LICENSE
![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X

![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X
History of Pelvi-Acetabular Fracture Treatment
/in Volume 2 | Issue 2 | May-Aug 2016Vol 2 | Issue 2 | May – Aug 2016 | page:17-19 | A S Prasad, Rahul Rishi
Author: A S Prasad [1], Rahul Rishi [1]
[1] Chandak Nursing Home Nagpur Maharashtra India.
Address of Correspondence
Dr. A S Prasad
Postal Address of correspondence with email of corresponding author-7/187 C ,Swaroop Nagar, Kanpur-208002.
E-mail: drprasadas@gmail.com
Abstract
Acetabular Fractures were treated conservatively before 1960. Robert Judet in 1960 started to treat displaced Acetabular Fractures Surgically. In the modern world of fast moving vehicular traffic, the Pelvic Fractures are the third most common cause of death in Motor Vehicle accidents. The associated injuries to the abdomen, chest, CNS and long bones as well as hemodynamic instability is frequently present Implementation of the ATLS protocol has helped in the early management of such patients but even during the ”golden hour” further decisions need to be taken regarding the surgical management (temporary or definitive) in order to improve survival rates in such patients. Acetabular Fixation can be delayed for a week after the index injury managing the life threatening injuries first. However they may have to be fixed as a damage control orthopedics when the Hemorrhage of pelvis fracture itself is a cause of the shock.
Keywords: Acetabulum Fractures, Pelvis Fracture, treatment.
Introduction
Today the Pelvic Fractures are the Third most common cause of death in Motor Vehicle accidents. The concern is to reduce this and guidelines for the management have come for the same. Historically too this has been discussed a lot. The modern specialty was really born with the publication of Malgaigne’s books on fractures and subluxations in 1847[2] . At the same time in the United Kingdom, Sir Astley Cooper (1768–1841) described various pelvic fractures, making the distinction between marginal stable fractures and unstable pelvic ring injuries. At this stage it should be emphasized that all these observations were made onclinical grounds with no x-rays. In the late 1950s and 1960s, Robert Judetbegan attempting to treat displaced acetabular fractures surgically.He felt that the outcomes with displaced acetabular fractures following conservative treatment were unacceptable. He identified certain subsets of acetabular fractures thatdid not do well with conservative treatment. These included fractures that involved the tectum or roof and those fractures where the hip was unstable. He described ten classic fractures patterns (five basic and five complex). Judet also developed many surgical approaches, particularly the ilio-inguinal approach, for treatment of anterior acetabular injuries. The present day concept of fixation after appropriate reduction started with Judet. He emphasized that for pelvic fractures treated non-operatively functional outcome was frequently a problem for both patient and surgeon as deformities and chronic pain had a significant incidence.
Present Day Concepts
In the modern world with a fast moving life, the acetabular fractures are mostly a part of Poly Trauma. Prioritizing the steps of management is an issue to get the best for the injured. The associated injuries to the abdomen, chest, CNS and long bones as well as hemodynamic instability is frequently present Implementation of the ATLS protocol has helped in the early management of such patients but even during the ”golden hour” further decisions need to be taken regarding the surgical management (temporary or definitive) in order to improve survival rates in such patients[1]. Haemodynamic stabilization is of capital importance in unstable and ”in extremis” patients. Hemorrhagic shock is one of the four pathological cascades of polytrauma (shock, hypothermia, coagulopathy, soft tissue injury)[3].Focus is given on the identification of the source of bleeding (fracture site, thoracic, abdominal or pelvic organ injuries, wounds and arteriovenous disruptions). Blunt abdominal trauma, open fractures and wounds should be addressed promptly. Normo-voluemia can then be restored primarily by administration of crystalloids/colloids and blood products.
Damage Control Orthopedics in Fracture Acetabulum
In some patients who are both hemodynamically and mechanically unstable, and in whom the major bleeding is thought to be related to the pelvic fracture, external stabilization of the pelvis becomes the first priority. Because the main sources of bleeding are most frequently the presacral venous plexus and fractured bony surfaces. External stabilization decreases the hemorrhage by reducing the volume of the pelvic basin and approximating the fracture ends.
Pelvic binders
Circumferential pelvic binders or sheets are gradually replacing anterior external fixation (AEF) as the method of choice of immediate external stabilization, and currently form part of the ATLS protocol[4]. These binders are noninvasive, simple to apply, inexpensive and can be applied at a prehospital stage.
It has been shown that simple application of this sling increases pelvic stability by 61% in response to rotational stress and 55%, flexion–extension. Although the same study[5] found this method to be less rigid than AEF, it has nonetheless been shown to reduce unstable pelvic fractures radiologically and to improve patient’s hemodynamic status[6].
Clinical judgment and reassessment are important in using these techniques. This safe, noninvasive method seems to be a logical first resuscitative step with a serious pelvic fracture, to provide early hemorrhage control before considering invasive methods
Anterior external fixation
Immediate AEF of an unstable pelvic injury has been the mainstay of acute stabilization for the past few decades. Reimer and coworkers[7] reduced mortality rates from 22% to 8% by adding acute AEF to their hospital resuscitation protocol. Based on their results, they concluded that skeletal stabilization of pelvic injury should be viewed as a part of resuscitation rather than reconstruction. Burgess and colleagues[18] and others[9,10] have also documented decreased transfusion needs and reduced mortality with the use of anterior external fixator. Subsequent investigators [8,9,11,14] have also recommended immediate application of external fixation for hemodynamically unstable patients, and consider it a life-saving procedure. Some investigators have advised[9] prophylactic stabilization with anterior external fixator in all patients demonstrating bony instability, as even those patients who are initially hemodynamically stable on presentation may decompensate later. The anterior fixator is thought to contribute to hemostasis by maintaining a reduced pelvic volume, allowing tamponade, and by decreasing bony motion at the fracture site, allowing clots to stabilize[15]. C– clamps. To deal with posteriorly unstable fractures, Ganz and coauthors[16] developed a pelvic C-clamp, now available in most trauma units. It acts like a simple carpenter’s clamp and can exert transverse compression directly across the sacroiliac joint. Experimental data[16] have shown that an average compression force of 342 N can be applied to the area of this joint. These clamps have been used therapeutically in hemodynamically unstable patients, and prophylactically in stable patients with unstable pelvic- ring disruptions. Hemodynamic status and fracture reduction have been shown to improve in both groups[16].
Acute fracture fixation
Provisional fixation of unstable pelvic- ring disruptions with a pelvic clamp or an external frame with a supracondylar pin has proved markedly beneficial in the resuscitative phase of management. If the patient is too ill to allow a more invasive intervention, traction pins can remain in place with the external frame as definitive treatment. If, however, the patient undergoes a laparotomy to deal with visceral injuries, symphyseal disruption and medial ramus fractures should be plated at the same time. Because neither blood loss nor operative time is greatly increased, combining these repairs decreases the risk of complications in a patient who is already compromised[17].
Pelvic packing
Patients who remain unstable with a probable retroperitoneal cause in spite of aggressive resuscitative efforts should not be transported to a distant angiography suite, especially if delay is involved[18]. These are often patients at risk for abdominal compartment syndrome, and who therefore need an open peritoneal cavity for adequate cardiovascular physiologic support after surgery. Such patients undergoing laparotomy for an identifiable intraperitoneal cause of hemorrhage should be assessed for an expanding pelvic hematoma. The true pelvis should be packed at that time if the hematoma has ruptured; the pelvic hematoma is otherwise not opened routinely. The true pelvis should be packed with large abdominal swabs and the wound closed over the packs to create tamponade. The packs are removed or changed in a second procedure at 24–48 hours.
Open fractures
Potentially lethal injuries with a reported mortality rate of 30%–50%[19]. Open fractures of the pelvis by definition communicate with the rectum, the vagina, or the outside environment by disruption of the skin. They are often associated with disruption of the pelvic floor, leading to loss of tamponade and persistent bleeding. Clinical suspicion of an open fracture and any rectal or vaginal bleeding mandate a thorough examination, proctoscopic, sigmoidoscopic or by speculum.
These are the cases for application of Damage Control Orthopedics Principles.
Definitive Fixation
Since the birth of pelvic fracture surgery, timing of surgery has been referred to as either early or late. Unfortunately, the terminology of ”early/late fixation” has been used inconsistently. Some of them define as ”early” the first 8 h[20],24 h[21],72 h[22],first week[23] or even the first 14 days[22] or 21 days[24] post-injury and the term ”late” has been used for periods above 2 weeks post-injury[25] or as long as 3 months post-injury[26]. Definitive fixation in 1st week is advisable, however can be extended to 14 days is the majority opinion now.
Delayed Fixation
Even though the studies favoring Early Total Care became the golden rule in trauma surgery, there was still much controversy. Patients were operated between the 5th and 14th day based on the assumption that earlier operation would be associated with significant and possibly life- threatening hemorrhage[27] and hemodynamically unstable patients were generally considered to be too unstable to undergo even external fixation[28].In real life, delayed fixation can be due to medical complications, unstable patients unable to operate on or transfer to a specializedCentre, unavailable senior surgeon, unavailable operating staff and operating rooms.Delayed fracture fixation creates operative difficulties: scar tissue, callus formation, inability toobtain anatomic reduction and need for more extensile approaches. Mears et al. found thatdelayed surgery of more than 11 days was related tosignificantly fewer anatomical reductions[29]. Alsothe quality of reduction is strongly related to theage of the patient, the above 70 year-old havingpoorer reductions and more intra-articular damage[29].
Conclusion
Fractures around hip joint are one of the most common and debilitating entities requiring intervention . These fractures encompass fractures of the pelvis and acetabulum. Health care providers must be trained and educated with scope of this problem as well as the basic types of these fractures and treatment they warrant. The clear distinction between energy levels of the injuries leading to these fractures should be understood and treatment given accordingly. This article briefly amalgamates these issues and gives pictorial examples to illustrate the specific points.
