
Classifications of Intertrochanteric fractures and their Clinical Importance
Vol 1 | Issue 1 | July – Sep 2015 | page: 7-11 | Dhiraj V Sonawane[1].
Author: Dhiraj V Sonawane[1].
[1] Grant Medical College and Sir JJ Group of Hospitals, Mumbai. India.
Address of Correspondence
Dr. Dhiraj V. Sonawane
Asst. Prof. Grant Medical College and Sir JJ Group of Hospitals, Mumbai.
Email: dvsortho@gmail.com
Abstract
Intertrochanteric fractures are one of the most common fractures encountered by an orthopaedic Surgeon. Many attempts to classify these fractures are made and different scientific rationale are applied by various authors. Here we tried to provide an overview of both old and new classification of intertrochanteric fractures and also provide with the clinical significance of the same
Keywords: intertrochanteric fractures, hip fractures, classifications
Introduction
Intertrochanteric (IT) fractures are most common fractures seen in elderly osteoporotic, usually due to simple fall in the house. With increasing number of elderly patients its number is estimated to be double by 2040 [1]. Understanding important factors in management of IT fracture like stability, reduction, role of posteriomedial wall, lateral wall, will help in choosing implant for better outcome. Most classifications are based on these factors and help in selecting management protocols. Many classification systems have come from last 6 decades, but none of them are found to be unanimously acceptable worldwide. Few classifications have focussed on stability and anatomical pattern (Evans; Ramadier; Decoulx; & Lavarde) while others on maintaining reduction of various types (Jensen’s modification of Evan’s, Ender; Tronzo, AO).
An ideal classification should be simple, reproducible, easy to apply and should provide information on stability after reduction, secondary displacement, technique of fixation, postoperative mobilisation, outcome, and also data organisation for research. It should have good interrater and intrarater reliability and validity.
Classification Review:
Various classifications in Intertrochanteric fractures:
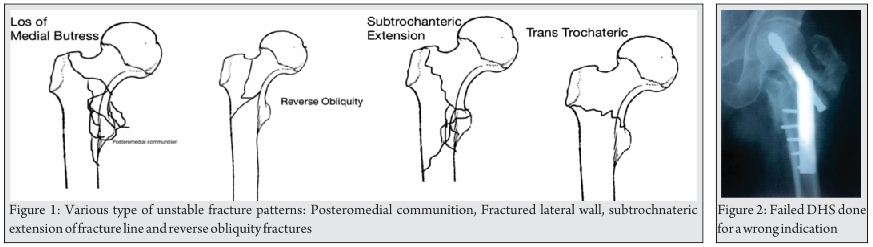
Evans Classification [2] (Fig 1):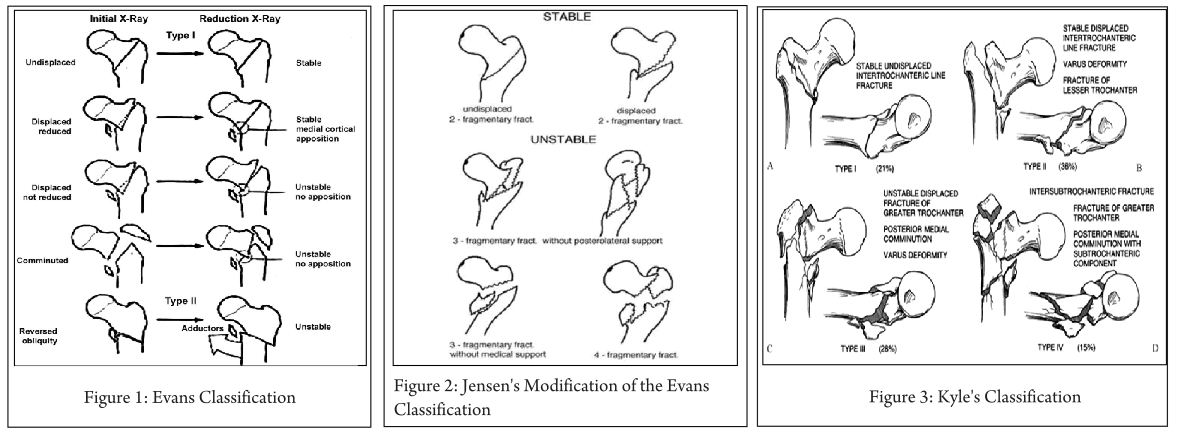
In 1949, Evans published his classification on intertrochanteric (IT) fractures as follows:
Type I:
Stable:
-Undisplaced fractures.
