. The role of newer and emerging techniques is also briefly discussed.
Keywords: Supracondylar fractures of femur, AO type A fractures of distal femur, extra-articular fractures of distal femur, current concepts in distal femur fractures, recent advances in distal femur fractures.
Introduction
Fractures of the distal femur are uncommon injuries, accounting for 0.4% of all fractures[1]. However, they continue to present a challenge to the treating surgeon, with frequent complications like non-union (6%), implant failure (3.3%) and deep infections (2.4%)[2], despite significant advances in reduction techniques (MIPO/biological plating) and implant technology (locking plates) in the last decade.
The extra-articular fractures (AO/OTA type A) of the distal femur have a better prognosis than the articular (type B/C) fractures, as the joint anatomy is preserved, allowing better knee function. However, their healing too can frequently be complicated. In the younger patients, distal femur fractures result from high-energy trauma, and are frequently associated with soft tissue injury and bony comminution, affecting patient rehabilitation and stability of fixation. Whereas, in the elderly, the fractures usually result from low-energy trauma, and are frequently complicated by poor bone quality and vascularity.
We have reviewed the current practices in the management of AO/OTA type 33A fractures, including the role of newer, emerging implants and techniques.
Fracture classification
The AO/OTA classification, which is currently the universally accepted classification for distal femur fractures, divides the extra-articular type A fractures into 3 further groups and 9 sub-groups, with further qualifications[3]. 33A3.1 fractures are apophyseal fractures of the medial or lateral epicondyles of the femur, and are usually a part of complex knee dislocations or complex intra-articular fractures. When present as an isolated injury, these can usually be managed conservatively with a good outcome.
Excluding the apophyseal fractures, type A fractures are further subclassified as simple (A1), wedge (type A2) and complex (A3) ones, according to the increasing severity of the injury. A1.2 (simple spiral/oblique), A1.3 (simple transverse) and A2.1 (intact wedge) fractures are amenable to open, anatomic reduction and compression plating, whereas the A2.2, A2.3 and A3 fractures are comminuted fractures, better suited for indirect (biological) reduction and nailing/bridge plating.
The term ‘supracondylar’ fracture of the femur has been variably used in the past, for fractures occurring within 7.5 cms4 to 9 cms5 from the articular surface of distal femur, giving rise to confusion. According to the AO/OTA classification, the ‘distal femur fractures’ are defined as those occurring within a length of bone, equivalent to the maximum condylar width, from the articular surface of distal femur. The term ‘supracondylar’ fracture of the femur is not currently favored, and should be used in a similar context, as ‘distal femur fractures’. It may be noted that, in the AO/OTA classification, any fracture extending to an end segment is classified as belonging to that segment, even if the centre of the fracture zone (which is otherwise used to define the location of the fracture) falls in the middle segment of the bone. For example, the fracture shown in Fig 1 would be classified as a 33A2.1, though the centre of the fracture falls above the distal femur region. The treatment principles of distal femur fractures described in this paper also apply to most distal femoral shaft fractures (32A2.3), the difference being nails are more commonly applicable for the latter than plates.
Surgical options and techniques
Surgical treatment is currently the standard treatment for distal femoral fractures, with the goal of providing a stable fixation to allow early mobilisation of the knee and the patient. Conservative management with a cast-brace or a prefabricated brace can be used in undisplaced or minimally displaced, simple fractures, with a high expected rate of union, and satisfactory anatomic and functional results[6]. Distal femur is the only part of the femur where brace management is still acceptable. Bracing, following a period of 4-6 weeks in cast/traction, was previously used in displaced fractures, but has now been abandoned, due to a high rate of complications like malunion and knee stiffness[7]. It may still be occasionally indicated in patients not willing/fit for surgery.
The following implants are indicated for displaced fractures of the distal femur in adults:

Table 1: Summary of the approach to extra-articular distal femur fractures according to the AO/OTA classification
Condylar buttress plates (CBP)
Condylar plates fixed with conventional (non-locking) screws were used in the past for type A/C fractures. These needed to be supplemented with a medial plate to prevent varus collapse[8], in fractures with medial comminution (A2.3, A3.2 and A3.3), and have now been replaced by locking plates.