References
1. Katsoulis E, Pape HC, Giannoudis PV. Shock-room management of pelvic ring lesions. Eur J Trauma 2005;31(3):222— 30.
2. Malgaigne JF (1847) Traite des fractures et des luxations,2 volumes.
3. Pohlemann T, Bosch U, Gansslen A, Tscherne H. The Hann- over experience in management of pelvic fractures. Clin Orthop Relat Res 1994;(305):69—80.
4. American College of Surgeons. Advanced Trauma Life Support for Doctors. Instruc- tor Course Manual. Chicago (IL): the College; 1997. p. 206-9.
5. Bottlang M, Krieg JC, Mohr M, Simpson TS, Madey SM. Emergent management of pelvic ring fractures with use of circum- ferencial compression. J Bone Joint Surg Am 2002;84(Suppl 2):43-7.
6. Simpson T, Krieg JC, Heuer F, Bottlang M. Stabilization of pelvic ring disruptions with a circumferencial sheet. J Trauma 2002;52:158-61.
7. Reimer BL, Butterfield SL, Diamond DL, Young JC, Raves JJ, Cottington E, et al. Acute mortality associated with in- juries to the pelvic ring: the role of early patient mobilization and external fixa- tion. J Trauma 1993;35:671-7.
8. Burgess AR, Eastridge BJ, Young JW, El- lison TS, Ellison PS Jr, Poka A, et al. Pelvic ring disruptions: effective classifica- tion system and treatment protocols. J Trauma 1990;30:845-56.
9. Poka A, Libby E. Indications and tech- niques for external fixation of the pelvis. Clin orthop 1996;(329):54-9.
10. Gylling SF, Ward RE, Holcroft JW, Bray TJ, Chapman MW. Immediate external fixation of unstable pelvic fractures. Am J Surg 1985;150(6):721-4.
11. Kellam JF. The role of external fixation in pelvic disruptions. Clin Orthop 1989; (241):66-82.
12. Slatis P, Karaharju EO. External fixation of unstable pelvic fractures: experience in 22 patients treated with trapezoid com- pression frame. Clin Orthop 1980;(151): 73-80.
13. Trafton PG. Pelvic ring injuries. Surg Clin North Am 1990;70:655-69.
14. Wild JJ Jr, Hansen JW, Tullos HS. Un- stable fractures of the pelvis treated by ex- ternal fixation. J Bone Joint Surg Am 1982;64:1010-20.
15. Mears DC. Clinical techniques in the pel- vis. In: Mears DC, editor. External skele- tal fixation. Baltimore (MD): Williams and Wilkins; 1983. p. 342.
16. Ganz R, Krushell AJ, Jakob RP, Kuffer J. The antishock pelvic clamp. Clin Orthop 1991;(267):71-8.
17. Tile M. Acute pelvic fractures: II. Princi- ples of management. J Am Acad Orthop Surg 1996;4(3):152-61.
18. Gansslen A, Giannoudis P, Pape HC. Hemorrhage in pelvic fractures: Who needs angiography? Curr Opin Crit Care 2003;9:515-23.
19. Jones AL, Powell JN, Kellam JF, McCor- mack RG, Dust W, Wimmer P. Open pel- vic fractures: a multicenter retrospective analysis. Orthop Clin North Am 1997;28 (3):345-50.
20. Latenser BA, Gentilello LM, Tarver AA, et al. Improved outcome with early fixation of skeletally unstable pelvic fractures. J Trauma 1991;31(1):28—31.
21. Plaisier BR, Meldon SW, Super DM, Malangoni MA. Improved outcome after early fixation of acetabular fractures. Injury 2000;31(2):81—4.
22. Cole JD, Bolhofner BR. Acetabular fracture fixation via a modified Stoppa limited intrapelvic approach. Description of operative technique and preliminary treatment results. Clin Orthop Relat Res 1994;(305):112—23.
23. Browner BD, Cole JD, Graham JM, et al. Delayed posterior internal fixation of unstable pelvic fractures. J Trauma 1987;27(9):998—1006.
24. Matta JM, Tornetta III P. Internal fixation of unstable pelvic ring injuries. Clin Orthop Relat Res 1996;(329):129—40.
25. BruetonRN.Areviewof40acetabularfractures:theimpor- tance of early surgery. Injury 1993;24(3):171—4.
26. Johnson EE, Matta JM, Mast JW, Letournel E. Delayed reconstruction of acetabular fractures 21—120 days follow- ing injury. Clin Orthop Relat Res 1994;(305):20—30.
27. Goldstein A, Phillips T, Sclafani SJ, et al. Early open reduc- tion and internal fixation of the disrupted pelvic ring. J Trauma 1986;26(4):325—33.
28. Riemer BL, Butterfield SL, Diamond DL, et al. Acute mor- tality associated with injuries to the pelvic ring: the role of early patient mobilization and external fixation. J Trauma 1993;35(5):671—5.
29. Mears DC, Velyvis JH, Chang CP. Displaced acetabular frac- tures managed operatively: indicators of outcome. Clin Orthop Relat Res 2003;(407):173—86.
(Abstract) (Full Text HTML) (Download PDF)
Symposium on Pelviacetabular Fractures
/in Volume 2 | Issue 2 | May-Aug 2016Vol 2 | Issue 2 | May – Aug 2016 | page: 3 | Dr. Harish Makker
Author: Harish Makker [1]
[1] Consultant Orthopaedic Surgeon, Lucknow, India.
Address of Correspondence
Dr.Harish Makker.
Rajendra Nagar,opp.water Tank, Lucknow, India 226004 India.
Email: drharishmakkar@gmail.com
Symposium on Pelviacetabular Fractures
Dear Friends
I have been given the responsibility of editor of a Symposium issue of Trauma International on Pelvi- Acetabular Fractures.
The idea came so as to dedicate an issue of Trauma International to the -Cadaveric Pelvi Acetabular Fracture Fixation Workshop under C ARM -after creating fractures in a cadaver, which was done for the first time in the world in 2014 and again in 2015. I have tried to include all relevant topics in this symposium so as to make it a comprehensive presentation of diagnosis and management of pelvi -cetabular and sacral #s and its treatment. The symposium is planned to run in three issues of Trauma International. To my knowledge this is a budding field of Orthopaedics as not many surgeons are still comfortable approaching this deep and curved bone and in midlevel and big cities, very few percentage of surgeon attempt this surgery and so has a vast scope of teaching this branch of orthopaedics. To learn a complicated surgery, the methods are- Read from Text book, Attend conferences and workshops, Work under a surgeon who has a vast experience in handling such cases [it may not be necessary that you get such cases when you visit him] or attend such cadaveric workshops where life like atmosphere and fracture-created cadavers are present. Masters of the field are there to reduce and fix it and you get a chance to do the same under their guidance. I had this idea for last few years and with the help of my friends I could achieve this and did the world`s first pelvi -acetabular fracture fixation workshop in September 2014 .My Faculty were Dr. Ramesh Sen of PGI Chandigarh and Dr. Vivek Trikha of AIIMS Delhi and nearby faculty from Kanpur and Lucknow ,which paved the way for 2nd workshop in November 2015 and further an invite to be Editor of a Symposium Issue of Trauma International.
Hope this will make a small but significant approach to attract and invite young and not so young surgeons to attempt this branch of orthopaedics. More details will follow in the regular issue of the Journal.
Pictures from Cadaveric Pelvi Acetabular Fracture Fixation Workshop & CME: 2015
Register for 2016 course 19-20th November at Lucknow. Registration Details on Website of Trauma International
(Abstract) (Full Text HTML) (Download PDF)
Editorial – Academics and Orthopaedic Trauma
/in Volume 2 | Issue 2 | May-Aug 2016Vol 2 | Issue 2 | May – Aug 2016 | page:1-2 | Dr. Sunil G Kulkarni and Dr. Ashok K Shyam
Author: Sunil G Kulkarni [1], Ashok K Shyam [2,3]
[1] Post Graduate institute of Swasthiyog Pratisthan Miraj, India.
[2] Indian Orthopaedic Research Group, Thane, India.
[3] Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India.
Address of Correspondence
Dr. Ashok Shyam
IORG House, A-203, Manthan Apts, Shreesh, CHS, Hajuri Road, Thane, India. 400604.