-Displaced but after reduction overlap of the medial cortical buttress make the fracture stable.
Unstable:
-Displaced and the medial cortical buttress is not restored by reduction of fracture.
-Displaced and comminuted fractures in which the medial cortical buttress is not restored by reduction of the fracture.
Type II: Reverse obliquity fractures.
Clinical importance: This helped in better understanding of intertrochanteric fractures based on stability of fracture after close reduction and skeletal traction. According to Evans, posterior-medial cortex continuation is important for restoring stability of IT fractures. Based on this he classified IT fractures into Stable and Unstable fractures. Stable fractures have intact or minimally communited posteriomedial cortex, while Unstable fracture has greater communition of posteriomedial cortex. Unstable fractures after reduction can be converted to stable fracture if the posteriomedial cortex opposition can be achieved. Reverse oblique pattern was considered inheritably unstable fracture as distal femur has tendency to drift medially due adductor pull.
Jensen’s Modification of the Evans Classification [3] (Fig. 2):
Jansen (1975 ) later modified Evans classification into three groups.
Displaced or undisplaced stable 2-fragment fractures, Unstable 3-fragment fractures with greater or lesser trochanter fracture and 4-fragment fractures
Clinical Importance: the classification reduced the number of types from 6 to 5 by including the extremely rare fracture with a reversed oblique fracture line and large greater trochanter fragment into Type 3. Modification of the Evans system offers the best prediction of the possibility of obtaining reliable anatomical reduction and the risk of secondary fracture dislocation.
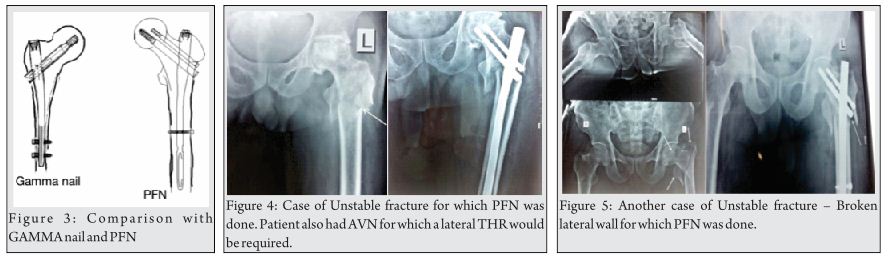
Kyle’s Classification [4] (Fig. 3):
Type I fractures consist of nondisplaced stable intertrochanteric fractures without comminution.
Type II fractures represent stable, minimally comminuted but displaced fractures; these are the fractures that, once reduced, allow a stable construct. Stable fractures are not a problem and hold up well with any type of fixation device.
Type III intertrochanteric fracture is a problem fracture and has a large posteromedial comminuted area.
Type IV fracture is uncommon and consists of an intertrochanteric fracture with a subtrochanteric component. This is the most difficult type of fracture to fix because of the great forces imposed by muscle forces and weight bearing on the subtrochanteric region of the femur.
Clinical Importance: Addition of new variant (type 4) extension of intertrochanteric fracture in neck.
