
Functional Outcome of Unstable Intertrochanteric Femur Fracture Patients Treated with Trochanteric Fixation Nail
Vol 3 | Issue 1 | Jan – Apr 2017 | page:32-37| Yashwant J Mahale ,Vikram Vilasrao Kadu
Author: Yashwant J Mahale [1] ,Vikram Vilasrao Kadu [1]
[1] ACPM Medical College, Dhule – 424001 , Maharashtra India ,
Address of Correspondence
Dr. Vikram Vilasrao Kadu,
C/O Vilas Shamrao Kadu, Plot No. 20, Kadu House, Barde Layout, Friends Colony, Katol Road, Nagpur – 440 013, Maharashtra, India.
E-mail: dr.yashwant.mahale@gmail.com
Abstract
Introduction: Intertrochanteric fractures are disabling injuries that most commonly affect the elderly population. These fractures have a tremendous impact on both the health-care system and society in general. These fractures can be managed by conservative methods, but mal-union and complications of prolonged immobilization are the result. Thus, surgery by internal fixation is the ideal choice. Dynamic hip screw was the gold standard treatment for intertrochanteric fractures before intramedullary devices were developed. These devices have the advantage of being an intramedullary fixation device, shorter lever arm of devices causing less tensile strain on the implant, controlled fracture impaction due to the incorporation of sliding hip screw, shorter operative duration, and less soft tissue dissection. In view of these consideration, this study of management of unstable intertrochanteric fractures using trochanteric fixation nail (TFN) is taken up to assess the outcome in terms of adequacy of fixation and results.
Methods: In a retrospective controlled study, 40 patients of unstable intertrochanteric fracture were treated by TFN. Mean age group of the patient was 61.78 years. 26 cases showed union at 3 months, 13 cases showed union at 4 months, and 1 case showed union at 5 months duration.
Results: Functional results were assessed in the 40 cases available for follow-up. Excellent results were noted in 10 cases, good in 27 cases, fair in 3 cases, and none had poor result. Anatomical results were assessed by presence or absence of shortening and range of movements. 37 cases had good results and 3 had poor result.
Conclusion: At present, we consider that the TFN is a good minimally invasive implant for unstable intertrochanteric fracture when closed reduction is possible. Technical and mechanical complications were mostly related to the operative technique and the type of fracture and pre-operative reduction of the fracture.
Keywords: Shortening, trochanteric fixation nail, unstable intertrochanteric fractures.
What to Learn from this Article?
TFN is a novel implant based on the experience of gamma nail. Minimally invasive TFN, despite few
unfavorable results and complications is a satisfactory method in treating unstable it fractures. It requires closed monitoring during pre,
intra and post-operative period to avoid complications, which can be easily managed.
Introduction
Inter-trochanteric fracture most commonly affect the elderly population and also in young. The incidence has increased significantly during recent years due to the advancing age of the world’s energy trauma, whereas in the elderly age group most of the fractures are osteoporotic, resulting from a trivial fall. [1] These fractures have a tremendous impact on the health care system and society in general. These fractures can be managed by conservative methods, but mal-union and complications of prolonged immobilization is the end result. Thus, surgery by internal fixation is the ideal choice. DHS is the gold standard treatment for inter-trochanteric fractures. [2] In cases of unstable inter-trochanteric fractures, the incidence of limb shortening, medialization of distal fragment and implant cut-outs is high. [1] This led to the development of intramedullary devices. Numerous variations of intramedullary nails have been devised to achieve a stable fixation and early mobilisation of trochanteric fractures. Among these the trochanteric fixation nail (TFN) devised by the AO/ ASIF group in 1996 has proven to be a promising implant in per-, inter- or subtrochanteric femoral fractures. [3] These devices have the advantage of being an intermedullary fixtion device, shorter operative duration and less soft tissue dissection.
Purpose of the Study
To study the outcomes in terms of adequacy of fixation and stability and to evaluate end results
and complications.