Email: drashokshyam@yahoo.co.uk
Editorial: Academics and Orthopaedic Trauma
Trauma, specifically Orthopaedic Trauma is a focussed surgical field. There are two main learning areas in orthopaedic trauma; Decision making and Surgical skills. We believe all academics in trauma surgery have to be focussed on these two parameters rather than focussing more on the theoretical aspect of the subject. Of course we need to know the basic demography and the epidemiology of fractures and injuries, however they do not generally affect the care given by individual surgeons to their individual patients. Even at Traumacon our focus remains on these two points while structuring the whole program. Decision making in Orthopaedic trauma is one of the most important but difficult area to understand. We begin learning this process way back in our medical schools, however orthopaedic trauma is something that we continue to learn forever. Our decision making depends essentially on the knowledge and experience we gather from various sources. The knowledge that help us make optimal decision are largely gained from our personal experiences in treating similar cases, share experiences from our colleagues and seniors, speciality conferences like Traumacon and speciality Journals like Journal of Orthopaedic Trauma, Injury Journal and now Trauma International. Orthopaedic Trauma is one area where every fracture has its own personality which needs to be understood along with patients profile and demands. A straightforward guideline for every facture is not only unavailable but also not advisable. The art of decoding the personality of the fracture helps us balance between managements options and also reach an optimal plan which is suitable for that particular fracture in that particular patient. In our trauma meetings this should be the focus of our discussion and that is what everyone involved in trauma care is interested into. Journals are also trying to find new ways of doing this by improving the format of articles, including expert commentaries, inviting narrative reviews etc. Articles in journals also have to be read carefully with the aim of applying the knowledge to your patient and not extrapolating the patient to fit the knowledge given in the article. This is an important aspect in reading any journal article. Surgical skills is another area that goes hand in hand with decision making in providing the best possible result to the patient. Surgical skill include the surgical technique and steps and also include knowing about the intraoperative improvisations, complications and their managements. Conferences like Traumacon have a huge focus on the surgical technique part but also play an important role in informing the delegates about what not to do, how to avoid complications and if complications happen how to manage them. These four together form the complete surgical skill set which will help trauma surgeons master a surgery. This part is very difficult to learn by reading journals or books unless the journal formats are modified to include the practical aspects of the surgical skills. Randomised trials and meta-analysis will not be of much hep to us in learning a surgical skill. Trauma International has created two special section on the surgical skills; one on technical note and one on ‘How I do my surgery’. Both sections are mostly pictorial and also include videos of the surgical steps. These will again help the surgeons to know the variations in surgical techniques from different. There is much more that should be done and that can be done. Technology can help us disperse this knowledge much more effectively but again it should be used wisely and not as a panacea. The requirements of Academic Orthopaedic Trauma is much different than the conventional modes of medical teaching. Learning decision making requires a different approach which is a balance of practical experience along with evidence based medicine. Surgical skills can be learnt by following good surgical practices, learning by personal experience, learning from experts and using technology in an optimal way. In future there will definitely be a shift from theoretical approach to a more practical and patient oriented approach and in coming years this will help us provide better care to our patients. Trauma International focusses mainly on this academic requirement and we have dedicated symposia in every issue of the Journal. We thank Dr Harish Makker for taking initiative and compiling and editing the current symposia on Pelvi-acetabular fractures. The sysmposia has contributions from all across the country and is divided into three parts. Part 1 containing basic details of pelvi-acetabular fractures and principles of emergency and specific management is published in this issue. The next part will contain the surgical approaches and last part will have more specific articles dedicated to individual fracture types and technical aspect of pelvi-acetabular surgery. Trauma International is also now officially affiliated to Trauma Society of India and will be regularly featuring contributions from the society members and mentors. We are very excited about this association and are hopeful that it will ramify into excellent academic content that will feature in the journal.
If you have any further opinions about the ideas presented above, please write to us. With this we leave you to enjoy this issue of Trauma International.
(Abstract) (Full Text HTML) (Download PDF)
Recurrent Anterior Shoulder Dislocation: Boytchev Treatment
/in Volume 2 | Issue 2 | May-Aug 2016Vol 2 | Issue 2 | May – Aug 2016 | page:31-39 | Otman Benabdallah, Ahmed Khamlichi
Author: Otman Benabdallah [1], Ahmed Khamlichi [1]
[1] Centres hospitaliers de Tanger, Morocco
Address of Correspondence
Dr. Otman Benabdallah
Centres hospitaliers de Tanger, Morocco
Email: otman.benabdallah@hotmail.com
Abstract
Background: Utilized since 1951, the Boytchev procedure is an open anterior repair, performed for the treatment of anterior gleno-humeral instability, which involves rerouting the muscles that attach the coracoid process deep to the subscapularis muscle between this and the capsule. The tip of the coracoid with its muscles is reattached to its base in the anatomical position.
Method: We conducted a prospective study of twenty patients with recurrent shoulder dislocations who were treated by the Boytchev procedure. All are men, with an average age of 29.2 years (age range from 17 to 42 years). 14 patients were affected on the right shoulder, 6 on the left. All had a clinical history of recurrent dislocation . We also performed a search of all published articles in the literature (16),17 studies including our series, with the aim of estimating, via a statistical analysis, to shed light on the post-operative results of recurrent anterior dislocations of the shoulder, for determining the reliability of this technique and possible specific risk factors that might lead to recurrence.
Results: Evaluated using the Rowe score in our series, 19 patients had excellent and good results; one patient, who suffered a recurrence, had a poor result in terms of stability. Another patient developed osteoarthrosis. For the 17 studies, the number of patients is 477 with 485 dislocated shoulders. The rate of recurrence is 7.33% .In 12 studies, the rate is 2%, versus 21.08% in 5 studies with a significant difference (1-p=99.89%). Concerning the gradation of results, we have 441 excellent and good results and 44 fair and poor (91% versus 9% with p=>99.9% which is also very significant).
Conclusion: The Boytchev procedure exhibits low recurrence rates in compiled studies and so can be considered a reliable surgical technique.
Keywords: Shoulder recurrent dislocation, Boytchev treatment
Introduction
Shoulder instability is one of most controversial joint diseases in terms of diagnosis and treatment. Clinical, anatomo-pathological, radiological, surgical and cadaveric findings have improved the recognition of unstable shoulder lesions and allowed a better understanding of their etiology and possibly a more adequate treatment. One of the key points about anterior dislocations is that Bankart is not always the essential lesion; lab tests seem to show in fact that this lesion alone does not frequently lead to dislocation, and it coexists with many other possibilities: HAGL lesions, capsular rupture or capsular plastic deformation, glenoid fracture or bony erosion, large Hill Sachs lesions, and muscular insufficiency. Now it is accepted that shoulder stability depends equally on static and dynamic stability, even after Bankart or capsular shifts [1]. The standard treatment is surgical; more than 150 surgical techniques have been used, and all are compromised by their own rate of recurrences and complications (loss of range of motion, osteoarthrosis, infection, etc) [2].
In our practice, we generally use the Latarjet or Bankart procedures. In 2002, we introduced the Boytchev procedure as another optional open repair for recurrent anterior dislocations [3].
This technique has also given rise to recurrences and complications; we note in the literature that a majority of authors obtained excellent and good results (Conforty, Ha’eri, Chatterjee, Shibata Yozo…), while others results were merely fair (Dalsgaard, Zamora-Navas) [2, 4, 5, 6, 7, 8]. Recurrence rates vary between 0% and 44%, so the procedure seems to be controversial.
Between January 2002 and December 2012, we therefore conducted a prospective study of 20 patients treated by the Boytchev procedure, with a follow up extending until December 2014. Our purpose was to shed light on the postoperative results of recurrent anterior shoulder dislocations after the use of the Boytchev procedure, to review the published articles in the literature and to compare these overall results with those obtained with other open repairs to determine the effectiveness or otherwise of the Boytchev procedure and to see if any specific risk factors can be identified which might explain the discrepancies already noted and settle the disagreements between those who have observed conflicting tendencies [7, 8]. It should nevertheless be recognized that comparing different open repairs is difficult because of a remarkable variability in study designs.
Material and methods
No funds were received in support of this study. All the patients gave their informed consent prior to being included in the study; the study was authorized by the local ethical committee and was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki as revised in 2000.
For our present study, the patients were selected to meet the following criteria: clinical history of anterior shoulder instability as a result of a traumatic event, more than three episodes of shoulder dislocations, no clinical evidence of multidirectional instability, and eventual previous surgery to the injured shoulder for recurrent anterior dislocations, other than the Latarjet procedure.
Twenty consecutive recurrent anterior dislocations of the shoulder were treated by the Boytchev procedure between January 2002 and December 2009. All twenty dislocated shoulders were in male patients; one female patient refused treatment. The average age was 29.2 years at the time of the surgical intervention, with an age range of 17 to 42 years. Fourteen patients were affected on the right shoulder, and six on the left; the right was the dominant side in all the patients. The total number of dislocations suffered by individual patients ranged between 4 and 200, with an average of 19 in a period of three to eight years. The etiology of the dislocation was related to a fall in thirteen patients and to sporting activities in seven patients. All had a severe initial traumatism; their first dislocated shoulder had been put back by an experienced practitioner and immobilized for periods ranging from a few days (the immobilisation being removed by the patient) to a few weeks (five days to six weeks).Three patients had a minor amyotrophy. No patient had generalised ligament laxity. There were no spontaneous dislocations in our patients. All patients had some pain, but nine of them had significant episodes of pain, probably after subluxations, and all had positive apprehension tests and a feeling of instability and /or insecurity of the shoulder. Thirteen shoulders had a normal preoperative range of motion, while just one had restriction of elevation and external rotation; this patient had had previous surgical treatment using another procedure which had failed, the cause being an unhealed Bankart lesion diagnosed by arthro-scan. Four Hill-Sachs lesions and greater tuberosity fractures were diagnosed preoperatively by plain radiographs (frontal, profile, special radiographs, and sometimes CT scan or Magnetic Resonance Imaging (MRI). The follow up evaluation consisted of a clinical examination and radiographs (plain radiographs and/or special radiographs and/or computed tomography or Magnetic Resonance Imaging (MRI)). The Rowe score for instability of the shoulder, evaluating stability, motion and function and interpreting the results as excellent (100-90), good (89-75), fair (74-51) or poor (50 or less) was used for the results [9],(Table I).
Concerning the statistical analysis, we conducted a statistical analysis comparing the results of all published articles about the Boytchev procedure for treatment of recurrent shoulder dislocation. Using Pubmed, Cochrane, Lilacs, Japan Links Science, Index Copernicus, and Google Scholar, we performed a search of all published articles. 17 studies (14 published works, our own study and 2 cited by Dalsgaard) met the inclusion criteria with data about number of patients and number of recurrences of dislocation, which is the main concern here, follow up and gradation of results [7,10]. Our purpose is to estimate the true effect size using descriptive statistics to describe quantitatively the features of the data which may enable comparisons for the recurrence and results across the overall set of patients and dislocated shoulders and a multivariate correlation and regression tests between those variables, using XLStat, Sphinx Lexica and R softwares.