95o angled blade plate (ABP)
This was the first fixed angle implant devised by AO for distal femoral fractures, and revolutionised their management in the 1960s. It provides excellent stability for all type A fractures, and guides the reduction of comminuted fractures (both in coronal and sagittal planes), once the blade is inserted parallel to the joint. However, being a monobloc (non-modular) implant, it is not amenable to percutaneous fixation techniques (MIPO). It has waned in popularity in recent times, due to the demanding surgical technique and excessive force (hammering) required to insert the blade portion of the plate in young patients. Such a force may disrupt the condylar mass in complex articular (C3) fractures.
Dynamic condylar screw (DCS)
DCS was devised as a modular, fixed-angle implant for proximal/distal femur, simplifying the surgical technique, as it allowed insertion of a guidewire and reaming, prior to insertion of the lag screw. However, the cost of replacing the blade with a screw is that more bone needs to be sacrificed, and one more cancellous screw needs to be inserted in the distal fragment for rotational stability in the sagittal plane. Hence, the fracture line needs to be atleast 5 cm proximal to the knee joint to allow insertion of a DCS with derotation screw, whereas only 2-3 cm of intact bone is required distally to insert an ABP. However, a low (transcondylar) fracture line is rarely seen in extra-articular fractures, being more commonly associated with complex type C fractures. Hence, DCS is applicable for most type A fractures.
A recent comparative study[9] between DCS and LISS demonstrated better results in distal femur fractures fixed with a minimally invasive technique using DCS, with a higher healing rate and lower reoperation rate, as compared to LISS plates. DCS is cost-effective and can be the implant of choice for all type A fractures, unless the bone quality is poor, mandating the use of locked plates.
Locking plates (LISS, DF-LCP, condylar LCP)
Locking plates have been the greatest revolution in implant technology in recent times. These plates are increasingly being used in osteoporotic and peri-articular fractures, as locking screws provide greater resistance to pullout in osteoporotic and cancellous bones. Moreover, locking plates are technically easier to apply and slide percutaneously, than even a DCS.