Material and Methods
The study consisted forty cases of unstable inter-trochanteric fractures of femur treated surgically with Trochanteric fixation nailing at our institute between 2010 to 2014. The fractures were classified according to Boyd & Griffin’s classification. Type-IV cases were mainly excluded because of extension of the fracture onto the proximal shaft since problems were encountered with fixation of the distal locking screw which mainly crossed the fractured fragment while using conventional TFN (180mm). All the 40 Patients were available for follow-up.
The age of the patients in the study, ranged from 30 years to 88 years, average being 61.78 years. Out of forty patients, sixteen were females and twenty four were males. The Most common mode of Injury in our series were trivial fall accounting for 19 cases, followed by road traffic accidents in 14 cases and fall from height in 7 cases. Right side was affected in 19 cases and left in 21 cases. Our series consisted of 40 cases of unstable inter-trochanteric fractures. Inter-trochanteric fractures were classified according to Boyd & Griffin classification. Cases were followed at regular intervals. This study was conducted with due emphasis for clinical observation and analysis of result after surgical management of unstable inter-trochanteric fractures of femur with Trochanteric fixation nail. Following the treatment, patients were discharged and followed up at regular intervals for clinical and radiological evaluation. The patients were followed up till fracture union and functional recovery was achieved. If necessary, subsequent follow up was done. At the arrival of the patient with suspected trochanteric fracture, patients were resuscitated depending on their general conditions. Fractures were stabilized using skin traction, alternatively with Thomas Splint.
A thorough preoperative assessment of patients were done, which include general condition of patients, clinical and radiological assessment of fractures, type and size of fragments. Once stabilized, all the patients were shifted to ward & skin traction was applied varying on the built of the patient. Analgesics were given accordingly. Patients were evaluated for associated medical problems and reference was taken from respective departments and necessary treatment started. Associated injuries were evaluated and treated simultaneously. Functional results were assessed based on the functions gained by the patients following surgery and points were awarded accordingly. The factors taken into consideration in assessing were Hip pain, Ambulatory status, Ability to squat, Walking distance, Sitting cross legged.
Observation and Results