AO/ Orthopaedic Trauma Association (OTA) Alphanumeric Classification [5] (1980-1987) (Fig. 4):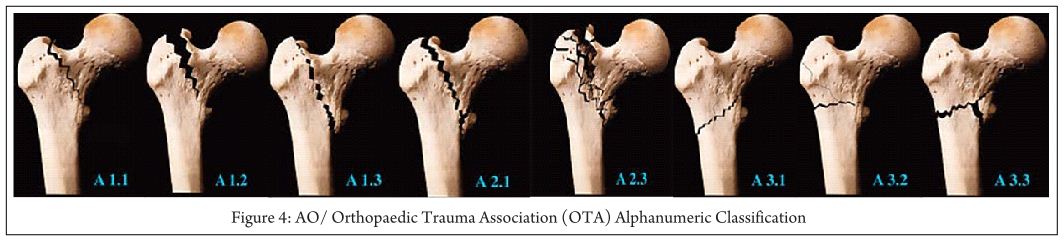
In the Comprehensive Classification of Fractures of the Long Bones, Müller and colleagues coded proximal hip fractures to offer a uniform alphanumeric fracture classification. This system was advocated by the AO/ASIF, and later adopted by OTA in their Fracture Compendium.
According to AO/OTA alphanumeric classification intertrochanteric fractures (Type 31A) Bone = femur = 3,Segment = proximal = 1,Type = A1, A2, A3 A1: simple (two-part) fractures, with the typical oblique fracture line extending from the greater trochanter to the medial cortex; the lateral cortex of the greater trochanter remains intact.
A2: fractures are comminuted with a posteromedial fragment; the lateral cortex of the greater trochanter, however, remains intact. Fractures in this group are generally unstable, depending on the size of the medial fragment
A3: fractures are those in which the fracture line extends across both the medial and lateral cortices; this group includes the reverse obliquity pattern or subtrochanteric extensions.
31-A Femur, proximal trochanteric
31-A1 Peritrochanteric simple
31-A1.1 Along intertrochanteric line
31-A1.2 Through greater trochanter
31-A1.3 Below lesser trochanter
31-A2 Peritrochanteric multifragmentary
31-A2.1 With one intermediate fragment
31-A2.2 With several intermediate fragments
31-A2.3 Extending more than 1 cm below lesser trochanter
31-A3 Intertrochanteric
31-A3.1 Simple oblique
31-A3.2 Simple transverse
31-A3.3 Multifragmentary.
Clinical importance: This helps in predicting prognosis and suggests treatment for the entire spectrum of IT fractures. Fractures A1.1 through A2.1 are commonly described as stable, and fractures A2.2 through A3.3 usually are unstable.
Generally, the Evans-Jensen type I fracture is represented by the 31-A1 group. Evans-Jensen type II fractures are in the 31-A2 group. The so-called reverse obliquity intertrochanteric fracture is in group 31-A3. It’s alphanumeric and standardized format make this system useful, particularly for research and documentation.
Boyd and Griffin Classification (1949) [6] (Fig. 5): 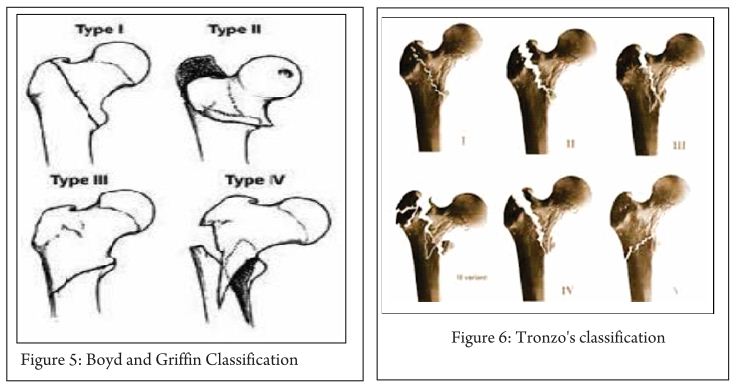
They were first to mention instability in both coronal and sagittal plane. This classification, included fractures from the extracapsular part of the neck to a point 5 cm distal to the lesser trochanter.