Operative technique
The incision begins from the level of the coracoid process, extending distally. We expose the horizontal part of the coracoid process with the tendinous origin of the short head of the biceps and the coracobrachialis muscle. An anteroposterior drill hole is made from the anterior end of the horizontal part of the coracoid process along its axis. The anterior 2 cm of the coracoid process is divided with an osteotome and mobilized distally gently to avoid a musculo-cutaneous injury (Fig.1) On the lower border of the subscapularis, we create a tunnel between shoulder capsule and muscle with a curved vascular forceps (Fig.2) (when the tunnel is created, we test the elasticity of the subscapularis introducing the fifth finger in the tunnel while making rotational movements), through which the isolated coracoid process with the conjoined tendons (Fig.3) is passed before being fixed to the predrilled proximal coracoid process with a 3.5 AO screw. The wound is closed in layers around a suction drain. A well padded dressing is applied. The arm is immobilized at the side of the chest with an elastic bandage.
Post operative management
During immobilization, isometric muscular reinforcement is begun. After removal of the elastic bandage, normally after three weeks, shoulder exercises are recommended. These are passive and active exercises, with special attention being paid to external rotational movement. (We did not recommend it immediately, but 4 weeks after open repair). All the movements are increased progressively by the patient himself and with the kinesitherapist for as long as is necessary to ensure recuperation of muscular strength, motion and proprioceptive control.
Results
In our series, the follow up period varied from 25 to 87 months, with an average of 52.05 months (4.3 years). Nineteen shoulders showed excellent and good results (Fig. 4); one showed poor results. No complications such as infections or neuro-vascular injuries were observed. One patient developed a glenohumeral osteoarthrosis, and at the seven-year follow up, the latest radiographic examination showed the arthrosis (Fig. 5) to be evaluated as grade 2 on Samilson and Prieto’s scale; however, function was not affected [11]. Full mobility of the shoulder was retained in 16 cases, except for some minor restrictions of external rotation: 15 degrees in three patients and 25 degrees in one. The recovery period ranged from less than three months in thirteen patients to more than three months in seven patients. Recurrence occurred in one patient (Fig .6) after a high-level traumatic event eleven months after surgery. On physical examination, this patient actually had subjective apprehension but no sign of abnormal positive apprehension; this patient was not satisfied, but he is now stabilized three years after surgery.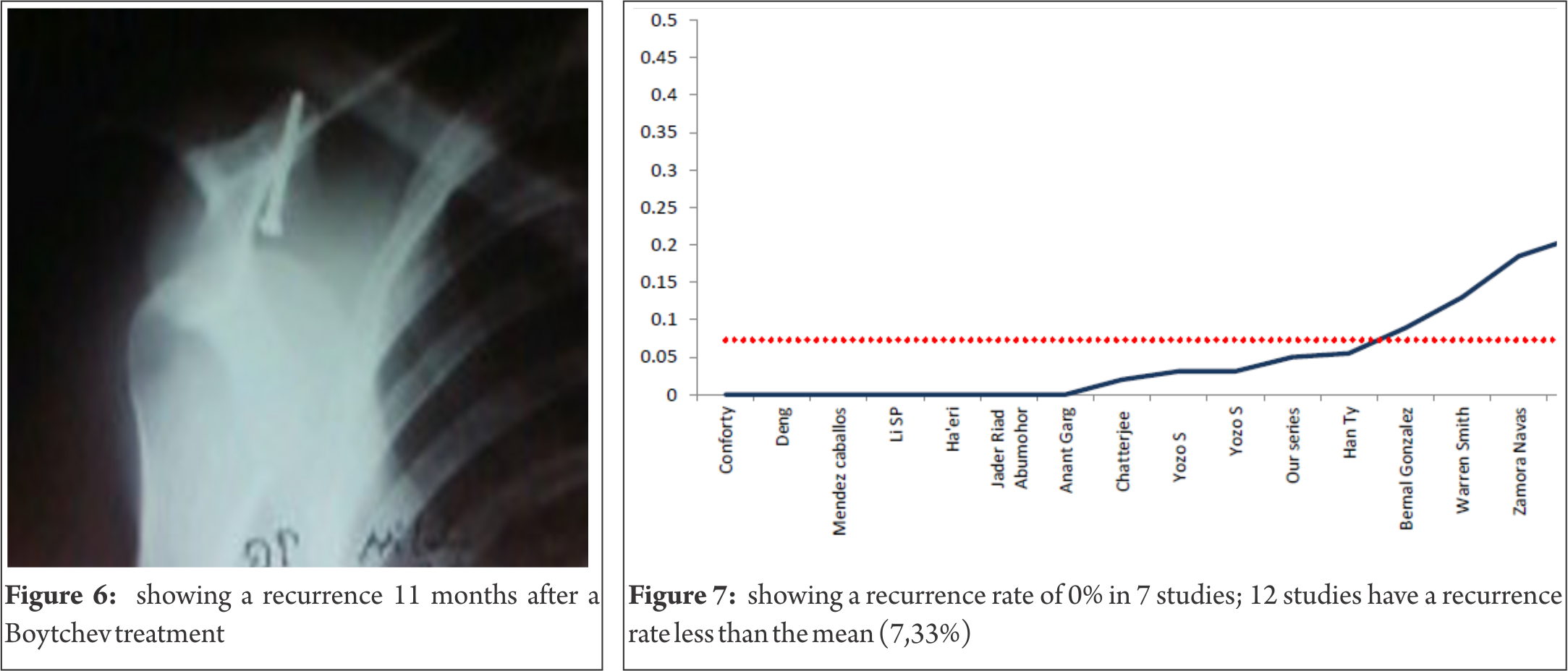
None of the patients complained of any significant pain (three patients complained about mild pain). All the patients were able to return to their normal activities (initial occupation or sport; seven were able to practise sport at more or less the same level).
As for the statistical analysis, among 477 patients with 485 dislocated shoulders, the overall outcome of recurrence ranges from 0 to 44%; we show a minimum of 0% in 7 studies (41.18%), a maximum of 44% in one study (5.88%) (Fig.7), a range of 44, a median of 3.1%, a mean of 7.33% with a standard deviation of [1.354 – 13.246] for p= 0.05 or7.33+-5.946). In 12 studies or 75% of dislocated shoulders, the recurrence rate is less than 7.33%, the percentage is 2% versus 21.08% in 5 studies, a difference which is statistically very significant (1-p=99.89%) (Fig.8). The statistical measures of dispersion show a robust index (Q1=0, Q3=8, 90, distance=8.90) for the interquartile range, the skewness value is -2.106, the kurtosis value is 4.006. The frequency and density distributions have a high incidence and range between 0 and 6.44% in 12 studies (71%) and the quartile’s estimation range between 0% and 5.50% in 12 studies (75%) (Fig.9). Concerning the gradation of results, we have 441 excellent and good results and 44 fair and poor (91% versus 9% with p=>99.9%), a difference which is also statistically very significant (Fig.10). The Pearson’s coefficient correlation with a level of signification alpha = 0.05 between the number of dislocated shoulders and excellent and good results has a p-value =0.000 versus a p-value =0.666 for fair and poor results. The regression test between the number of dislocated shoulders and excellent and good results has a high coefficient of correlation (0.97). Finally, regarding the time interval of recurrence in 12 studies, it varies from 1 to 43 months, with a mean of 31 months. The follow up time varies between 1.7 and 13.3 years, with a mean of 5.25 years.
Discussion
The twenty shoulders with recurrent anterior dislocations treated by the Boytchev procedure in this present prospective study were followed clinically and radiologically for periods ranging from a minimum of 2 years to a maximum of 8 years. Analysis of demographic data shows that all our patients are men in the third decade of life, whose activity requires moderate or extensive use of the shoulder joint, and whose dominant right shoulder was that affected by the recurrent dislocation. Almost all the results are excellent, except for the one instance of recurrence. The stabilisation of the shoulder by the Boytchev procedure allowed most patients to return to their former level of activity. One patient developed a glenohumeral arthrosis wiithout effect on function. Like the majority of the authors who have reported on this technique, we thus confirm that the Boytchev procedure seems not to be affected by variables such as gender, age, dominance, number of dislocations, direction and severity of traumatism, rehabilitation, and function over time [2, 4, 5, 6, 12, 13, 14, 15, 16, 17, 18].
As for the statistical analysis, to our knowledge (based on the literature) this is the first quantitative comparative statistical analysis of studies for the treatment of recurrent dislocation of the shoulder by the Boytchev procedure. 17 studies which reported the main factor which is the recurrence were included in our systematic review, in which we also extracted data on number of patients and dislocated shoulders, follow up, time interval of recurrence, and gradation of results, and we pooled the outcomes whenever possible. First, we took the outcome of recurrence for efficacy assessment, and we found no significant dependence between the number of dislocated shoulders and the rate of recurrence, the coefficient of correlation being +0.06, but there is a robust coefficient of correlation (+0.97) between the number of dislocated shoulders and excellent and good results; the dependence is a significant linear correlation (Fig.11). On the contrary, the dependence is not significant between the number of dislocated shoulders and fair and poor results (Fig.12), the coefficient of correlation being +0.26 (barely influential). Concerning the gradation of results, we have 441 excellent and good results and 44 35 fair and poor results or 91% versus 9%, a difference which is obviously very significant with an interval of confidence of 95%, with t=6.17 and p=>99.9. The multivariate analysis of regression concerning the number of dislocated shoulders compared to the rate of recurrence, the percentage of excellent and good results and the percentage of fair and poor results confirms the robust correlation between the number of dislocated shoulders and the number of excellent and good results compared to fair and poor results (Fig.13). So we can confirm the existence of two different groups with the probability of 0.87% to reject the hypothesis that the groups being compared differ to a degree greater than would be expected by chance.