Surgery was performed on average of 8 days with a range of 4-14 days Due to financial constrain and other comorbid conditions. The delay was due to the general and medical conditions of the patients and managing associated injuries. Duration of surgery was longer in the initial operated cases. With frequent use of the nail system the duration has come down. Duration was longer in managing inter-trochanteric with subtrochanteric extension fractures type III, due to the difficulty in achieving anatomical reduction. Reduction was easier in type II inter-trochanteric fractures. Difficulty was noted in comminuted fractures and in cases with longer delay for surgery. Amount of blood loss was very less as compared to an average hip surgery. Blood loss was measured in terms of mop count and suction collection. The average amount of blood loss was 80 ml (range 60-120ml).
We encountered few complications in our study intra-operatively
1.Jamming of nail in the proximal fragment while insertion was noted, requiring progressive reaming of the proximal fragment and use of lesser diameter nail. 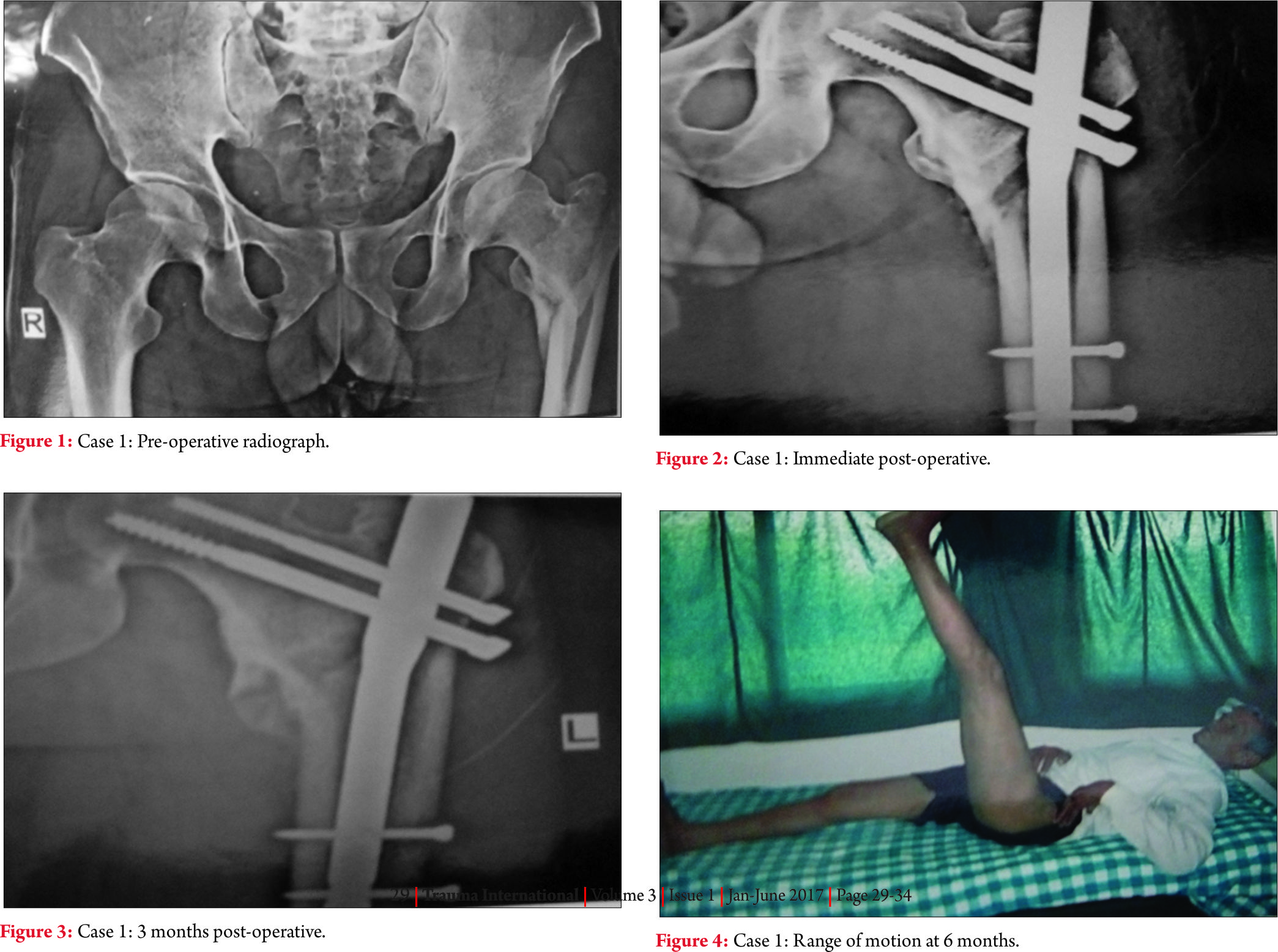
2.In one case manual distal locking had to done due to mismatch of the zig and nail, occurring intra-operatively.
3.In one case fixation of the fractures in varus angulation took place.
4.In one case iatrogenic fracture of lateral cortex of proximal fragment was noted.
Post Operative complications
In our series we had 2 cases of superficial wound infection which required appropriate intravenous antibiotics for 2 weeks period followed by 4 weeks oral antibiotics. No other complication like deep venous thrombosis, systemic infection, acute respiratory distress syndrome, fat embolism etc were noted.
Delayed complications
A case of varus collapse was noted in inter-trochanteric fracture type III with shortening of up to 1cm, due to the prominence of the screw laterally which was managed with regular follow up, to wait for the fracture to unite & implant removal. Stiffness of knee was noted in 2 cases which required vigorous physiotherapy, with full recovery of the range of movements. Stiffness of hip was noted in 2 cases due to the complications associated (Z effect and reverse Z effect) which were managed subsequently.
Duration
The average duration of hospital following surgery was 21.35 days ranging from 15-28 days. Patients were prescribed supportive drugs such as analegesic, antibiotics and other drugs as per associated medical conditions. Patients were advised to do physiotherapy such as quadriceps strengthening exercise, knee bending exercises and chest physiotherapy. Patients were instructed non weight bearing with bed rest upto 6 weeks post-operatively and were gradually made ambulatory with partial weight bearing using walker or crutches depending on the radiological signs of union and pain tolerability at subsequent follow up.
