
Intramedullary Fibula with Rigid Osteosynthesis in Revision of Neglected and Multiple times Operated Non Union of Long Bones
Vol 3 | Issue 1 | Jan – Apr 2017 | page:27-31 | Dilip D Tanna, Sangeet Gawhale, Kaustubh Shinde, Viral Gondalia, Hayoung Park, Ashok Shyam
Author: Dilip D Tanna [1], Sangeet Gawhale [1], Kaustubh Shinde [2], Viral Gondalia [1], Hayoung Park [3], Ashok Shyam [4]
[1] Saifee Hospital Medical research center, Mumbai , India.
[2] BY L Nair medical college & hospital, Mumbai
[3] Researcher Department of Orthopaedics Joint Arthritis & research Laboratory Himchan Hospital Seoul,South Korea
[4] Indian Orthopaedic Research Group, Thane & Sancheti Institute of Orthopaedics and Rehabilitation, Pune, India.
Address of Correspondence
Dr D D Tanna
3A new queens road back bay view , mama parmanand marg. Mumbai 400004
Email: ddtanna@me.com
Abstract
Background: Plates with Intramedullary Fibula as Strut graft(IFSG) in Non- union of long bone fractures provides most stable construct overall as fibula acts as second implant, screws have better anchorage and very high pull out strength due to penetration of four cortices and osteogenic property of the fibula is most helpful. The aim of this paper is to re-focus the importance of non-vascularised intramedullary fibula as a second internal biologic stable splint along with rigid osteosynthesis for the treatment of difficult and neglected non -union of long bones.
Methods and Material: 15 cases (13 :2,males: females) of revision surgery for the neglected and multiply operated non-union of the long bones were treated with the debridement, decortication and shingling of the fracture site with addition of the trimmed fibula (as intramedullary strut). Liberal cancellous bone graft was added subperiosteally with stable and rigid internal osteosynthesis by using LCP. DASH Score was used for upper limb and VAS for lower limb for assessment.
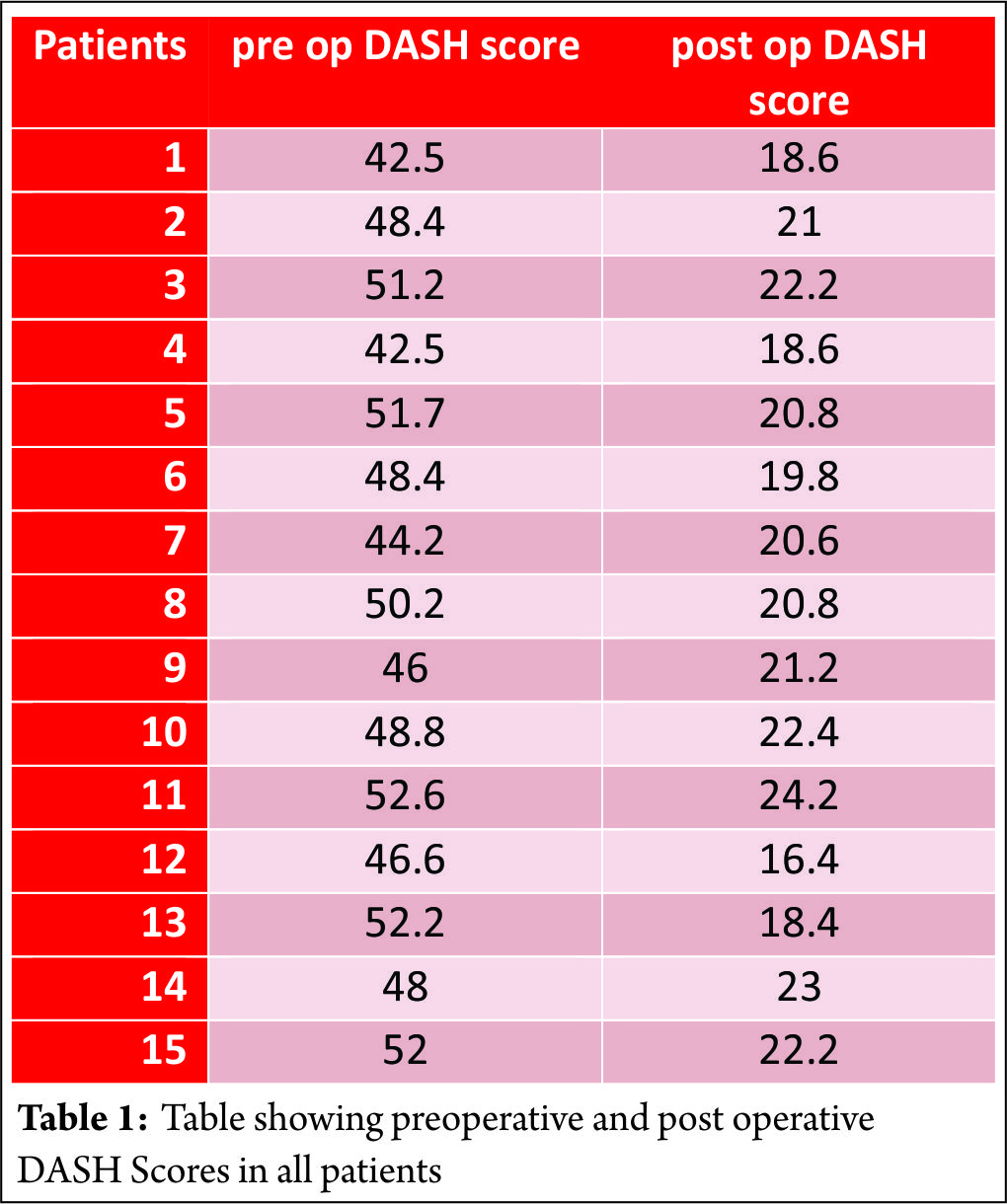
Results: Union was achieved in all patients in 12 months (range 9-12 months). Preoperative DASH score averaged 40.86(range 42.6-52.6). DASH score at the last follow-up averaged 20.38 points (range 16.4-24.2).difference was significant. (p=0.0001)
Conclusions: Intra medullary fibula almost works mimicking double plate and adds in the stability as it works as second plate. Its osteogenic property helps in the healing, not only at the fracture site but proximal and distal to it. This prevents slow union at the ends of bone which are usually avascular because of the lysis. Screws have a better hold around osteoporotic bones due to four cortices hold in presence of fibula. Strong bony union can be successfully achieved in almost all cases with rigid compression at the fracture site & additional extensive cancellous bone grafting.
Keywords: Intra- medullary Fibula ,revision non union, rigid osteosynthesis.
Introduction