Type 1: Fractures that extend along the intertrochanteric line.
Type 2: Comminuted fractures with the main fracture line along the intertrochanteric line but with multiple secondary fracture lines (may be in coronal plane).
Type 3: Fractures that extend to or are distal to the lesser trochanter.
Type 4: Fractures of the trochanteric region and proximal shaft with fractures in at least two planes.
Clinical importance:
Type 1- Reduction usually is simple and is maintained with little difficulty. Results generally are satisfactory
Type 2- Reduction of these fractures is more difficult because the comminution can vary from slight to extreme
Type 3- these fractures usually are more difficult to reduce and result in more complications at operation and during convalescence.
Type 4- if open reduction and internal fixation are used, two-plane fixation is required because of the spiral, oblique, or butterfly fracture of the shaft.
Tronzo’s classification [7] (1973) (Fig. 6):
Tronzo incorporated Boyds and Griffin two plane instability in classification.
Type 1: Incomplete fractures
Type 2: Uncomminuted fractures, with or without displacement; both trochanters fractured
Type 3: Comminuted fractures, large lesser trochanter fragment; posterior wall exploded; neck beak impacted in shaft
Type 3 Variant: As above, plus greater trochanter fractured off and separated
Type 4: Posterior wall exploded, neck spike displaced outside shaft
Type 5: reverse obliquity fracture, with or without greater trochanter separation
Clinical importance:
This system is complex to use & not adequate to apply in clinical practice. It has poor reliability, though can be used for documentation of long-term results and comparison of treatment modality. Yet many surgeons prefer it for its simplicity and biomechanical rationale.
The Ramadier’s Classification[8](Fig. 7):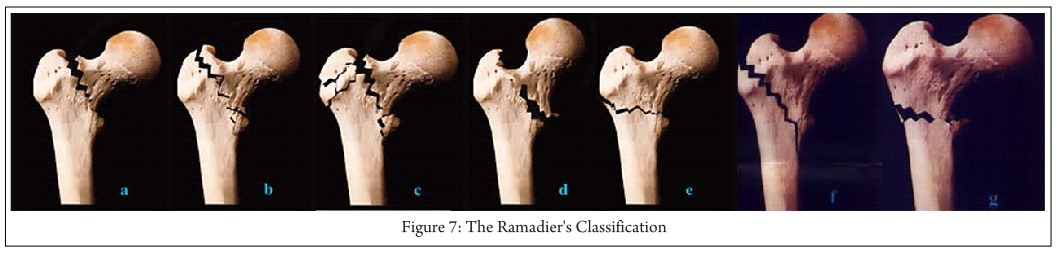
A: Cervico-trochanteric fractures- with a fracture line at the base of the femoral neck
b: Simple pertrochanteric fractures- fracture line that runs parallel to the intertrochanteric line; frequently, the lesser trochanter is broken off
c: Complex pertrochanteric fractures have an additional fracture line that separates most of the greater trochanter from the femoral shaft; the lesser trochanter is often fractured
d: Pertrochanteric fractures with valgus displacement- fracture line that begins on the greater trochanter and finishes below the lesser trochante
e: Pertrochanteric fractures with an intertrochanteric fracture line
f: Trochantero-diaphyseal fractures- spiral line through the greater trochanter and into the proximal shaft often with 3rd fragment.
G: Subtrochanteric fractures- more or less horizontal fracture line that runs below the two trochanters
Decoulx and Lavarde’s classification [9](1969):Simple anatomical classification for descriptive purposes.