However, over-enthusiasm of surgeons and over-reliance on the new technology has led to inappropriate application of locking plates in all fracture patterns, including simple ones in which a short working length can lead to an overstiff construct. Many recent papers have highlighted the problems of asymmetric callus formation[10] and callus inhibition[11] with the use of locked plates. High rates of complications (40%), particularly non-union (20%), have been reported with the use of locked plates in distal femur fractures, with the suggested causes being mechanical, like use of stainless steel plates and an insufficient bridge span (working length of the fracture)[11]. A long working length of the plate, two to three times the working length of the fracture, is desirable, with a screw density ratio of 0.4 to 0.5, to prevent the construct from becoming too stiff.
The locking compression plate (LCP) design amalgamates the principles of both conventional and locking plates in a single design, providing an option of compression of simple fracture patterns, with the subsequent use of locking screws in the articular and/or diaphyseal segments (hybrid fixation) for increased stability. The condylar LCP is based on the design of a condylar buttress plate, while a DF-LCP is based on the design of a LISS plate (Fig 2).
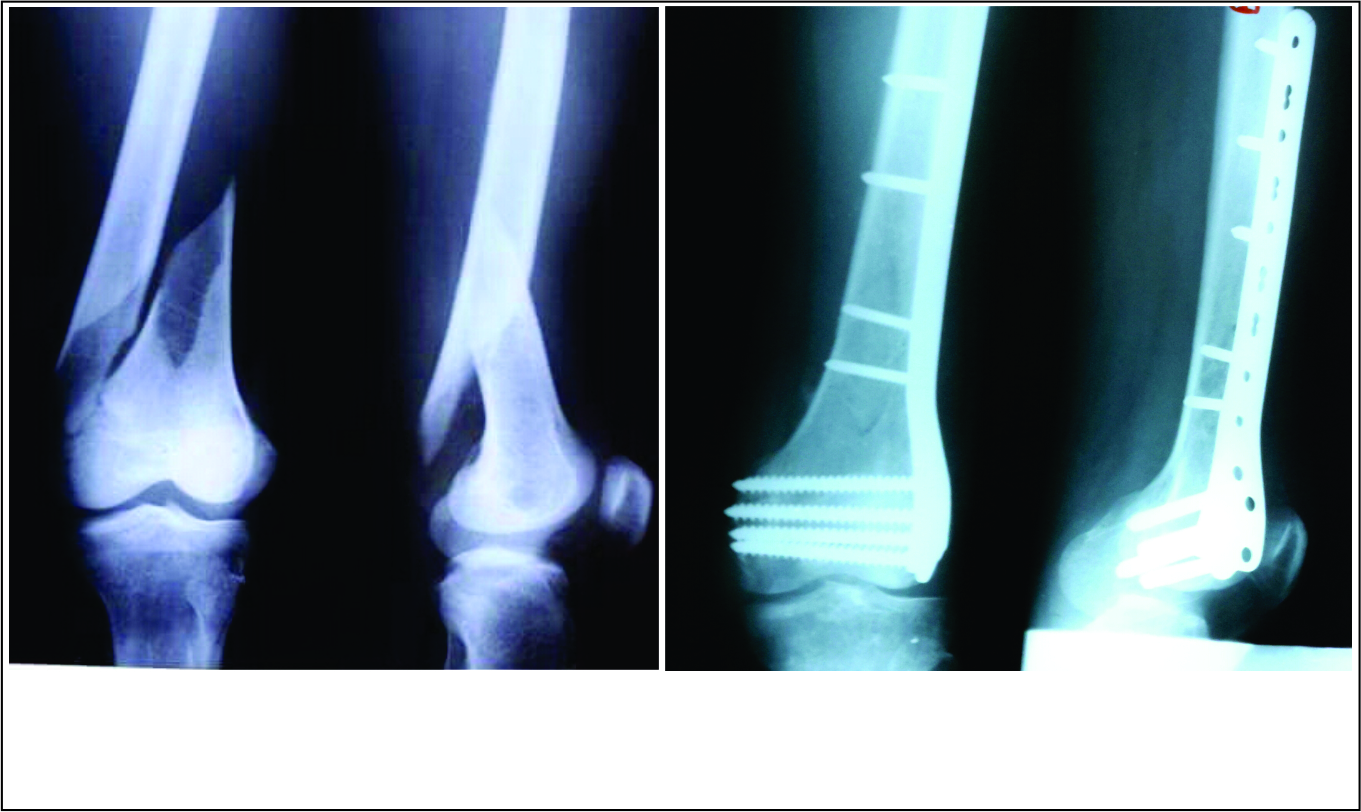
Figure 1: Treatment of simple spiral fracture of distal femur (33A2) in a 32 year old young male by open, compression plating with DF-LCP. DCS could have been used here, instead of DF-LCP. Fig 1A Pre-operative x-rays Fig 1B 3 month post-operative x-rays
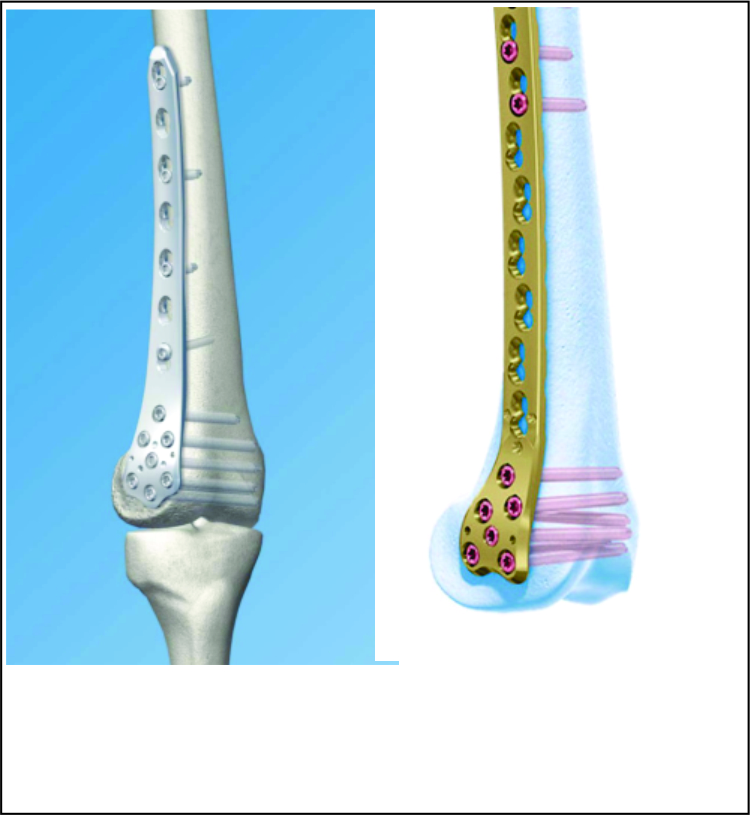
Figure 2: Designs of common locking compression plates (LCP) used for distal femur Fig 2A Distal femur Locking Compression Plate (DF-LCP) Fig 2B Condylar LCP
Antegrade/retrograde nails
Though intramedullary nails allow an indirect reduction and percutaneous fixation of distal femur fractures, providing similar advantages as MIPO, the stability provided by the nails is less than locked plates, particularly in osteoporotic bones. In a biomechanical comparison of locked plating and spiral blade retrograde nailing in 33A3 fractures, the nail constructs showed greater subsidence and reduced axial stiffness, and a higher risk of failure in osteoporotic bones[12]. In a meta-analysis, Zlowodzki et al reported a higher rate of secondary surgical procedures (23-24% versus 16%) required after nailing of distal femur fractures, with a slightly lower rate of infections (<1% versus 2%), as compared to submuscular LISS plates[2].