Non -union, of multiple times operated long bone fractures, poses the extreme challenge to the orthopaedic surgeons. Surgical treatment of proximal humeral non unions and malunions are technically challenging. Osteosynthesis with bone grafting for the treatment of nonunions is indicated in young, active patients with adequate bone stock in the proximal fragment and preservation of the glenohumeral articular surfaces[2]
Vascularised bone grafting requires surgical experience and equipment not readily available in every hospital. The technique is demanding of time and resources, and vascular thrombosis may compromise the result [5]
Iliac crest cancellous bone graft has no mechanical strength to withstand stresses prior to solid union of the fracture site and also is associated with quite significant graft harvest site morbidity. The fibula transmits one eighth of body weight and can be as useful as vascularised or non-vascularised graft in reconstruction of bony defects.
Compression plating with autogenous grafting is accepted as the gold standard method so has yielded satisfac¬tory results, with 92 to 100% healing rates
Operative treatment can be very successful when the techniques of plate-and-screw fixation are modified to address osteopenia and relative or absolute loss of bone. Healing of the fracture substantially improves function and the degree of independence[6]
Subjects and Methods: 15 patients of multiply operated non union of long bones (13 humerus, 1 femur and one distal tibia non union) were included in a study. All were treated by open reduction of the fracture, debridement and excision of the fibrosis, shingling of the bone both proximally and distal to fracture site and osteosynthesis with strut non vascularised fibular graft and Locking Compression Plate with few locking screws and rest of all are cortical screws to make it rigid and stable construct with extensive cancelleous bone grafting 3600 surrounding the fracture site.
All patients were assessed at final follow up using D.A.S.H score for upper limb and Visual analogue score for lower limb.
All patients were followed up for 4 to 36 (average mean months is 20 months) except two patient, who are under study with last two-two and half months.
Out of 15 patients,13 were male and 2 were female. Out of 15, 13 patients had humerus non union,two had femoral mid shaft non union and remaining one had lower third distal tibia non union.
Out of the 13 humerus cases 4 had proximal humerus, 7 had mid shaft to lower third humerus(M3-L3RD) non union & two patient has non union of segmental shaft humerus fracture.
All were closed fractures except one open fracture and all had eventual atrophic non-union upon presentation. The patients had mild pain, tenderness and abnormal mobility at the non-union site (except distal tibia and middle femur), and limitation of activities of daily living. All patients had stiff¬ness of shoulder and elbow to varying degrees.
