
The Screw Intra-medullary Elastic Nail Fixation in fresh Displaced Mid Shaft Clavicle Fractures – Technical note
Vol 2 | Issue 2 | May – Aug 2016 | page:53-55 | Wasudeo Gadegone, Vijayanad Lokhande, Yogesh Salphale
Author: Wasudeo Gadegone [1], Vijayanad Lokhande [1], Yogesh Salphale [1]
[1] GMC Chandrapur, Maharashtra, India.
[2] Shushrusha Multispecialty hospital, Chandrapur, India.
[3] Smt. Kashibai Navale Medical College and General Hospital, Pune
Address of Correspondence
Dr. W.M. Gadegone.
VivekNagar Mul-Road Chandrapur 442402, Maharashtra, India.
Email: gadegone123@yahoo.co.in
Abstract
Conservative treatment remains the gold standard in treatment of simple undisplaced midshaft clavicle fractures, but for displaced and comminuted fractures surgical intervention is appropriate especially in young active adults. Surgical stabilisation can be achieved using either a plate or an intramedullary device. One of dreaded complication of intramedullary device in migration of the implant. We have used a screw intramedullary device with screw mechanism at one end which can get hold in the medial cancellous bone, thus preventing chances of migration. This report describes the technique of using the screw intramedullary nail for displace clavicle fracture.
Keywords: clavicle fracture, intramedullary nailing.
Introduction
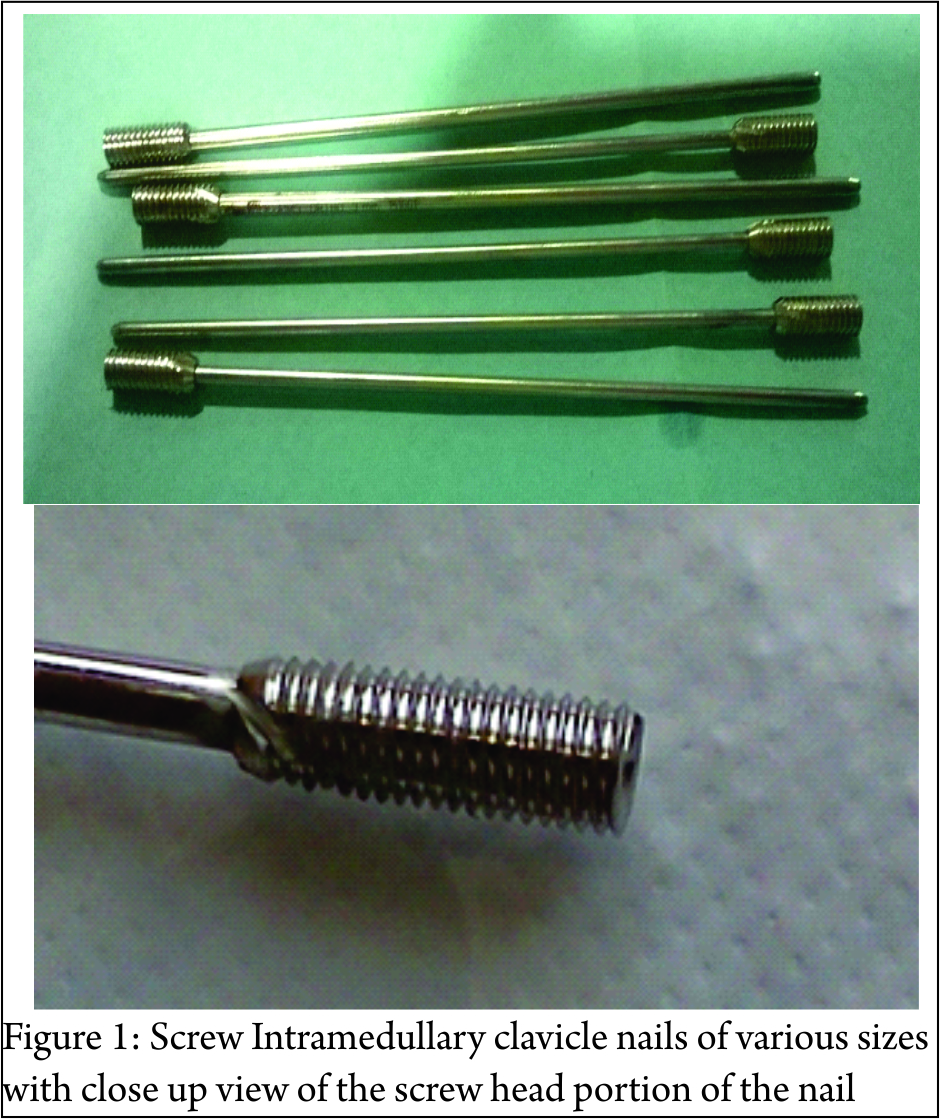
Although conservative treatment is the gold standard for clavicle fractures, there may be some issues like shoulder impairement, a bump at the fracture site that is cosmetically unacceptable or nonunions which happen when grossly displaced fractures are treated conservatively. Surgical stabilisation may be additionally indicated in cases with completely displaced fractures (gap of > 20mm), potential skin perforation, shortening of clavicle by more than 20 mm, neurovascular injury, and floating shoulder injury. Plating is an option which is used commonly, but leads to scarring and may need repeat surgery of implant removal. Intrameduallry nailing has been successfully used by few authors but has a complications like nail migration. We are using a screw intrameduallry device (Fig. 1) which anchors to the metaphyseal bone by the wide screw head at the end of the nail. This technicaal note simply describes the technique.