Antegrade nailing is applicable only for fractures more than 7-9 cm proximal to the knee joint[13], and provides a less stable construct than retrograde nailing, which provides an option to insert multiple, larger distal bolts/blade, and a thicker nail . Hence, antegrade nails are not favored in distal femur fractures, except in special situations like a stiff knee (precluding retrograde nailing), or segmental femur fractures (particularly where the proximal fracture is high in the trochanteric/subtrochanteric region).
Retrograde nails are preferred over plates for fixation of distal femur fractures by many surgeons, citing advantages like decreased blood loss, shorter operative time and reduced length of hospital stay[14]. However, they can lead to complications like anterior knee pain, malalignment, intra-articular impingement of the knee (due to incorrect technique), stress fracture at the tip of the nail, and injury to the deep femoral artery with proximal locking[15]. Malalignment is a common complication of retrograde nails, as an accurate reduction of the fracture requires a correct entry point and at times, the use of poller screws. Acharya et al[16] reported a high rate of complications like anterior knee pain (73%), knee instability (38%) and malunions (31%) after retrograde nailing of distal-third femur fracture. Thus, the use of retrograde nailing is gradually on the decline for distal femur fractures, and it should be reserved for special situations like a floating knee injury (wherein both femur and tibia can be nailed through a single incision) or a concomitant femoral neck fracture, wherein a DHS-retrograde nail ‘rendezvous’ construct[17] is advantageous (Fig 3).
 and shaft (32B2.2) fractures with a DHS-retrograde nail combination Fig 4A Pre-operative x-rays Fig 4B Immediate post-operative x-rays")
Figure 3: Rendezvous fixation of ipsilateral femoral neck (31B2.3) and shaft (32B2.2) fractures with a DHS-retrograde nail combination Fig 3A Pre-operative x-rays Fig 3B Immediate post-operative x-rays
External fixators
The use of monolateral external fixators (either spanning or non-spanning) is currently limited as a temporary fixation in polytrauma patients, fractures with vascular injury, fractures with extensive soft tissue loss and open fractures presenting late. Fractures with extensive bone loss can be definitively managed by an external fixator (a rail fixator or ring fixator) and bone transport through a subtrochanteric corticotomy (Fig 4).

Figure 4: Crush injury of left thigh in a 13 year old girl Fig 4A Clinical picture at presentation, showing extensive soft tissue injury, with loss of extensor mechanism Fig 4B Presenting x-rays, showing extensive bone loss Fig 4C Bone transport was done with application of a rail fixator primarily Fig 4D Final radiological picture after knee fusion at one year
Open versus closed reduction
There is an increasing attempt to preserve the fracture biology wherever feasible, with the use of minimally invasive plate osteosynthesis (MIPO) technique. MIPO technique has been shown to better preserve the bone circulation[18], when compared to traditional open plating, which may be particularly advantageous for callus formation with bridge plating. However, MIPO is a technically difficult procedure, involving a steep learning curve and increased radiation exposure. When done improperly, it may lead to a high rate of malalignment and malpositioning of the plate[19,20]. In a study of distal femur fractures fixed using LISS plates by MIPO technique, 38.5% of the femora were found to be malrotated >10o, as compared to the normal side, on CT scanograms.20 In an experimental study, a LISS plate, when malpositioned in external rotation to the lateral femoral surface, showed a significantly less axial stiffness and more failure rate with cyclic axial loading, as compared to a correctly positioned plate[21]. Hence, MIPO technique should be reserved for comminuted fractures (A2.2, A2.3 and A3) of the distal femur, where open reduction would be technically difficult, and endanger fragment devascularisation. Simple (A1.2, A1.3) or intact wedge (A2.1) fractures of distal femur can be anatomically reduced by an open technique, and the fracture compressed by lag screws (A1.2, A2.1) or dynamic hole compression (A1.3), using conventional plates or LCPs (hybrid fixation).