Elsewhere in the literature, Chatterjee, in a 7-year follow-up study, reported one immediate recurrence after surgery, while Zamora-Navas, in his long term study, reported an 18% recurrence rate, recurrences occurring between 4 and 43 months later (a short or medium period after surgery) [2 ,8]. Warren-Smith found 13% of patients complaining of episodes of possible subluxation at an average of 14.3 months after operative treatment [19]. Finally, Dalsgaard, with the same period of follow up as Chatterjee (7 years), observed a high rate of recurrence (44%) [2, 7]. Dalsgaard did not report the time interval of recurrences following surgical repair and insisted on the fact that the surgical treatments were performed by 11 different surgeons; is this an inhomogeneous parameter for the study? We cannot grasp the reason for this discrepancy; Dalsgaard comments that the technique needs more study [8]. Concretely, we note a mean recurrence rate of 7.33%. Like most authors , we consider this result very acceptable [2, 4, 5, 6, 12, 13, 14, 15, 16, 17, 18], (Table II).
Some published reports on the incidence of recurrent dislocations after anterior repairs by procedures other than the Boytchev procedure cite rates ranging from zero to 30% [20, 21, 22, 23]. In 1976, Morey and Janes, in their study of 176 patients, found a redislocation rate of 11% [21]. The operative reconstructions were of the Bankart and Putti-Platt types; in 7 of the 20 patients, redislocation occurred two years after surgery. In 1984, Rowe et al reported on the management of 32 patients with recurrence of instability; 84% had not had effective repair of the Bankart lesion at the initial surgery [9]. In 1988, O’Driscoll and Evans, who followed 269 consecutive staple capsulorraphies, found that 21% suffered redislocation [22]. In 1995, Ungersbock and then Zabinski reported similar findings (unhealed Bankart lesions) [24, 25]; Karlson, reporting on Bankart repairs, found a recurrence rate of 15% after arthroscopic repair and 10% after Bankart open repair [20]. It should be noted that many of these reports did not include recurrent subluxation or recurrent apprehension. The incidence of recurrence is also underestimated by some studies and revealed by Rockwood and Roca Ramos Vertiz [26, 27] We may also note that in the literature the recurrence rate did not always increase with follow up for different procedures [28, 29]. Hovelius did not observe a significant difference in recurrence rates at two, five and ten years follow up after surgery on recurrent dislocated shoulders [28]. Rowe reported that 52% of the dislocations recurred within two years after operative procedures [29]. This is not the case with the Boytchev procedure reported in the compiled studies in the literature [2, 4, 5, 6, 12, 13, 15, 16, 17,18].
The results of anterior repair by the Boytchev procedure or by other procedures cannot be evaluated solely in terms of the rate of recurrence, even though the avoidance of recurrence is the aim of stabilization. Rather, we must place the treatment of recurrent instability in its overall context. Surgical repairs of glenohumeral instability may lead to a number of complications which can compromise the final result. These include limited range of motion, deep infection, recurrent post-operative instability, failure of diagnosis (it is essential to differentiate TUBS syndrome and AMBRII syndrome), muscle laxity or weakness of the subscapularis, neurovascular injuries, hardware complications and secondary degenerative disease. Limited range of motion has been reported after Magnusson Stack, Putti Platt and other procedures. In 1979, Hovelius reported an average loss of motion of 21 degrees of external rotation [28]. In our series, three patients had a minor or moderate loss of external rotation as reported by other authors; probably the tension of the subscapularis is increased by the rerouted muscles which pull it forward [5, 30].
Concerning secondary degenerative disease, we note one case in our series, and this is the first case reported following treatment with the Boytchev procedure. We think that it was not a consequence of the high number of dislocations (more than 200 dislocations in the patient concerned), because other authors like Chatterjee reported cases suffering very high numbers of dislocations (cases with 200, 250 and 500 dislocations) without degenerative disease, but rather that it was subsequent to stabilization by the force of the coracobrachialis and short head of the biceps muscles, acting as compressors of the head into the glenoid concavity and not only as a dynamic backstop [2]. The tip of the coracoid process with its muscles rerouted deep to the subscapularis also increases the compression from the subscapularis, which can hold the humeral head centred on the glenoid.
Shibata has also reported that the Boytchev procedure increases the pressure between the humeral head and the subscapularis tendon [18]. This pressure increases proprioceptive stimuli in the subscapularis tendon, and this accelerates the protective reflex needed to prevent shoulder dislocation. In our series, we did not observe any muscular weakness during the operative management (subscapularis, muscles attached to the coracoid process). In 2007, Lei-Sheng Jiang reported in his article that application of load to the conjoined tendon significantly reduced anterior displacement of the humeral head either with the capsule intact or with Bankart lesion simulated [31]. The most significant decrease of the anterior displacement occurred when the conjoined tendon was transferred beneath the subscapularis. Their findings show that the conjoined tendon per se has a stabilizing effect on unstable shoulders and therefore provide scientific support for the treatment of recurrent shoulder instability using the modified Boytchev procedure.
So we can assume, as other authors have done, for all types of open repair, that lesions, like bone deficiency, poor quality of soft tissues, decompensation of neuro-muscular control, hypoplasia, erosion or fracture of the glenoid rim, injuries of the rotator cuff, labrum, capsule (unhealed Bankart lesion), and ligaments are on the whole the main factors of shoulder instability and so lead to an unsteady glenohumeral stabilizing mechanism [24, 26 29]. Also like the majority of the authors who have reported on this technique, we thus confirm that the Boytchev procedure provides reliable stabilization of the shoulder and satisfactory function over time [2, 4, 5, 6, 12, 13, 14, 15, 16, 17, 18, 31, 32]. The fact remains that the gradation of results of the cited compiled studies confirms 441 satisfactory (excellent or good) results and 44 unsatisfactory (fair or poor), or 91% versus 9%, results which are obviously satisfactory, when generally compared with other procedures.
We can affirm that the Boytchev procedure is an effective technique and that other types of open repair do not offer better results in terms of stability, recovery of full range of motion, function and other complications. However, we do not plead for the superiority of this procedure and we insist on the fact that more studies are required to confirm these results.
Finally, we notice, as the majority of authors have done, that the Boytchev procedure provides reliable stabilization of the shoulder, satisfactory function over time and low recurrence rates (7.33% in 2% of the total dislocated shoulders reported on in the literature), and that it does not lead to more complications than other procedures. But even with these results, our conclusions must be drawn with caution, for a number of reasons: the limited amount of data available; the puzzlingly high recurrence rate in certain studies (Dalsgaard) [7]; the need for correct execution of the surgical procedure; the need for checks on the evolution of the patients; the importance of ensuring that the technique is in fact indicated; and the need for more cases to be studied, with longer-term follow up.
References
1 Allain J, Goutallier D, Glorion C: Long –term results of the Latarjet procedure for the treatment of anterior instability of the shoulder, JBoneJointSurg, 1998,80:841-52.
2 Anant Kumar Garg, Saankritya Ayan, Vikas K, Debi K, Kiran Kumar M, Biplab A: Modified Boytchev procedure for treatment of recurrent anterior dislocation of shoulder. Indian Journal of Orthopaedics. 2011 Jul-Aug; 45(4):336-340 DOI: 10.4103/0019-5413.82340
3 Bernal Gonzalez M, Cabrera Filtres N, Remon Davila, Xiomara de J. Alvarez Placeres L: Tratamiento quirurgico de la luxacion recidivante de hombro por la tecnica de Boytchev, Revista Cubana Ortop Traumatol, 2000, vol 14 :1-8
4 Boytchev B: Treatment of recurrent shoulder instability. Minerva Orthop 1951, 2:377-379
5 Chatterjee ND, Nath C, Pal AK, Baksi DP: Modified Boytchev procedure for the treatment of recurrent anterior dislocation of the shoulder. Int Orthop 2002, 26:7–9 DOI: 10.1007/s00264-001- 0303-7
6 Claes T: Boytchev anterior shoulder reconstruction: “no problem” surgery? Presented at the annual meeting of the American Orthopaedic Association, 1990, Boston,USA. (cited by Dalsgaard)
7 Conforty B: The results of the Boytchev procedure for treatment of recurrent dislocation of the shoulder. Int Orthop 1980, 4: 127- 132
8 Dalsgaard HL, Gothgen CB, Hoogmartens MJ: The Boytchev procedure for recurrent anterior dislocation of the shoulder: a controversial technique. Acta Orthop Belg 2000, 66:248–250
9 David Ip: Orthopedic-Traumatology:A resident’s guide. Second edition,Springer,2008: 252- 258 DOI 10.1007/978-3-540-75861-7
10 Deng J, Package J: Boytchev procedure for treatment of recurrent anterior dislocation of shoulder joint .Orthopaedic J China. 2003, 9:604-05
11 Ha’eri GB: Boytchev procedure for the treatment of anterior shoulder instability. Clin Orthop 1986, 206: 196-201
12 Han T, Zu Q, Xiang LB, Xian M: Modified Boytchev procedure for treatment of recurrent anterior dislocation of shoulder joint. J Clin Orthopaedics 2008, 6: 519-20
13 Hovelius L, Augustini BG, Fredin H, Johansson O, Norlin R, Thorling J: Primary anterior dislocation of the shoulder in young patients: A ten year prospective study, JBJS,1996, 78:1677- 84
14 Jader Riad Abumohor, Juan Montoya: Tratamiento de la inestabilidad anterior de hombro con la tecnica de Boytchev, Rev Med Hondur, 2009, 77 (1) 16-18 ,journal code :ISSN 0375-1112
15 Karlsson J, Magnusson L, Eperhed L, Hultenheim I, Lundin O, Kartus J: Comparison of open and arthroscopic stabilization for recurrent shoulder dislocation in patients with a Bankart lesion. Am J Sports Med, 2001, 29: 538-542
16 Lei-Sheng Jiang, Yi-Min Cui, Zhi-De Zhou, Li-Yang Dai: Stabilizing effect of the transferred conjoined tendon on shoulder stability, Knee surgery, Sports Traumatology, Arthroscopy, 2007, 15,6: 800-805. DOI:10.1007/s00167-006-0239-y
17 Mendez Caballos J.A, Saenz Lopez de Rueda F, Zamora Navas P, Flores Gallego F.J, Luna Sanchez C, Huerta Valderas J: Tratamiento quirurgico de la luxacion recidivante de hombro por transposicion del coraco biceps, Rev Esp de Cir Ost,1985, 20, 39-45.