The patients with femoral non unions have constant pain at the fracture site and difficulty while bearing weight.
distal tibia non union patient had not started bearing weight as he was on fixator for three months following the Gun shot injury operated in other country.
Surgical technique:
52 years old male, who was operated 4 times within last 10 years, presented to us with this latest x rays showing atrophic gap non union of the proximal humerus (Fig 1 A,1B)

Fracture site was exposed using previous scar in all cases as to avoid cosmetic ugly scar. The fibrous non-union and any devitalised bone were thoroughly excised and the medullary canal opened via sharp thinner humerus awl and 3.5-4.5 mm drill bits.
• Preparation of the medullary canal: The humeral medullary canal was prepared to accept the bone graft. Fibrous and pseu¬doarthrosis tissue were removed completely and the medullary cavity reconstituted both proximally and distally by curettage, drill or the use of serial hand reamers (6mm-9mm). Dilate humerus medullary cavity mainly to measure the cavity
•Uniformly expanded medullary cavity by the reamers was prepared to put in the graft.(Fig 2a,2b)
•Preparation of fibular graft: The mid-shaft of the fibula was then harvested under tourniquet control with care taken to identify and protect the superficial peroneal nerve. The fibular shaft of excess length was harvested so that it could be trimmed as neces¬sary. The fibula graft was trimmed so as to enable it to telescope snugly into the fragments across the fracture site. Size of fibula graft will be one smaller than Last reamer used.
If the thickness did not permit its use, it was conversely bevelled at one of the ends leaving behind proximal wider part in hollow cavity of proximal humerus and remaining part in the distal shaft. Generally in humerus ,it necessary to split fibula in the center, with oscillating saw or reciprocating saw or large bone cutter instruments to reduce the size (Fig 3)

5. Insertion of the fibular graft: The fibular autograft was pushed into one of the fracture fragments and the exact length of graft that needed trimming was assessed. Once the final shaping of the graft was done, the fracture was reduced with the intramedullary fibular graft spanning the fracture site. Confirm it is movable in the humerus medullary cavity on both sides of fracture easily.
• Plate fixation: Reconfirm graft moving in canal push it up all the way proximally(Fig 4 – a,b)
•Reduce fracture , distract slightly hold fibula end and slowly push it distally(Fig 4c
•Compress fracture maximally and add cancellous graft after shingling (Fig 4 c & 4 d)
How to achieve compression at the fracture with intramedullary graft:
It is safer to do compression by Muller’s device as it is applied at the end of the bone and maximum compression can be achieved by this device. If one chooses to compress by D C P holes. Fix screw on one side of fracture , and for opposite side D C P hole should be used which is not going thru the fibula , as if fibula is fixed it will not allow compression. So under C arm see the end of fibula and go beyond it to put other D C P screw and compress . Generally one hole compression is not enough in this non union set up, so it will have to be repeated also on 2nd hole . so it is suggested to use Muller’s device or a webers device to do compression of the fracture.
A LCP was used with quadricortical screw fixation till fibula is extending. Each screw hole was drilled and tapped through four cortices, two in the fractured bone and two in the intact fib¬ula and 4. 5 mm cortical screws were inserted. End of the bone screws were from parent bone and few locking screws were used for osteoporosis.
Shoulder and elbow exercises were started a day after the opera¬tion. Lifting of weights using the operated limb was deferred for a period of three to four months or until osteo-integration of the fibular ends or fracture healing. After hospital discharge, patients were observed on a monthly basis until healing of the fracture. All pa¬tients were examined both clinically and radiologically. Fracture union was considered radiographically if callus formation was seen in three of four cortices on AP and lateral views. Clinical union was considered when the fracture site was painless.
Data collected retrospectively included grip strength, range of motion, radiographic parameters, and functional outcomes as measured by the DASH (Disabilities of the Arm, Shoulder and Hand) questionnaire.