Implant
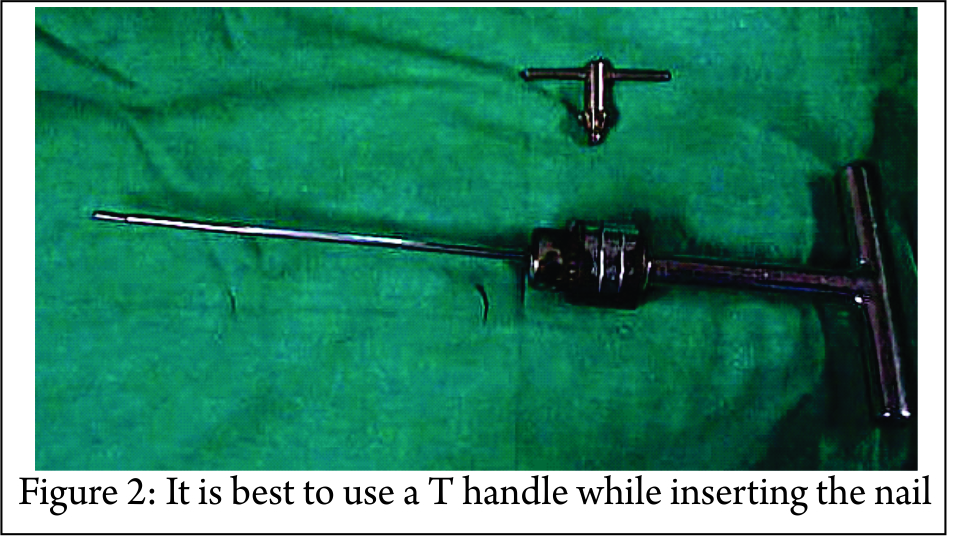
Screw elastic intramedullary nail is available in diameter of 2, 2.5, and 3 mm. The nails are 5-6 cm in length , with screw portion of 10mm length and 4.5mm in diameter. The screw head is of 3.5 mm size where the appropriate screw driver fits (Fig. 1). The nail is made of either steel of titanium and is sufficiently elastic to bend as it traversed the canal from the point of insertion and resilient enough to spring back in the curvature when finally seated. However it is still rigid enough to withstand the torsional, rotational, and angulatory forces.]Nail has a bevelled tip at one end and a threaded head positioned at other. This design allows the self-cutting thread to be advanced and screwed in with a 3.5 mm screw driver. The distal beveled end of the nail aids in fracture reduction and helps in engaging in the subchondral area of the bone, thereby imparting stability. The inserter should firmly grasp the nail in order to control rotation, insertion and nail withdrawal. It is best to mount the nail on a T handle while inserting but other devices can also be used (Fig. 2)
Surgical Technique:
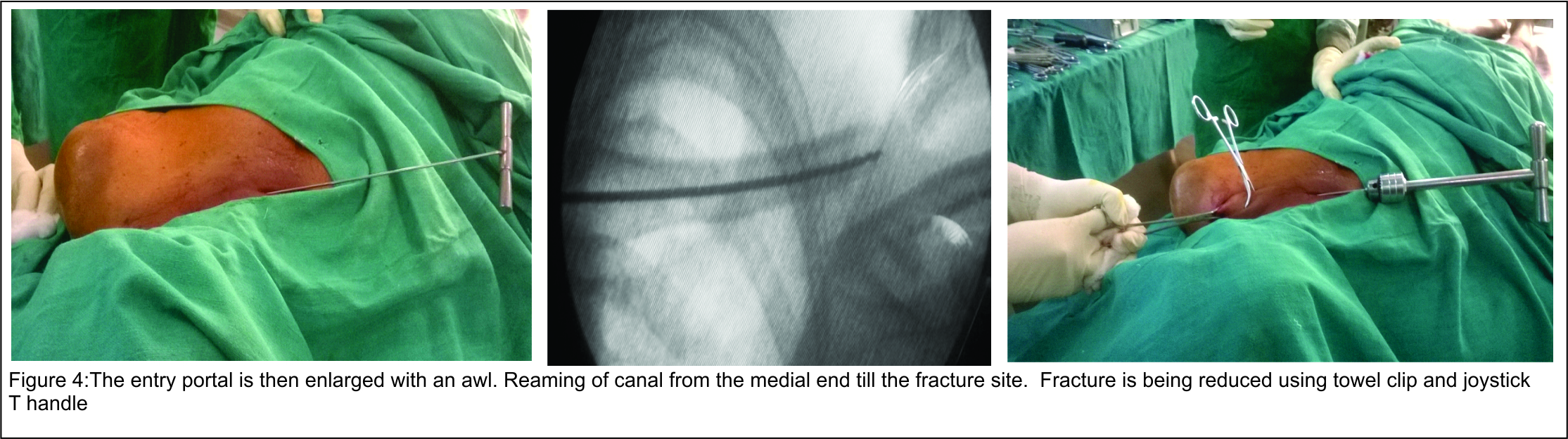
Operative procedure is carried out under interscalanae block or general anaesthesia. Affected shoulder is elevated by a bolster so that clavicle becomes more prominent. This position also helps to restore length and increase exposure of the clavicle (Fig. 3). The procedure is performed under fluoroscopic guidance. A one centimeter skin incision is made over medial end of clavicle and a hole is drilled in the anterior cortex with a 3.2 mm drill bit and guide. The insertion point is made approximately 1 cm lateral to the sternoclavicular joint. The entry portal is then enlarged with an awl (Fig.3).