Compression plating can also be done by minimally invasive techniques (MIPO compression plating) in simple spiral/oblique fractures of the distal femur, by percutaneous reduction of the fracture with clamps, and percutaneous placement of lag screws, without opening of the fracture, followed by a neutralisation plate. However, closed reduction is usually difficult to achieve in spiral (particularly double spiral) fractures, and risks fracture of the spike(s). Moreover, the three-dimensional fracture configuration in spiral fractures requires an open approach for accurate positioning of the lag screws. Hence, we restrict the use of MIPO compression plating in long oblique fractures, favouring open compression plating for transverse, short oblique and spiral fractures. Table 1 shows our preferred approach to distal femur fractures, based on the AO/OTA fracture classification.
Locked versus hybrid plating
With the availability of locking compression plates (LCP), a locking plate can be used as a hybrid fixation (an amalgamation of traditional compression plating with locked plating). The term ‘hybrid’ construct is used in two contexts- the use of two different modes of fixation (compression and bridge techniques) in a single plate, as in segmental fractures, and secondly, the use of both locking and conventional screws in a single plate (fixing a single fracture), compressing the plate to the bone. Here, we have used the term ‘hybrid’ construct in the latter context.
Biomechanical studies have shown that only the locking screws placed in the distal segment are important for axial and torsional stiffness of the construct, with proximally unlocked (hybrid) plates showing equivalent axial and torsional stiffness, as fully locked plates[22]. Thus, the LCPs may be preferred over LISS plates in simple fracture configurations, where compression plating is required. Moreover, the use of less number of locking screws brings down the costs too. The use of plates compressed to the bone can potentially affect periosteal/cortical circulation, but this has not been proven to be detrimental for primary bone healing.
Surgical approach
The lateral approach to the distal femur is the standard surgical approach for the fixation of type A distal femur fractures. It involves a mid-lateral skin incision, incision of the iliotibial tract and atraumatic elevation of the vastus lateralis from the intermuscular septum (Fig 5A). Distal extension of the approach towards tibial tuberosity/ lateral knee arthrotomy is not required in type A fractures.
The approach can be extended proximally, if open compression plating of the fracture is planned. If a MIPO compression/bridge plating is planned, only the distal part of the approach is performed, with a minimal exposure of the lateral femoral shaft at the proximal end of the plate (to ensure proper positioning of the plate in coronal and sagittal planes) and multiple stab incisions for percutaneous screw placement (Fig 5B). There is a potential space beneath the vastus lateralis which allows percutaneous, submuscular sliding of the plate.
For retrograde nailing, a midline infra-patellar skin incision in 20-40o knee flexion is performed, with the patellar-tendon either split or retracted laterally (through a small medial arthrotomy). Some surgeons prefer to perform a complete medial parapatellar arthrotomy to ensure correct positioning of the entry point, but that is not required, except in type C fractures, where direct visualisation of the articular fracture reduction is essential.

Figure 5: Surgical approaches and reduction techniques for distal femur Fig 5A Standard open, lateral approach to distal femur Fig 5B MIPO approach to distal femur Fig 5C Use of intra-op distractor for indirect reduction Fig 5D Use of cautery cord intra-operatively to judge limb alignment
 occurring below a hip prosthesis, with pre-existing gonarthrosis Fig 7A,B Pre-operative x-rays, showing a spiral fracture line with a wedge fragment anterodistally Fig 7C,D Immediate post-operative x-rays after open, compression plating with DF-LCP, overlapping the plate over the hip stem")
Figure 6: 65 year old male with a distal femur fracture (33A2.1) occurring below a hip prosthesis, with pre-existing gonarthrosis Fig 6A,B Pre-operative x-rays, showing a spiral fracture line with a wedge fragment anterodistally Fig 6C,D Immediate post-operative x-rays after open, compression plating with DF-LCP, overlapping the plate over the hip stem
Technical pearls for close reduction
All distal femur fractures should be reduced in a slightly flexed position of the knee to relax the gastrocnemius muscle complex, allowing correction of the apex posterior deformity in the sagittal plane. A bump may be placed posteriorly at the fracture site to correct the deformity. Conventional tables are usually preferred over fracture tables.