Morality
There was no mortality in this series of study.
Follow up
The average duration of follow up was 3 months ranging from 1-6 months, of which all the patients were available for follow-up.
Radiological union
Radiological union was said to be achieved on the evidences of presence of bridging callus and haziness of the fractures line on antero-posterior and lateral radiographs. 26 cases showed union at 3 months, 13 cases showed union at 4 months duration and 1 cases showed union at 5 months duration.
Anatomical result
Anatomical results were assessed by presence or absences of shortening, deformities and range of movements. 92.5% of the cases had good results and 7.5% had poor results.
Functional results
Functional results were assessed in the 40 cases available for follow up. Excellence was noted in 10 cases, good in 27 cases, fair in 3 cases and none had poor results.
Discussion
Inter-trochanteric fractures of the femur are relatively common injuries among the elderly individuals. Sometimes the associated generic problem makes it a terminal event in the lives of elderly individuals. In order to reduce the morbidity and mortality associated with conservative management of inter-trochanteric fractures, surgical management of the inter-trochanteric fractures is advocated as the best modality of management of these fractures.
Various fixation devices are available for the fixation of inter-trochanteric fractures. Most of the fixed angle nail plates were associated with many complications. Many intramedullary devices have been introduced after the development of the sliding hip screw with side plate assembly, but have their own restrictions.
In cases of unstable inter-trochanteric fractures the incidence of limb shortening, medialization of distal fragments and implant cutouts is high. This led to the development of intramedullary devices. These devices have the advantage of being an intramedullary fixation device, shorter lever arms of devices causing less tensile strain on the implant, controlled fractures impaction due to incorporation of sliding hip screw, shorter operative duration and less soft tissue dissection but however radiation exposure were high in the initial cases due to lack of experience and in cases of difficulty in reduction as compared to other modality of treatment. The average duration of radiation exposure was 60 seconds in cases of TFN which is comparatively more as compared to DHS plating which averages to 40 seconds. [4]
Amount of blood loss using trochanteric fixation nail was very less compared to an average hip surgery. Blood loss was measured in terms of mop count and suction collection. The average amount of blood loss was 80 ml (range 60-120ml) which is comparatively less as compared to DHS plating which average to 300ml. [5]
Trochanteric fixation nail attempts to combine the advantages of a sliding lag screw with those of intramedullary fixation while decreasing the moments arm as compared with that for a sliding nail plate system. It can be inserted by a closed procedure which retains the fractures haematoma, are important consideration in fracture union (MC Kibbin1978) and reduced both exposure and dissection.
Inter-trochanteric fractures almost invariability occur as a result of a fall, involving both direct and indirect forces. [6,7] Mulley and espley [8] demonstrated that inter-trochanteric fractures which occurred in hemiplegic patients sustained a trauma directly over the side secondary to impaired locomotor function and discuses osteoporosis on that side. Direct force act along the axis of the femur or directly over the greater trochanter to result in an inter-trochanteric fracture. Indirect forces include forces including pull of the iliopsoas muscle on the lesser trochanter and the abductors on the greater trochanter have also been incriminated as a cause of the fracture. [6]
When there is cortical instability on one side of a fracture due to cortical overlap or destruction, a fracture tends to collapse in the direction of such instability. [9] A truly stable inter-trochanteric fracture, therefore, is one that, when reduced, has cortical contact without a gap medially and posteriorly. [10,11]
Early operative treatment of trochanteric fractures reduces both mortality and morbidity (laskin, gruber and Zimmerman,1979) giving best chance of early independence and reducing the risk of prolonged bed rest. In the management of inter-trochanteric fractures of femur, it is important to re-establish bone to bone contact to the postero-medial cortex.