The reaming of canal is done with sequential reamer and then an elastic nail of appropriate diameter and length is inserted in the medullary canal of clavicle with a universal chuck and T-handle (Fig. 4).
With oscillating movements the nail is advanced until it reaches the fracture site. With the help of percutaneously placed towel clips fracture fragments are approximated (Fig. 5). The reduction is checked in image-intensifier and then the nail is advanced through the fracture site till it reaches distal end of clavicle. Generally nail can be negotiated one cm short of acromioclavicular joint. If closed reduction is unsuccessful, an additional skin incision is made at fracture site for open reduction of the fragments (Fig. 5).
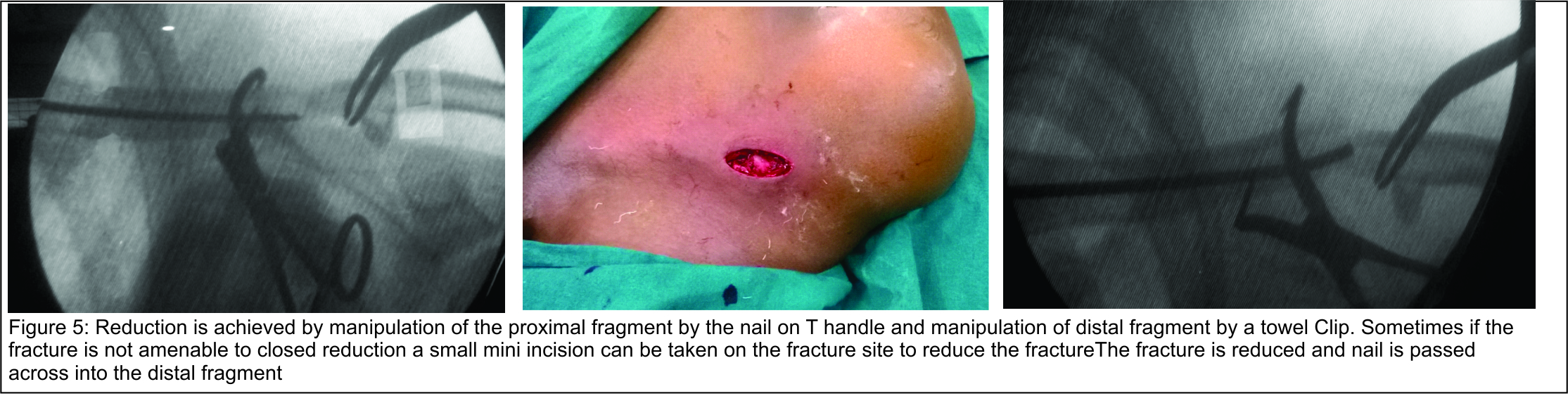
Although clavicle is S shaped, tip of the nail is curved which helps the surgeon to pass the elastic nail into distal fragment. After adequate engagement of the distal fragment, the medial end of screw nail is screwed in the metaphyseal region of the medial end of clavicle and skin closed over it (Fig. 6).

Postoperatively arm pouch sling is given for three weeks. Gentle pendulum exercises of the shoulder are allowed as per pain tolerance immediately after surgery. We tend to limit extreme overhead activities for 3-6 weeks. At four to six weeks, active assisted range of motion in all planes was allowed. When fracture union (defined as radiographic union with no pain or motion with manual stressing of the fracture) was evident, muscle strengthening exercises were also allowed. At eight to twelve weeks, Isometric and isotonic exercises were prescribed for shoulder girdle muscles with return to full activities (including sports) at three months (Fig. 7).

Conclusions
Percutaneous elastic screw intramedullary nailing of the clavicle is a safe, reliable method for fixation of displaced midshaft clavicle fractures. It is less invasive and allows rapid healing by callus formation. Complication rates are low, with better functional and cosmetic results.
| How to Cite this article: Gadegone W, Lokhande V, Salphale Y. The Screw Intra-medullary Elastic Nail Fixation in fresh Displaced Mid Shaft Clavicle Fractures – Technical note. Trauma International May – Aug 2016;2(2):53-55. |