Application of traction is central to restore limb length and allow reduction of distal femur fractures. Traction can be applied directly (by an assistant), through a pin inserted in distal femur or proximal tibia, or more effectively by the use of a femoral distractor (Fig 5C) with Schanz screws inserted proximal and distal to the fracture.
Restoration of length is easy to judge in A1/2 fractures, where direct contact between the main fracture fragments provides an easy guide. In complex A3 fractures, the restoration of limb length can be difficult, and is facilitated by draping of the normal side too, to allow direct intra-operative comparison.
Restoration of alignment in the coronal plane is paramount for a good knee function, and reduce the incidence of secondary osteoarthritis of the knee. An anatomic femorotibial angle between 5 to 10o is desirable for a normal function. The restoration of alignment is usually facilitated by a plate, if the distal blade (blade plate), lag screw (DCS) or locking screws (locking plates) of the plate, are correctly placed parallel to the knee joint. The cautery cord method (Fig 5D) can be helpful in difficult fractures, ensuring the centre of the knee lying just medial to a cautery cord placed joining the centres of the hip and the ankle joints.
Restoration of alignment in the coronal and sagittal planes is trickier with a nail, than a plate. Unlike diaphyseal fractures, a retrograde nail does not facilitate reduction of metaphyseal fractures (due to the mismatch in diameters of the proximal and distal fragments), and fracture reduction has to achieved prior to reaming and passage of the nail. Indeed, an intramedullary nail can lead to malalignment, if the entry point is not correctly made in both the coronal (in line with the centre of canal) and sagittal (just anterior to the Blumensaat’s line) planes. Placement of poller screws at the concave side of the deformity (usually medial and anterior to the guidewire to correct the commonly seen varus and apex posterior angulation deformities) is frequently required to achieve a correct alignment.
Restoration of alignment in the axial plane, i.e. rotation, is the trickiest part in comminuted fractures. Unlike diaphyseal fractures, matching the diameters of the proximal and distal fragments is not helpful in comminuted distal femur fractures, due to the differing diameters of the proximal (diaphysis) and distal (epiphysis) segments. Again, draping the normal side is helpful to restore the correct rotational alignment intra-operatively. First, the rotational profile of the lesser trochanter of the fractured limb is noted, and the normal side is then rotated to assume a rotational profile of the trochanter similar to that of the injured side. Then, the rotational profile of the foot on the normal side is noted, and the foot of the injured side is then rotated to assume a position similar to that of the normal side.
Role of newer implants and techniques
Polyaxial locked plates
Polyaxial locking plates are newer locking constructs, which allow for variable angle screw insertion, which can then be secondarily locked into the plates. Biomechanical studies have shown conflicting evidence regarding the superiority of polyaxial locking plates over uniaxial locking plates, in terms of axial/torsional stiffness and fatigue strength[23,24]. Currently, the role of polyaxial locking plates seems limited in extra-articular distal femoral fractures, except in special situations, like peri-implant fractures (around a nail or stem of a hip/knee prosthesis), where the variability in angle of insertion of locked screws id advantageous to negotiate the intra-medullary implant.
Dynamic locked plates
With increasing reports of asymmetric/insufficient callus formation and delayed/non-union with locking plates, systems have been developed to make the locking constructs more dynamic by overdrilling the near cortex, use of far cortical locking (FCL) screws, or use of dynamic locking screws[25]. Biomechanical studies comparing the stiffness and strength of these constructs in distal femur fractures are awaited. Clinical studies using FCL constructs in distal femur fractures have shown excellent rates of union with no implant failures[26,27] This technique seems to be prevent the healing problems seen with locked plates.
Implant augmentation
Even locking plates can fail in severely osteoporotic bones, due to decreased strength of the construct. Attempts to augment the fixation of locked screws by cement injection, either prior or following (through perforated cannulated screws) screw insertion, have shown success in biomechanical studies[28,29]. Implant augmentation seems a viable option for severely osteoporotic fractures, though reports of its successful clinical use are awaited.