Cervico-trochanteric fractures
Pertrochanteric fractures
Intertrochanteric fractures
Subtrochanteric fractures
Subtrochantero-diaphyseal fractures
The Briot Classification Diaphyseo-Trochanteric Fractures [10] (1980) (Fig. 8):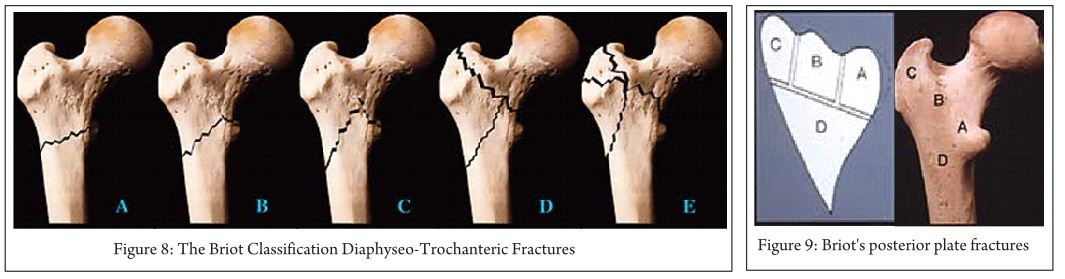
A Evans’ reversed obliquity fracture
B “Basque roof” fractures
C Boyd’s “steeple” fracture
D Fractures with an additional fracture line ascending to the intertrochanteric line
E Fractures with additional fracture lines radiating through the greater trochanter
Briot’s posterior plate fractures
Note: Boundaries of posterior plate, Maximum extent of plate, Possible fracture lines
Clinical importance: Its simple and based on biomechanical concept. Briot’s found posterior wall fracture is important for sagittal instability and external rotation sometimes causing malunion in external rotation. Reduction can be done in these by internal rotation reducing the anterior gap while realign the posterior fractured wall.
Ender Classification(1970)[11] (Fig. 10):
Trochanteric eversion fractures
-1. Simple fractures
-2. Fractures with a posterior fragment
-3 Fractures with lateral and proximal displacement
3. trochanteric inversion fractures
-4. With a pointed proximal fragment spike
-5 .With a rounded proximal fragment beak
6. Intertrochanteric fractures
Subtrochanteric fractures
-7 and 7a Transverse or reversed obliquity fractures
-8 and 8a Spiral fractures
Clinical importance: This classification gives information on injury mechanism, which can be helpful to reduce fracture while performing closed nailing.
Dr G. S. Kulkarni et al Classification / Modified Jenson-Evan’s Classification[1] (Fig 11): 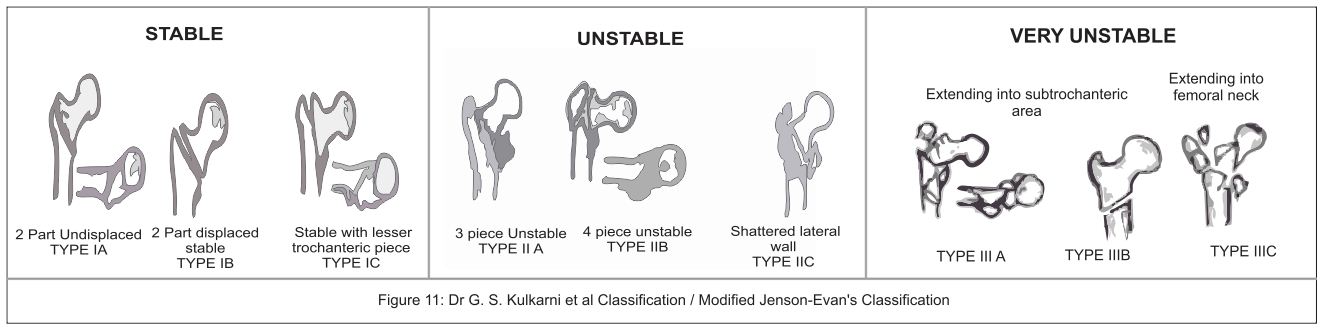
Dr G.S. Kulkarni et al [1] published his new classification in intertrochanteric fractures based on AO & Evan-Jansen classification. He added new varieties of intertrochanteric fractures described by Gotfried[12] and Kyle [4]. This classification is treatment oriented and will help in deciding the implant according to the fracture type.