Results
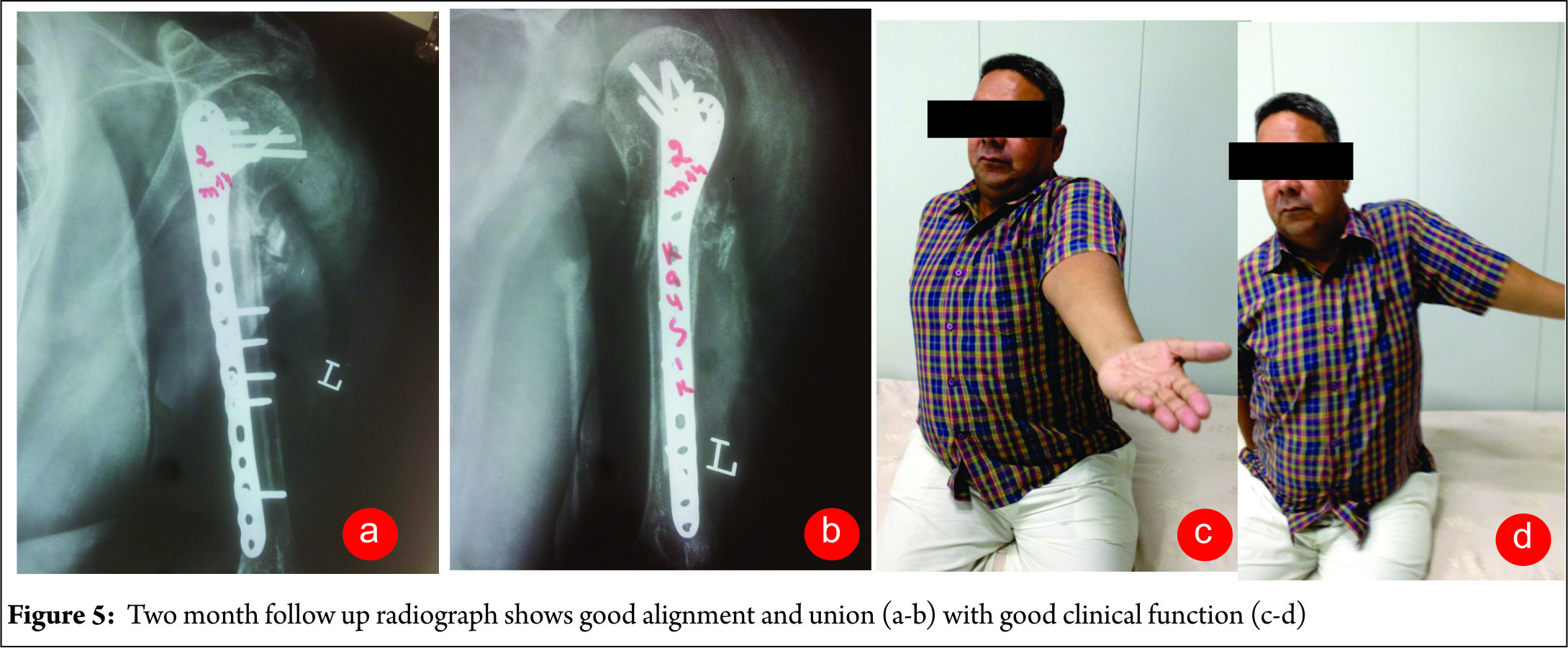
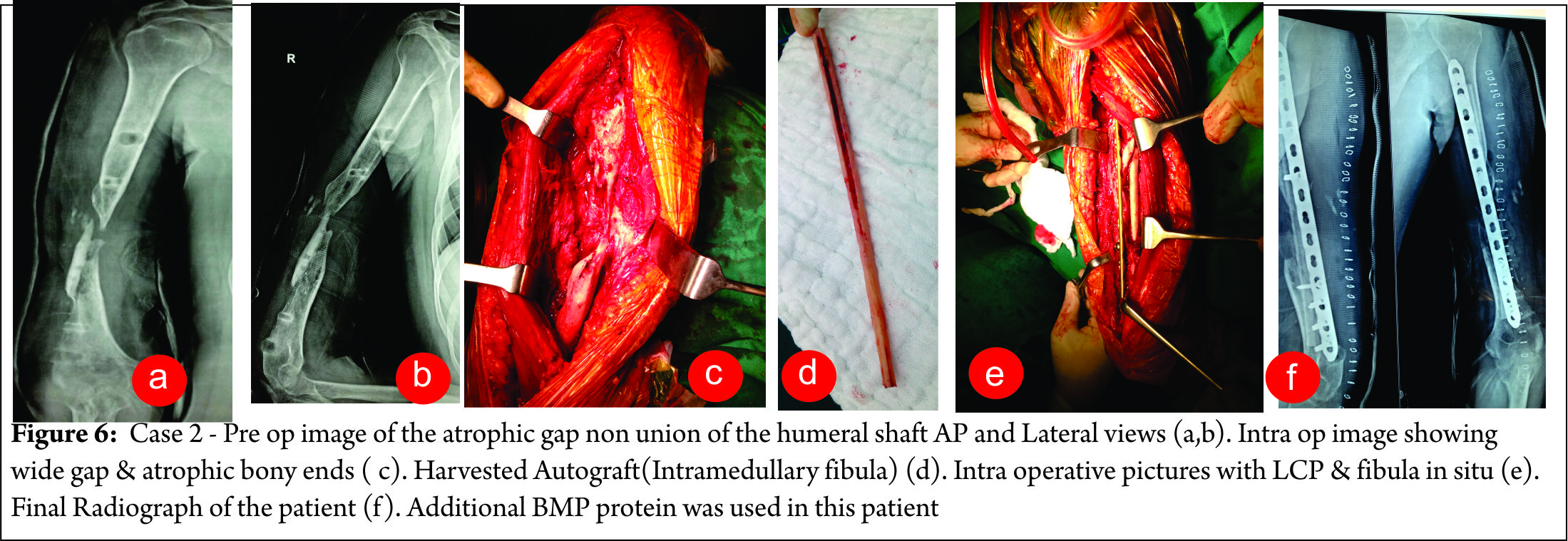
Patients were followed-up for an average of 1.5-2 years (range 1-2 years). Union was achieved in all patients in 12 months (range9-12 months ) and patients were very satisfied with the treatment Figure 5 shows long term follow up of case 1 and figure 6 shows the results in case 2. There were no perioperative complications such as wound infection, radial nerve palsy, hematoma formation. Post op two patient had discomfort over the fibular graft harvest site, and one has ASIS graft site morbidity in the form of pain mainly. One patient has persistent fracture line visible on fresh x ray at the shaft of humerus at one year follow up, but still fracture seems to be “ clinically united “ as patient has painless arm movement.
Preoperative DASH score averaged 40.86(range 42.6-52.6). DASH score at the last follow-up averaged 20.38 points (range 16.4-24.2).(p=0.0001)[Table 1] V.A.S (visual analogue scale) in one patient was improved from 6-7 to 2 at the last follow up.[table 1] There was an average loss of 10-20˚ abduction and 15-20˚ flexion of the shoulder. . Range of motion of adjacent joint (knee in lower limb and elbow in upper limb) was restricted in all patients because of history of multiple surgeries and immobilization periods, but was within the functional limit in all except two patients. There was no change in shoulder rotations following surgery on the contrary three patient had pain free rotation of shoulder who had atrophic proximal humerus non union. One patient with preoperative fixed flexion deformity of elbow to varying degrees had persistence of a similar deformity at the last follow-up.
Discussion
Non -union of the long bone, after repeated surgery with multiple failed attempts poses challenging reoperation.
Healing is challenge & unpredicted with any kind of surgery and may have sub-optimal result . We have done 15 cases of previously operated multiple times with failed union