18 Morrey BF, Janes JM: Recurrent anterior dislocation of the shoulder: long term follow up of the Putti Platt and Bankart procedures. J Bone Joint Surg.1976, 58 A: 252-256
19 O’Driscoll SW, Evans DC: The DuToit staple capsulorrhaphy for recurrent anterior dislocation of the shoulder: Twenty years of experience in six Toronto hospitals. American shoulder and Elbow Surgeons 4th Open Meeting, Atlanta, 1988.
20 Ping L, Chen F: Improved Boytchev treatment of habitual anterior dislocation of 15 cases. J Integr Tradit West Med China. 2007, 2: 513-14
21 Roca LA, Ramos-Vertiz: Luxacion erecta de hombro. Rev San Mil Arg.1962, 61: 135.
22 Rockwood C.A Jr, Green D.P: Part 2: Dislocations about the shoulder. J.B1.1, 2nd Ed, eds. Lippincot,Vo, Philadelphia,1984
23 Rowe CR, Patel D, Southmayd WW: The Bankart procedure: A long-term end-result study, JBJS 60-A,1978,1-16.
24 Rowe CR, Zarins B, Ciullo JV: Recurrent anterior dislocation of the shoulder after surgical repair: Apparent causes of failure and treatment. J Bone Joint Surg 66A:159, 1984.
25 Rowe CR: Prognosis in dislocations of the shoulder, J Bone Joint Surg., 1956, 38:957-977
26 Samilson RL, Prieto V: Dislocation arthropathy of the shoulder. J Bone and Joint Surg., 1983, 65- A: 456-460.
27 Shibata Y, Midorikawa K, Ogata K, Izaki T: Modified Boytchev and its combined operation for traumatic unstable shoulder. Shoulder Joint. 1999, 23: 327-1
28 Shibata Y, Honjo N, Shinoda T, Kumano T, Naito M (2004) Pressure between the humeral head and the subscapularis tendon after the modified Boytchev procedure. J Shoulder Elbow Surg 13: 170–173, DOI:10.1016/j.jse.2003.12.010
29 Ungersbock A, Michel M, Hertel R: Factors influencing the results of a modified Bankart procedure. J Shoulder Elbow Surg 4: 365-369, 1995.
30 Warren-Smith CD, Wallace WA, Ebrahimzade AR, Pailthorpe CA: Pitfalls with the Boytchev operation for recurrent anterior shoulder dislocation. Presented at the fourth International Conference on surgery of the shoulder, October 4-7, 1999, New York, USA. (cited by Dalsgaard)
31 Zabinski SJ, Callaway GH, Cohen S, Warren RF: Long Term Results of Revision Shoulder Stabilization. American Shoulder and Elbow Surgeons Meeting, La Quinta, CA, 1995. .
32 Zamora-Navas P, Borras Verdera A, Porras Garcia J, Padilla Marquez A, Linares P: Long-term results of the Boytchev procedure for the treatment of recurrent dislocation of the shoulder. Acta Orthopaedica Belgica, 2001, 67-3: 233-235
(Abstract) (Full Text HTML) (Download PDF)
Understanding Clinical Radiology of Fracture Acetabulum
/in Volume 2 | Issue 2 | May-Aug 2016Vol 2 | Issue 2 | May – Aug 2016 | page:9-16 | U K Sadhoo
Author: U K Sadhoo [1]
[1] Nayati Hospital, Mathura, U.P. 281003
Address of Correspondence
Dr. U K Sadhoo
Nayati Hospital, Mathura, U.P. 281003
Email: uksadhoo@yahoo.com
Abstract
Acetabulum is one of the most anatomically complex regions of the body. Fractures in this area are difficult to visualise due to complex anatomy and overlaping of radiological shadows. Plain radiology od acetabular and pelvis fractures require detailied understanding of the imaging techniques and anatomy. Newer advances like 3-D CT etc have added new dimensions to the radiological assessment of acetabular fractures. Current review focusses on basic radiological principles to help the readers understand and categorised acetabulam fractures an also plan the surgical intervention.
Keywords: Acetabular fractures, radiological asessement, CT Scan.
Introduction
Acetabulum is a major weight-bearing joint, connecting Axial skeleton to lower limbs. Therefore a fracture of Acetabulum has implications for the mobility and disability for rest of life. Until the pioneering work of Judet and Letournal (1), these injuries were poorly understood and inadequately treated. Now this sub-specialty has come of age. The difficulty in understanding the nature of these injuries is the complex shape of Pelvis anatomy. Radiology not only provides an accurate assessment, it also gives a pointer to the approach and definitive treatment. Judet and Letournal classification is based on the lines produced by xray beams on the cortical surfaces in AP and two 45 degree oblique projections. Though advent of CT has enhanced our understanding, this classification remains the de facto standard. The other classifications are AO/OTA classification and the CT based Harris et al classification (3,4)
Anatomy
Acetabulum is formed by confluence of Ilium, Ischium and Pubis into an inverted horse-shoe shaped structure that is deficient inferiorly, bridged by Transverse Acetabular Ligament. The central non-articular part is known as cotyloid fossa which houses fat (Pulvinar) and Ligamentum Teres (Fig 1). Bony Acetabulum has inclination of 55-60 degrees to horizontal. This is deepened by Labrum, a soft fibro-cartilagenous structure not unlike meniscus. This increases the load-sharing area and provides additional check against dislocation.
Radiology
X-rays (Fig. 3):
Look for 6 landmarks :
1. Post. Wall : Lateral-most projection on AP and Obturator view x-ray. Seen clearly because of anteverted Acetabulum.
2. Ant. Wall : Superimposed on post. Wall, still visible as undulation line on good quality x-ray.
3. Dome : weight-bearing area of acetabulum.
3 variants :
TransTectal : through weight-bearing area
Juxta Tectal : at roof of cotyloid fossa where it joins articular area
Infra Tectal : Through floor Cotyloid fossa. Juxta and infra-Tectal don’t involve weight bearing surfaces so rarely need operative measures.
4. Tear Drop : Not an anatomical structure. Seen on AP projection. Lateral wall represents inferior-most Acetabulum articular surface, medial boundary by Quadrilateral plate.
5. Ilio-Ischial line : representing Posterior column
6. Ilio-Pectineal line : representing Anterior column
AP View 1-minute assessment (Fig. 4) : Basic, quick, cheap investigation. Look at 4 lines, 1 curve, 1 circle; it gives lot of information, enough to make a considered decision about the severity of injury and urgency of treatment. It may not pick up subtle fractures, small intra-articular fragments, marginal impaction. There is virtually nil to be deduced from x-ray about the soft tissue component of injury.
Judet Views (Fig. 5,6,7) : Patient is tilted 45 degree to horizontal, once with injured side up, then normal side up, at right angle to each other. The x ray beam is perpendicular to Horizontal, focused on affected hip in both views.
Obturator : shows Iliac wing seen end-on, Obturator foramen in full profile. (highlights Anterior column, Posterior Wall)
Iliac : shows Iliac blade, Posterior column, Ant. wall (most lateral projection), Sciatic notch, Quadrilateral plate.
Sometimes, it is not possible to do Judet views because of patient discomfort. In such cases, angiographic C-arm can be tilted, instead of the patient, to gain necessary information (7).
Planar CT scan (Fig 8,9,10) : Thin-slice scans, axial, coronal and sagittal, are invaluable tool for complete evaluation of Acetabulum fractures. It can show marginal impaction, intra-articular fragments, subtle fracture lines, and posterior Sacro-Iliac injury. It thus complements the information gained on x-rays. In addition, soft tissue injury like Morell-Lavalle lesion can be picked up on CT (or MRI).
3D CT (Fig.11): It is a reformatted image from thin sections into 3D surface-rendered images. These images are easy to understand, easy to manipulate in any direction, with or without femoral head in acetabulum. No doubt finer details like intra-articular bone pieces, impaction, and fine fracture lines are lost but it remains a powerful tool to have a bird’s eye-view of a very complex anatomy and injury. One major advantage is the ability to process data into reformatted images (Fig.12) to appear as planar AP or Judet views without the need to move or tilt the patient (5).
CT can show fracture in coronal or sagittal planes; it can also be used with artefact-suppression software for post–op evaluation of adequacy of reduction, intra-articular metal or loose bone pieces (Fig 13). The fracture lines through the Dome need understanding to interpret the diagnosis correctly (Fig 14).
Proximal 10mm of Axial CT also corresponds to the weight-bearing Dome (6). Therefore, if a fracture does not involve the proximal 10mm of Acetabulum, conservative treatment is indicated.
Judet and Letournal Classification:
Before discussing Classification, it is important to keep the following points in mind:
-Fractures are described with respect to a lateral-facing Acetabulum (Fig 1). This is quite different from real-life situation in which Acetabulum is tilted anteriorly and inferiorly. Therefore, a Transverse fracture orients in oblique-sagittal plane in a Pelvis-AP x-ray than a horizontal line.