Distal femur replacement
In low-demand elderly patients (eg. nursing home residents) with severe osteoporosis, there has been a recent trend to opt for prosthetic replacement, instead of osteosynthesis, in comminuted metaphyseal fractures, to allow earlier pain relief and immediate, full weight-bearing. However, distal femur replacement is a costly and technically challenging surgery, associated with greater morbidity/mortality, and a high rate of complications[30] (upto 50%), like peri-prosthetic fractures, infections and aseptic loosening. Hence, it needs to be cautiously used, only as a salvage procedure in low-demand patients with poor bone stock and comminuted peri-prosthetic fractures, complex intra-articular (C3) fractures, comminuted extra-articular fractures with pre-existing gonarthrosis, and resistant non-unions. Patients with relatively simple fracture patterns and pre-existing gonarthrosis can be managed with a standard total knee prosthesis with femoral stem extension (eg. the case illustrated in Fig 6 could have been managed by a primary TKR, but osteosynthesis was chosen as the patient could not afford a total knee prosthesis)[31].
Conclusion
Distal femur fractures are challenging injuries, though an excellent outcome can be expected in most extra-articular fractures with current techniques. The treating surgeon should understand the regional anatomy, fracture morphology, implant biomechanics and patient characteristics (age, functional status, bone quality) to formulate a suitable plan for an individual case.
References
1. Ehlinger M, Ducrot G, Adam P, Bonnomet F. Distal femur fractures. Surgical techniques and a review of the literature. Orthop Traumatol Surg Res. 2013 May;99(3):353-60.
2. Zlowodzki M, Bhandari M, Marek DJ, Cole PA, Kregor PJ. Operative treatment of acute distal femur fractures: systematic review of 2 comparative studies and 45 case series (1989 to 2005). J Orthop Trauma. 2006 May;20(5):366-71.
3. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium- 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007; 21(10 Suppl):S1-133.
4. Neer CS, Grantham SA, Shelton ML. Supracondylar fractures of the femur. J Bone Joint Surg. 1967;49A:591- .
5. Olerud S. Operative treatment of supracondylar-condylar fractures of the femur. J. Bone Joint Surg. 1972;54A:1015.
6. Zych GA, Zagorski JB, Latta LL. Current concepts in fracture bracing Part II: Lower extremity [Maramed Orthopedic Systems website]. Feb 1, 2001. Available at: http://www.maramed.com/articles/article_reprint_2/. Accessed December 4, 2015.
7. Sarmiento A. Functional bracing of tibial and femoral shaft fractures. Clin Orthop Rel Res. 1972;82(2).
8. Davison BL. Varus collapse of comminuted distal femur fractures after open reduction and internal fixation with a lateral condylar buttress plate. Am J Orthop (Belle Mead NJ). 2003 Jan;32(1):27-30.
9. Canadian Orthopaedic Trauma Society. Are locking constructs in distal femoral fractures always best? A prospective multicentre randomized controlled trial comparing the Less Invasive Stabilization System (LISS) to the minimally invasive Dynamic Condylar Screw system (DCS). J Orthop Trauma. 2015 Sep 29. [Epub ahead of print]
10. Lujan TJ, Henderson CE, Madey SM, Fitzpatrick DC, Marsh JL, Bottlang M. Locked plating of distal femur fractures leads to inconsistent and asymmetric callus formation. J Orthop Trauma. 2010 Mar;24(3):156-62.
11. Henderson CE, Lujan TJ, Kuhl LL, Bottlang M, Fitzpatrick DC, Marsh JL. 2010 Mid-America Orthopaedic Association Physician in Training Award: Healing Complications Are Common After Locked Plating for Distal Femur Fractures. Clinical Orthopaedics and Related Research. 2011;469(6):1757-65.
12. Assari S, Kaufmann A, Darvish K, Park J, Haw J, Safadi F, Rehman S. Biomechanical comparison of locked plating and spiral blade retrograde nailing of supracondylar femur fractures. Injury. 2013 Oct;44(10):1340-5.