As we have used massive mixed cortico-cancelleous auto graft in almost all cases circumferentially at the non-union site –the reason why it unites in each cases is not definite what worked out of these procedure is not predictable, like shingling & solid compression at the fracture site+cancelleous autograft Vs IMSF autograft.
Before we conclude, that fracture is united, we need evidence of circumferential callus formation , and osteo-integration, which takes long time , to be observed . Though patient is using arm almost normally, probably due to good long bony rigid fixation, and hence clinical signs of union are not convincing. This is observed most often in such multiple times operated cases only after 12 months and so we feel, 12 months minimum time should be considered for union.
The main weakness of our study is
1. Very few number of cases(only 15 cases)-so difficult to judge trend of results
2. What exactly helped union , out of everything we did is unclear
The main strength of our study:
Our procedure can not only salvage the “function less –atrophic non united bone “—-it can even have profound effect on the overall compliance of the patient, reduce repeated morbidity from the lengthy and costly treatment like ilizarov, which has frustrated outcome and at the same time gives pain free extremity function up to its fully maximum ability.
We did not seen any complication like post op infection, radial nerve palsy, implant cut through, not even
fracture of the fibula graft in any case. Two patient had fibula graft site pain, which subsided within 6 months and another female patient had ASIS graft site pain mainly which also settled within a year.
The reason for low complications in all cases may be we were lucky .
Osteoporosis, either as a result of disuse or due to
generalised metabolic causes, compounds the choice of surgical treatment in these patients. It significantly reduces the pull out strength of the screws thus increasing the chance of implant failure. Humeral nonunion in osteoporotic bone presents a reconstructive challenge for the treating orthopaedic
surgeon [3,4].