-Walls are part of the column (Fig 2). Therefore, it is possible to break either wall or column or both simultaneously. For a column to break, exit line is through Obturator oval in most, but not all, cases. Add to this, part or complete Transverse # element and many possibilities emerge.
10 fracture patterns are recognized (fig. 15, 16); 5 elementary and 5 associated which are combination of one or more of elementary pattern. All of them are based on the walls getting separated from columns and columns getting broken at Sciatic buttress, with transversely oriented fracture through Acetabulum completing the picture.
5 elementary types are Anterior Wall, Anterior Column, Posterior Wall, Posterior Column and Transverse fracture (Fig. 15).
5 Associated patterns (Fig. 16), as name suggests, are combination of two or more Elementary patterns. These are: Posterior wall and Column fracture, Transverse with Post Wall, T Shaped, Ant Wall/Column with Posterior Hemi-transverse and associated both column. Not every fracture can be pigeon-holed in these 10 patterns, but it is as good a working classification as any.
5 patterns of these 10 constitute 80% of all Acetabulum fractures: Post Wall, Transverse, Transverse with Post wall, T shaped and Both Columns (Fig. 30).(5,6)
Post. Wall ( Fig.17,18) : A part of the rim with articular surface is broken. Often, it is displaced with subluxed/dislocated head Femur and best seen on Judet Obturator view (Fig 5,6). Comminution is not uncommon. Sciatic involvement is not infrequent and subtle injury even more common. On CT, marginal impaction can be picked up easily (Fig. 8).
Ant. Column (Fig 19) : Uncommon. Pure Ant. Wall fracture is even less common. It generally is a hallmark of elderly, osteoporotic individuals.
Transverse # (Fig. 20) : The fracture runs obliquely and can exit through weight-bearing Dome, at junction with Cotyloid fossa or through fossa itself. The distal fragment displaces medially and rotates. Both these factors need to be taken into account at ORIF. Though the fracture line traverses both Ilio-Pectineal and Ilio-Sciatic line, thus involving Anterior AND Post Columns, it still is not a “Both Column” Fracture, a term reserved for
Post Wall and Column # (Fig 22, 23) : Post. Column break can occur in isolation or may be accompanied by Wall fracture. Column component exits proximally, Sciatic notch and distally, Obturator foramen. This is an unstable situation and at ORIF, Sciatic Nerve and Superior Gluteal neurovascular bundle are at risk.
Ant. Column with Post. Hemitransverse # (Fig. 24) : Not to be confused with Transverse or T #. The fracture line of Ant. Component exits obliquely compared to the straight line in Transverse #.
T-shaped # (fig. 25, 26) : The transverse component has additional break in Obturator fossa. This essentially separates Anterior and Posterior components. Therefore choosing appropriate approach is of paramount importance. Generally, the more displaced fragment decides approach. The other component is then reduced and held indirectly. Sometimes, two approaches may necessary.
Transverse with Post. Wall # (Fig. 27, 28) ; As name indicates, the post wall component makes the head displace posteriorly, often with communition.
Both Column # (fig. 29) : No part of the weight-bearing Dome is connected to the Sciatic buttress. On Obturator view, “Spur” sign is characteristic of this pattern.
Fragility Fractures : (Fig. 31, 32) : With increasing longevity, the fracture patterns are also changing due to osteoporosis. Anterior wall, column injuries are common and many injuries are because of trivial fall on Greater Trochanter.
“Gull wing” sign, which shows a depressed/punched-in part of weight bearing area, is a bad prognostic indicator.
Some of these fractures can be picked only on MRI and if, despite negative X-ray, a strong suspicion prevails, MRI is indicated.
Conclusion
Acetabulum fractures need evaluation comprehensively by X-rays and CT Scans. Only then can this complex injury to a complex region be understood. Radiology not only provides assessment of injury, it helps choose best possible approach for stabilization, if indicated..
References
1. Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res 1980;(151):81–106.
2. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium: 2007—Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21(10 suppl):S1–S133.
3. Harris JH Jr, Lee JS, Coupe KJ, Trotscher T. Acetabular fractures revisited: part 1—redefinition of the Letournel anterior column. AJR Am J Roentgenol 2004;182(6):1363–1366.
4. Harris JH Jr, Coupe KJ, Lee JS, Trotscher T. Acetabular fractures revisited: part 2—a new CT-based classification. AJR Am J Roentgenol 2004;182(6):1367–1375
5.Leschka S, Alkadhi H, Boehm T, Marincek B, Wildermuth S. Coronal ultra-thick multiplanar CT reconstructions (MPR) of the pelvis in the multiple trauma patient: an alternative for the initial conventional radiograph. Rofo 2005;177(10):1405–1411.
6. Olson SA, Matta JM. The computerized tomography subchondral arc: a new method of assessing acetabular articular continuity after fracture (a preliminary report). J Orthop Trauma 1993;7(5):402–413
7. Geijer M, El-Khoury GY. Imaging of the acetabulum in the era of multidetector computed tomography. Emerg Radiol 2007;14(5):271–287
8. Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum: a meta-analysis. J Bone Joint Surg Br 2005;87(1):2–9
9. Patel NH, Hunter J, Weber TG, Routt ML Jr. Rotational imaging of complex acetabular fractures. J Orthop Trauma 1998;12(1):59–63.
(Abstract) (Full Text HTML) (Download PDF)
Emergency Management of Pelvic Fractures
/in Volume 2 | Issue 2 | May-Aug 2016Vol 2 | Issue 2 | May – Aug 2016 | page:25-30 | Nadeem Akhtar Faruqui
Author: Nadeem Akhtar Faruqui [1]
[1] Regency Hospital, Kanpur , Uttar Pradesh, India.
Address of Correspondence
Dr Nadeem A Faruqui
14/116d, Civil Lines,
Kanpur 208001 India
Email: nafaruqui@hotmail.com
Abstract
Hemorrhage is leading cause of death following pelvic fractures. 15-25% of patients of closed pelvic fractures and 50% of open pelvic fracture patients die as a result of haemorrhage. The main source of hemorrhage is the shearing injury of posterior thin walled venous plexus (80%). Other sources of bleeding include the bleeding cancellous bone and arterial injury. Injury to the pelvic viscera is also quite common because of the close proximity. Perineal lacerations make a closed injury into an open injury thereby more than doubling the risk of morbidity and mortality. Adequate fluid replacement and application of a pelvic Binder or Sheet can markedly reduce the mortality associated with this fracture. A linen sheet folded onto itself to make it about 20-30 cms wide applied tightly over the pelvis and centered over the trochanters can significantly reduce the mortality figures.
Keywords: Acetabulum fractures, pelvis fracture, emergency management.
Introduction
The basic principles of emergency management, Airway, breathing and circulation hold true for pelviacetabular fractures too. However there are certain practical tips and principles that will help in getting better results in these situations. These principles and tips are detailed below.
Hemorrhage is Leading Cause of Death
15-25% for closed pelvic fractures and 50% for open pelvic fractures are fatal secondary to exsanguination following either external or internal occult bleeding [1,2]. Increased mortality associated with
– systolic BP <90 on presentation
– age >60 years
– increased Injury Severity Score (ISS)
– need for transfusion > 4 units
– Head and neck injuries
Sources of Major Bleeding
• intrathoracic
• intraabdominal
• retroperitoneal
• extremity (thigh compartments)
• pelvic
• Common source of hemorrhage
• venous injury (80%)
• shearing injury of posterior thin walled venous plexus
• bleeding cancellous bone
• Less common sources of hemorrhage
• arterial injury (10-20%)
• superior gluteal most common (posterior ring injury, APC pattern)
• internal pudendal (anterior ring injury, LC pattern)
• obturator (LC pattern)
Blood Transfusion
Replacement volume is estimated by using the formula of 3 ml of crystalloid for each 1 mm of blood loss. A minimum of 2 litres of crystalloid solution is given rapidly if the patient is in shock. Crystalloid is administered until type-specific blood of non–cross-matched universal donor (O-negative) is available
• Packed RBC:FFP:Platelets should ideally be transfused in the ratio 1:1:1
• this ratio has been shown to decrease mortality in patients requiring massive transfusion
D) Disability
Clinical Examination
Pelvis: NO firm endpoint on rotation or traction indicates that there is no gross instablity (Fig 1). Pelvic compression and distraction test can detect gross instabilities, however these may at times be dangerous and can dislodge clots leading to further bleeding [3,4]. These test have been reported to have poor sensitivity and specificity and are no longer recommended in cases of pelvic fractures [4]
Perineum (Fig 2): Look for
• lacerations of perineum
• degloving injuries
• flank hematoma
• scrotal, labial or perineal hematoma, swelling or ecchymosis
• urethral bleeding
Rectal Examination
mandatory to rule out occult open fracture
• rectal blood
• anal sphincter tone
• bowel wall integrity
• bony fragments
• prostate position
Vaginal Examination
mandatory to rule out occult open fracture
Presence of blood in vaginal vault
Vaginal lacerations
Urogenital Examination (Fig 3)
Bladder and the urethra are most frequently injured (25-30% of major pelvic fractures). 66% male versus 34% females patients difficulty in voiding urine or blood at the urethral meatus.