13. Schatzker J. Supracondylar fractures of the distal femur. J Bone Joint Surg Br. 2004;86-B(Suppl 4):494-5.
14. Markmiller M, Konrad G, Sudkamp N. Femur- LISS and distal femoral nail for fixation of distal femoral fractures: are there differences in outcome and complications? Clin Orthop Relat Res. 2004; 426:252–7.
15. Link BC, Babst R. Current concepts in fractures of the distal femur. Acta Chir Orthop Traumatol Cech. 2012;79(1):11-20.
16. Acharya KN, Rao MR. Retrograde nailing for distal third femoral shaft fractures: a prospective study. J Orthop Surg (Hong Kong). 2006 Dec;14(3):253-8.
17. von Rüden C, Tauber M, Woltmann A, et al. Surgical treatment of ipsilateral multi-level femoral fractures. J Orthop Surg Res. 2015 Jan 24;10:7.
18. Farouk O, Krettek C, Miclau T, Schandelmaier P, Guy P, Tscherne H. Minimally invasive plate osteosynthesis: does percutaneous plating disrupt femoral blood supply less than the traditional technique? J Orthop Trauma. 1999 Aug;13(6):401-6.
19. Pakuła G, Wodzisławski W, Fudalej P, Wodzisławski J. Errors in Treatment of Fractures of Distal Femur by LISS Method (Less Invasive Stabilization System) – Single-centre Experience. Ortop Traumatol Rehabil. 2014 May-Jun;16(3):275-84.
20. Buckley R, Mohanty K, Malish D. Lower limb malrotation following MIPO technique of distal femoral and proximal tibial fractures. Injury. 2011 Feb;42(2):194-9.
21. Khalafi A, Curtiss S, Hazelwood S, Wolinsky P. The effect of plate rotation on the stiffness of femoral LISS: a mechanical study. J Orthop Trauma. 2006 Sep;20(8):542-6.
22. Cui S, Bledsoe JG, Israel H, Watson JT, Cannada LK. Locked plating of comminuted distal femur fractures: does unlocked screw placement affect stability and failure? J Orthop Trauma. 2014 Feb;28(2):90-6.
23. Wilkens KJ, Curtiss S, Lee MA. Polyaxial locking plate fixation in distal femur fractures: a biomechanical comparison. J Orthop Trauma. 2008 Oct;22(9):624-8.
24. Otto RJ, Moed BR, Bledsoe JG. Biomechanical comparison of polyaxial-type locking plates and a fixed-angle locking plate for internal fixation of distal femur fractures. J Orthop Trauma. 2009 Oct;23(9):645-52.
25. Nikhil N, Marcus W. Current concepts to reduce mechanical stiffness in locked plating constructs: a review article. Orthopaedic Research & Reviews. 2014;6:91-6.
26. Adams JD Jr, Tanner SL, Jeray KJ. Far cortical locking screws in distal femur fractures. Orthopedics. 2015 Mar;38(3):e153-6.
27. Bottlang M, Fitzpatrick DC, Sheerin D, et al. Dynamic fixation of distal femur fractures using far cortical locking screws: a prospective observational study. J Orthop Trauma. 2014 Apr;28(4):181-8.
28. Wähnert D, Hofmann-Fliri L, Richards RG, Gueorguiev B, Raschke MJ, Windolf M. Implant augmentation: adding bone cement to improve the treatment of osteoporotic distal femur fractures: a biomechanical study using human cadaver bones. Medicine (Baltimore). 2014 Nov;93(23):e166.
29. Wähnert D, Lange JH, Schulze M, Lenschow S, Stange R, Raschke MJ. The potential of implant augmentation in the treatment of osteoporotic distal femur fractures: a biomechanical study. Injury. 2013 Jun;44(6):808-12.
30. Fakler JK, Hepp P, Marquaß B, von Dercks N, Josten C. [Is distal femoral replacement an adequate therapeutic option after complexfractures of the distal femur?]. Z Orthop Unfall. 2013 Apr;151(2):173-9.
31. Choi N-Y, Sohn J-M, Cho S-G, Kim S-C, In Y. Primary Total Knee Arthroplasty for Simple Distal Femoral Fractures in Elderly Patients with Knee Osteoarthritis. Knee Surg Relat Res. 2013;25(3):141-6.
| How to Cite this article: Agrawal A. Distal femur AO type A fractures – Surgical options, techniques, results and complications. Trauma International. Jan-Apr 2016;2(1):12-16. |

Dr. Anuj Agrawal