In case of non-union, mechanical stability at the fracture site and biologic re¬vitalization are keys for the management.
A non-union of a diaphyseal fracture of the humerus can present a major functional problem even in the elderly population. Advances in operative exposures combined with newer techniques of achieving stable internal fixation even in the presence of pathologic bone have enabled the surgeon to successfully treat even the most complex non unions [7]
Approximately 10% of all long-bone fractures occur in the humerus. Although primary treatment usually is successful, humeral nonunion can lead to marked morbidity and functional limitation. Complications include joint contractures of the shoulder and elbow, especially with periarticular pseudarthrosis. Marked osteopenia or bone loss, or both, often occur after fracture and after failure to achieve union. Retained implants often break, impeding fixation and requiring removal. Soft-tissue deficits and incisions from the original injury or prior surgeries also may complicate reconstruction, as can intra-articular fractures and associated nerve palsies. Successful surgical management of humeral nonunion requires stable internal fixation that allows early joint motion and uses autogenous bone graft to promote healing [8,9]
DCP with cancellous bone graft is a reliable and an effective treatment for revision of aseptic nonunion of humeral shaft fracture after surgical treatment [10,11]
We have used LCP in all 15 cases.
There are four main indications reported in the literature for use of LCP in fractures:1)osteoporotic bone,
2) comminution, 3) intra-articular fracture, and4) short segment periarticular fracture [12,13]
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Locked plates may increasingly be indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone. Conventional plates may continue to be the fixation method of choice for periarticular fractures which demand perfect anatomical reduction and to certain types of nonunions which require increased stability for union.[14]
Conclusion
Non-vascularised intramedullary fibula(along with debridement, decortication & shingling ) as a second internal biologic stable splint along with rigid osteosynthesis can achieve excellent Union for treatment of revision of difficult & neglected non -union of long bones.
References
1. Volgas DA, Stannard JP, Alonso JE. Nonunions of the humerus. Clin Orthop Relat Res. 2004 Feb;(419):46-50.
2. Cheung EV, Sperling JW. Management of proximal humeral nonunions and malunions. Orthop Clin North Am. 2008 Oct;39(4):475-82.
3. Ansell RH, Scales JT. A study of some factors which affect the strength of screws and their insertions and holding power in bone. J Biomechanics 1968;1:279–302
4. Schatzker J, Sanderson R, Murnaghan JP. The holding power of orthopaedic screws in vivo. Clin Orthop 1975;108:115–26
5. Jupiter JB. Complex non-union of the humeral diaphysis: treatment with a medial approach, an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am. 1990 Jun;72(5):701-7.
6. Ring D, Perey BH, Jupiter JB. The functional outcome of operative treatment of ununited fractures of the humeral diaphysis in older patients. J Bone Joint Surg Am 1999; 81: 177-90.
7. Jupiter JB, Von Deck M. Ununited humeral diaphyses. J Shoulder Elbow Surg 1998; 7: 644-53.
8. Pugh DMW, McKee MD. Advances in the management of humeral non-union. J Am Acad Orthop Surg 2003; 1: 48-59.
9. Weber BG. Minimax fracture fixation. AO Masters Series. Stuttgart: Thieme Medical Publishers, 2004
10. Lin CL, Fang CK, Chiu FY, Chen CM, Chen TH. Revision with dynamic compression plate and cancellous bone graft for aseptic nonunion after surgical treatment of humeral shaft fracture. J Trauma. 2009 Dec;67(6):1393-6.
11. Hierholzer C, Sama D, Toro JB, Peterson M, Helfet DL. Plate fixation of ununited humeral shaft fractures: effect of type of bone graft on healing. J Bone Joint Surg. 2006; 88A: 1442-drv7
12. SmithWR, Ziran BH,Anglen JO, et al. Locking plates: tips and tricks. J Bone Joint SurgAm 2007;89(10):2298-307. PMID:17966158.
13. Wagner M. General principles for the clinical use of the LCP. Injury 2003;34 Suppl 2:B31-42.
14. Egol KA, Kubiak EN, Fulkerson E, Kummer FJ, Koval KJ. Biomechanics of locked plates and screws. J Orthop Trauma. 2004 Sep;18(8):488-93.
| How to Cite this article: Tanna DD, Gawhale S, Shinde K, Gondalia V, Park H, Shyam AK. Intramedullary Fibula with Rigid Osteosynthesis in Revision of Neglected and multiple times Operated Non Union of Long Bones. Trauma International Jan – June 2017;3(1):27-31. |