Type IA- stable undisplaced.
Type IB- stable minimally displaced.
Type IC- stable minimally displaced with a small fragment of lesser trochanter.
Type IIA- unstable 3 piece fracture with large posteromedial fragment of lesser trochanter.
Type IIB- 4 piece fracture.
Type C- Shattered lateral wall.
Type IIIA- trochanteric fracture with extension into subtrochanter.
Type IIIB- reserve oblique.
Type IIIC- trochanteric fracture with extension into femoral neck area.
Clinical Importance: Classification helps in selecting treatment protocols as below.
Type I: This stable fractures can be managed by any fixation modality gives excellent results. DHS is implant of choice.
Type II: These unstable fractures are described as problem fractures can be managed with DHS with some modification or IMN.
Type III: This very unstable fracture with DHS gives poor results. In these type with lateral wall fracture use of DHS lead to excessive collapse, pain, restricted mobility in hip, sometime non union and failure. Intramedullary nails (IMN) are better choice as they prevents excessive collapse at fracture site, better restoration of anatomy and biomechanically stronger implants; Arthroplasty can also be done in select cases. Unusual fracture pattern like basi-cervical fractures extension can be fixed with additional derotation screw as these are also rotationally unstable. Reverse oblique pattern like fracture lateral wall are better fixed with IMN.
Conclusion:
Various classifications have been proposed over years described the fracture patterns, focusing on importance of posteriomedial and lateral wall for stability. Tronzo classification is found to be less reliable and not useful in clinical practice. AO/OTA and Dr G.S. Kulkarni et al modified classification has described in detail the preferred implant according to the fracture type. An AO/OTA group has good reliability but subgroup assessment has poor reliability; it is more useful in record keeping, deciding management and research. Kulkarni et al classification is found to be more simple & easy to apply in practice, record keeping and research. There is still no consensus on the best classification but with new biomechanical informations coming through, the classification systems would continue to evolve.
References
1. GS Kulkarni, Rajiv Limaye, Milind Kulkarni, Sunil Kulkarni. Current Concept review: Intertrochanteric fractures. Indian Journal of Orthopaedics.2006;40:16-23.
2. Evans, E. M. () The treatment of trochanteric fractures of the femur. J. Bone Jt Surg. 1949;31-B: 190-203.
3. Jensen J. S. Classification of trochanteric fractures. Actaorthop. Scand. 1980; 51:803-810.
4. Kyle R. F., Gustilo R. B. And Premer R. F. Analysis of six hundred and twenty-two intertrochantenc hip fractures. J. Bone joint(Am). 1979;61: 216-21.
5. M.E. Muller, S. Nazarian, P. Koch, J. Schatzker The comprehensive classification of fractures of long bones Springer, Berlin. 1990.
6. Boyd HB, Griffin LL. Classification and treatment of trochanteric fractures. Arch Surg. 1949; 58:853.
7. Tronzo RG. Symposium on fractures of the hip. Special considerations in management. Orthop Clin North Am. 1974; 5(3): 571–583.
8. M. Bombart, J.O. Ramadier Trochanteric fractures Rev Chir Orthop, 52 (1966), 353–374.
9. Decoulx P, Lavarde G. Fractures of the trochanteric region. A statistical study of 2,612 cases. J Chir (Paris). 1969; 98(1):75-100.
10. Briot B. Fractures per-trochantériennes: anatomie pathologique et classification. Cahiers d’Enseignement de la SOFCOT Expansions Sci Franc.1980;12: 69-76.
11. J. Ender Per- und subtrochantere Oberschenkelbrüche. Hefte Unfallheilk;1970:106, 2–11.
12. Gotfried Y. The lateral trochanteric wall. Clin Orthop. 2004; 425:.82-86.
| How to Cite this article: Sonawane DV. Classifications of Intertrochanteric fractures and their Clinical Importance. Trauma International July-Sep 2015;1(1):7-11 |
{kind=link}