95% of bladder injuries have gross haematuria
urethral injuries are suspected under following clinical scenario
• blood at the urethral meatus
• gross hematuria
• inability to spontaneously void
• high riding prostate on rectal examination
• retrograde urethrogram (RUG) should ideally be done before insertion of Urinary catheter in unstable patient with suspected urethral injury make only 1 attempt to pass the urinary catheter, if it fails do RUG
Neurologic Examination
• rule out lumbosacral plexus injuries (L5 and S1 are most common)
• rectal exam to evaluate sphincter tone and perirectal sensation
Whenever an unstable pelvic injury is suspected in a haemodynamically unstable patient, a pelvic binder/sheet should be applied to control bleeding
The goal of treatment for pelvic fracture stabilization is early control of life-threatening hemorrhage. Returning pelvic bones to correct position helps to reduce pelvic volume and control venous bleeding.
Pelvic Binder [5,6]
• Applies compression leaving less space for blood to accumulate. It decreases the pelvic volume and also reduces pelvic fractures
• Tamponades bleeding sources, such as fractured bony surfaces or ruptured vessels
• Reduces instability of the injured pelvis
• Prevents further damage to pelvic organs and vessels
• Reduces pain by limiting movement of pelvis
Commercially available pelvic binder are also useful but use of lumbosacral belts is to discouraged [6].
Pelvic Binder/sheet
Indications
• initial management of an unstable pelvic ring injury
Contraindications
• hypothetical risk of over-rotation of hemipelvis and hollow viscus injury (bladder) in pelvic fractures with internal rotation component (LC)
• no clinical evidence exists of this complication occurring
Technique
• A linen sheet folded onto itself to make it about 20-30 cms wide is passed under the pelvis
• Centered Over Greater Trochanters to effect indirect reduction
• Applied very tightly over the pelvis
• do not place over iliac crest/abdomen as it makes the ineffective and precludes assessment of abdomen
• augmented with traction & internal rotation of lower extremities and taping at knees & ankles
• transition to alternative fixation as soon as possible
• prolonged pressure (>24 hours) from binder or sheet may cause skin necrosis
• working portals may be cut in sheet to place percutaneous fixation
Lumbosacral belt should not be used because it is elastic and cover abdomen.
Important note. Binder should be centered over the TROCHANTERS and Not the ASIS
Because of their ease of use and fast application, Pelvic Binders have
largely replaced the Pelvic C-Clamp and External Fixators for early
mechanical stability in pelvic fracture [5].
Radiology & CT
X-ray Pelvis –AP
Pelvis Is Unstable When There Is
Sacro-Iliac joint Diastasis > 1 cm or
Cephalad Displacement of Posterior Sacro-Iliac Complex > 1 cm
Usually associated with Avulsion fracture of ischial spine, ischial tuberosity, sacrum or transverse process of 5th lumbar vertebrae
High Risk Patients as per the Young and Burgess Classification:
– LC III
– APC II
– APC III
– VS
– CM
Ct Scan is the Gold Standard
CT scan is essential in determining:
Posterior ring instability
Helps define comminution and fragment rotation
Intra-articular fragments
Fractures of articular surface of acetabulum and femoral head
Ultrasonography
Allows Focused Assessment with Sonography for Trauma (FAST)
Four classic areas are examined quickly by ultrasonography for free fluid (Blood):
Perihepatic space (hepatorenal recess)
Perisplenic space
Pericardium
Pelvis
External Fixation/ Stabilization of Pelvic Ring Injury
These are temporary life saving measures in the acute stage to stabilize the pelvis in a haemodynamically unstable patient. However, None of these methods can fully stabilize the pelvis. These are put on till such time as more definitive fixation can be done.
Femoral traction pin with 10-12 kg weight should be applied to maintain the reduction of the hemipelvis.
Mode of Action of External Fixation
•Decreases pelvic volume
•Stabilizes bleeding bone surfaces and venous plexus in order to form clot
•Reduces Pain
Types
A) Pelvic Binder/sheet
B) Pelvic C Clamp
C) External Fixator
A) Pelvic Binder/Sheet
Easily available everywhere annd is easy to apply. Technique of application discussed previously
B) Pelvic C Clamp (Fig 6)
Indications
– Emergency stabilization of Sacroiliac joint disruptions and fractures of the sacrum with associated circulatory instability
Contraindications
Absolute contraindications are:
•Fracture lines within the illium (transiliac fracture) as it bears the risk of pin perforation through the fracture line
•Hemodynamic stability in Pelvic fractures
Relative contraindications are:
•Hemodynamic stability of the patient after Unstable type injuries
•Comminuted sacral fractures with risk of compression of the sacral nerve plexus
In life threatening situations hemorrhage control takes priority over the potential risk of nerve root compression
One Pin is inserted on each side of pelvis at the level of the Sacro-iliac joint. This point corresponds to the intersection of the line drawn along the long axis of the femur and a vertical line drawn from the ASIS with the patient supine. The 2 pins are connected with a C Clamp.
Advantage
Can be applied in the emergency room
Laparotomy can be done with the C Clamp in place
Disadvantage
Costly and not available everywhere.
Efficacy similar to Pelvic Binder/ Sheet.
C) External Fixator
Indications
Pelvic ring injuries with an external rotation component (apc, vs, cm)
Provide only marginal stability in vertically unstable ring injury
APC II (OPEN BOOK injuries with posterior ligaments/hinge intact) :
All designs work
APC III injuries (Post Ligaments damaged)
No designs work well (but AIIS frames better than ASIS frames)
Contraindications
•Ilium fracture that precludes safe application
•Acetabular fracture
Technique
Pin insertion in iliac crest (ASIS) (Fig 7)
multiple half pins inserted in the superior iliac crest placed in thickest portion of anterior ilium or gluteus medius tubercle
Should be placed before emergent laparotomy
• Stab incision over iliac crest
• Pass 2 K-wires by hand 1 each on medial & lateral sides of iliac wing
• Drill hole started at junction of Medial 1/3 & lateral 2/3rd of iliac crest
• 45 degree inclination lateral to medial
• Ceplalad to caudal direction – towards acetabulum
• Drill 1 cm
• 5 mm Schanz pin inserted with hand
• Cortical walls to guide pin into position
• Obturator Oblique view on C-Arm /Outlet view
Pin Placement In Anterior Inferior Iliac Spine (AIIS) Fig 8,9)
single pin in column of supra-acetabular bone from AIIS towards PSIS. Obturator outlet or “teepee” view can be used to visualize this column of bone. AIIS pins can place the lateral femoral cutaneous nerve at risk
Tranverse skin incision at or below AIIS
•Muscles split longitudinally to avoid lateral femoral cutaneous nerve injury
•Drill through trocar under image intensifier towards greater sciatic notch
•Pins directed 30-450 towards midline in frontal plane
•Pins directed perpendicular to body axis or slightly cephalad
•Schanz pins of 50-70mm thread length required
•Fixator bar connects the pins on both sides
•Permits easy access for laparotomy
Subcutaneous Pelvic Internal Fixator (INFIX) (Fig 10)
One pedicle screw is fixed in the supra-acetabular bone of the ilium on each side. The pedicle screws are connected to each other by a rigid, anteriorly bowed fixation rod passed subcutaneously superficial to the sartorius muscles [7]
Less infection and wound site morbidity
After Stabilization/ External Fixation Of Pelvic Ring Injury
A) Control Hemorrhage
B) Control Contamination
A) Control of Haemorrhage
1) Pelvic Packing (Fig 11)
Make Midline Incision, pack the wound with sponges. Apply External Fixator. DON’T TRY TO LIGATE THE BLOOD VESSELS..Re-open wound after 24-48 hours and then ligate the vessels if possible or required.
2) Angiography
Indications
•Small bore artery (sup gluteal or obturator) can be controlled by embolization
•No role in Venous or bony bleeding
Available only in select centres and success based on multiple variables including: stability of patient, proximity of angiography suite, availability and experience of staff
CT angiography useful for determining presence or absence of ongoing arterial hemorrhage (98-100% negative predictive value)
Contraindications
• not clearly defined
Technique
•selective embolization of identifiable bleeding sources
• if uncontrolled bleeding even after selective embolization, bilateral temporary internal iliac embolization may be effective
• complications include gluteal necrosis and impotence
B) Control of Contamination
• Debridement & Packing of Open Wounds
• Suprapubic Catherization
• Diverting Colostomy
Conclusion
Priciples of pelvis fracture damage control
External Fixation
Pelvic Binder
Pelvic C-clamp
External Fixator
Control of Haemorrhage
Pelvic packing
Angiography
Control of Contamination
Debridement & packing of Open Wounds
Suprapubic catherization
Diverting colostomy.
References
1. O’Sullivan RE, White TO, Keating JF. Major pelvic fractures: identification of patients at high risk. J Bone Joint Surg Br. 2005;87(4):530-3.
2. Kido A, Inoue F, Takakura Y, Hoshida T. Statistical analysis of fatal bleeding pelvic fracture patients with severe associated injuries. J Orthop Sci. 2008;13(1):21-4.
3. Lee C, Porter K. The prehospital management of pelvic fractures. Emerg Med J. 2007 Feb;24(2):130-3
4. Grant PT. The diagnosis of pelvic fractures by ‘springing’. Arch Emerg Med. 1990 Sep;7(3):178-82.
5. Bottlang M, Krieg JC, Mohr M, Simpson TS, Madey SM. Emergent management of pelvic ring fractures with use of circumferential compression. J Bone Joint Surg Am. 2002;84-A Suppl 2:43-7
6. Mohanty K, Musso D, Powell JN, Kortbeek JB, Kirkpatrick AW. Emergent management of pelvic ring injuries: an update. Can J Surg. 2005 Feb;48(1):49-56.
7. Vaidya R, Kubiak EN, Bergin PF, Dombroski DG, Critchlow RJ, Sethi A, Starr AJ. Complications of anterior subcutaneous internal fixation for unstable pelvis fractures: a multicenter study. Clin Orthop Relat Res. 2012 Aug;470(8):2124-31.
(Abstract) (Full Text HTML) (Download PDF)