The trochanteric fixation nail (TFN) AO-ASIF device introduced in 1996 was designed to reduce the risk of implant complications. Studies have shown that screw cut out occurred by varus collapse and concomitant rotation of the femoral head around the neck axis (seral B et al 2004, sommers MB et al 2004 ) therefore in addition to the 8mm load bearing femoral neck screw, the TFN has a 6.5 mm autorotation screw to increase the rotational stability of the fragment. The derotation screw is inserted first to prevent possible rotation of the proximal fragment at the time of insertion of hip screw. An anatomic 6 degree neck valgus bend in the coronal plane, a narrower distal diameter and distal flexibility of the nail eliminates the need for routine reaming of the femoral shaft and also minimizes stress concentration and postoperative femoral shaft fractures.
The aim of our study was also to assess the epidemiology and functional outcomes of inter-trochanteric fractures with newer method of intramedullary fixation with trochanteric fixation nail.
The Z effect was seen in one patient mainly because of comminution of the medical cortex. The postoperative reduction of the fracture was not anatomic and the proximal screws had been placed higher than the level of the tip of the nail. A possible explanation the Z- effect phenomenon is the impaction of the hip pin into the proximal hole of the nail while the neck screw is normally sliding back during the weight-bearing period. The proximal fragment and the femoral head are moved back normally, whereas the impacted hip pin protrudes through the head. The reverse Z- effect occurred with the movement of the hip pin towards the lateral side. The mechanism is similar, but here the hip pin is sliding back, whereas the neck screw remains impacted to the hole of the nail.
Failure of fixation was seen in 3 cases which included one case of z effect, one case of reserve Z effect as mentioned above and one case of varus collapse of the fracture due to excessive comminution of the fracture. All these patients were managed with regular follow up to wait for the fracture to unite & subsequently implant removal.
One case of delayed union was seen due to varus collapse of the fracture because of excessive comminution and severe osteoporosis.
In 2 of our cases we had to perform open reduction due to wide displacement of fragments, comminution of fragment and in cases with delay in surgery of days due to comorbid conditions.
Trochanteric fixation nail can be used in cases of open injuries, which as compared to closed fracture is however extremely rare. Since it is an intermedullary device, it provides better strength and stability but on the contrary when using in open injuries the wound should be devoid of any contamination and should be healthy and clean. The patient should be operated as early as possible within 6 hrs since the time of accident.
Conclusion
TFN is a novel implant based on the experience of gamma nail. In the light of these results, one can conclude that the TFN, despite few unfavourable results and complications is a satisfactory method in treating unstable IT fractures. It requires closed monitoring during pre, intra and post – operative period to avoid complications, which can be easily managed. It however requires large study population with a long term follow-up.
Reference
1.Robert W Bucholz, James D Heckman, Charles M Court-Brown, Rockwood and Greens volume 2, 6th edition; pages 1827-44.
2.GS kulkarni, Rajiv Limaye, Milind Kulkarni, ‘ intertrochanteric fractures- Current concept review’ Ind J Orth, 2006, vol 40, 16-23.
3.Boldin, Christia, Seibert, Franz J, Fankhauser, Wolfgang, Szyszkowitz, Rudolf (2003) et al. Acta Orthopaedics, 74:1, 53-58.
4.Wei-Chao Sheng, Jia-Zhen Li, Sheng-Hua Chen and Shi-Zen Zhong. International orthopaedics, vol 33, number 2, 537-42.
5.Patil Suresh S, Panghate Atul. J orthopaedics 2008, 5(3) E7.
6.Ganz R, Thomas R.J, Hammerle CP. Clin Orthop 1979; 138:30-40.
7.Cleveland, m. Bosworth, D. M and Thompson, F.R. JBJS, 29:1049-67, 1947.
8.Mulley G and Espley, A. J. Postgrad Med. J, 55:264-265, 1979.
9.Evans EM. JBJS 1949; 31B: 190-203
10.Wolfgang GL. Clinical Orthopaedics and related research 1982; 163: 148-158.
11.Sarmeinto, A. Clin.Orthop, 53:47-59, 1967.
| How to Cite this article: Mahale YJ, Kadu VV. Functional Outcome of Unstable Inter-trochanteric Femur Fracture Patients Treated with Trochanteric Fixation Nail. Trauma International Jan-Apr 2017;3(1):32-37. |
