
Nonunion distal radius fracture – Case series of 6 cases with Review of Literature
Vol 1 | Issue 1 | July – Sep 2015 | page: 31-35 | Dilip D Tanna[1], Ashok K Shyam[2]
Author: Dilip D Tanna[1*], Ashok K Shyam [2].
[1] Private Clinic, 3A new queens road back bay view , mama parmanand marg. Mumbai 400004, India.
[2] Indian Orthopaedic Research Group, Thane & Sancheti Institute of Orthopaedics and Rehabilitation, Pune, India.
Address of Correspondence
Dr D D Tanna
Private practitioner, 3A new queens road back bay view , mama parmanand marg. Mumbai 400004
Email: ddtanna@me.com
Abstract
Background: Distal radius nonunions are rare but complex problems. They can present with severe disability and functional limitation, however clear guidelines do exist due to sparse literature. We present our experience of 6 cases with review of literature
Material and Methods: Retrospective review of 6 cases (4 males and 2 females) was done. Two cases were primarily treated with closed reduction and cast while others underwent surgical procedures ranging from single to 4 procedures. All were treated with open reduction, strut bone grafting using iliac crest bone graft and internal plate fixation. Darrach’s procedure was done in 4 cases and Sauvé-Kapandji in 2 patients after distal radius reconstruction. Supplementary wrist splint or below elbow plaster cast, was given in all cases for 3 wks with gradual mobilization.
Results: All patients showed, radiological union at mean 4 months (range 3 to 6 months). Range of flexion extension at wrist and supination and pronation improved over 4 months period in all cases. Grip strength was 30 % weak compared with opposite side in 5 patients. There were no subsequent complications in our series and all patients reported satisfaction with the functional results
Conclusions: Nonunion distal radius are rare but respond well to principles of open reduction, strut bone grafting and stable fixation. Distal radio ulna joint requires management in form of either a Sauvé Kapandji procedure (in young patient) or Darrach’s procedure (in older patients)
Keywords: nonunion distal radius fracture, open reduction internal fixation, bone grafting, Sauvé Kapandji, Darrach’s procedure.
Introduction
Distal radius fractures are one of the commonest fractures encountered in orthopaedic practice. Due to metaphyseal location, most fractures unite and nonunion is an unfortunate occurrence that poses a difficult scenario to treat [1,2]. Treatment of nonunion distal radius fracture depends on the size of the distal fragment, bone quality, amount of radial shortening, condition on distal radioulnar joint (DRUJ) and patients demands [1,2,3]. In cases with thin distal fragments, wrist fusion is suggested while with a sizable distal fragment a reconstruction is reported to be successful in maintaining the wrist range of motion [2,3]. In cases of distal ulna instability or incongruity procedures like Sauvé Kapandji procedure or Darrach’s procedures are combined with stabilization of distal radius [2,4,5,6]. However literature is still sparse and guidelines are still unclear. The current series adds our experience of 6 patients of nonunion distal radius treated surgically and is accompanied with detailed literature review to propose a guideline for treatment of such nonunions.
Materials and Methods
A retrospective review of database was conducted and six cases of nonunion distal radius presenting to us during last 10 years [between 1997 to 2010] were included in the study. There were 4 males and 2 females with mean age of 47.8 (range 22 to 91) (Table 1).  Out of 6 patients 5 were AO Type A and 1 was AO type C. Five cases were closed while one was grade 1 compound primarily. Four cases were fall on outstretched hands while two cases were fall from height. However since all cases were treated at other centres, direct assessment of soft tissue injury was not available to us. One patient was diabetic and one was hypertensive. One patient was chronic smoker while rest had no other significant co-morbidities. Cases 1 and 2 were elderly and were treated primarily with a cast but continued to have pain and deformity after cast removal.
Out of 6 patients 5 were AO Type A and 1 was AO type C. Five cases were closed while one was grade 1 compound primarily. Four cases were fall on outstretched hands while two cases were fall from height. However since all cases were treated at other centres, direct assessment of soft tissue injury was not available to us. One patient was diabetic and one was hypertensive. One patient was chronic smoker while rest had no other significant co-morbidities. Cases 1 and 2 were elderly and were treated primarily with a cast but continued to have pain and deformity after cast removal.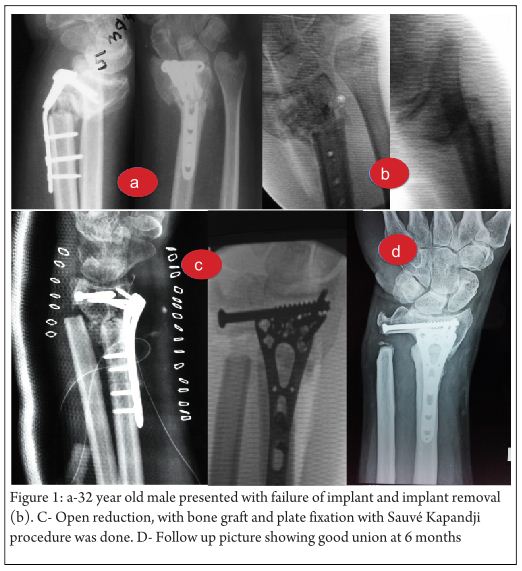 The remaining four were treated operatively with ORIF using simple non-locking distal radius plates. Two were multiply operated with same procedure and presented with implant failure. One case had primary open reduction internal fixation with non locking distal radius plate. The repeat surgery involved implant removal and re-application of cast. The second case was primarily treated with distal end radius non locking plate. Second surgery was only local bone grafting. Third surgery was implant removal and re-application of same implant with bone graft. Fourth surgery was implant removal after which wrist was simply immobilized in a below elbow cast at which time the patient presented to us. There were no infected nonunions. Only one case was atrophic nonunion while the others were oligotrphic. All patients complained to pain, deformity with functional limitation in carrying out daily activities comfortably.
The remaining four were treated operatively with ORIF using simple non-locking distal radius plates. Two were multiply operated with same procedure and presented with implant failure. One case had primary open reduction internal fixation with non locking distal radius plate. The repeat surgery involved implant removal and re-application of cast. The second case was primarily treated with distal end radius non locking plate. Second surgery was only local bone grafting. Third surgery was implant removal and re-application of same implant with bone graft. Fourth surgery was implant removal after which wrist was simply immobilized in a below elbow cast at which time the patient presented to us. There were no infected nonunions. Only one case was atrophic nonunion while the others were oligotrphic. All patients complained to pain, deformity with functional limitation in carrying out daily activities comfortably. 
All patients were operated with strut bone graft and internal fixation as described below
Surgical procedure.
Under general anesthesia, scar tissue was excised and adjacent bone surfaces were freshened. Tri cortical cortico-cancellous bone graft was obtained from iliac crest along with extra cancellous bone graft. This strut graft was trimmed to fit in the gap at the fracture site, and was wedged in the non-union giving it good stability. Further cancellous graft was put in the remaining, bone gap. Volar locking plate was applied with divergent screws engaging in the styloid process and in medial end of the radius. One patient operated many years back before the era of volar locking plates was treated with ordinary dorsal plate. This fixation was supplemented by K wires. Darrach’s procedure was done in 4 cases and Sauvé-Kapandji in 2 patients after distal radius reconstruction. We preferred Darrach’s procedure in elderly patients in our series and did Sauvé Kapandji for younger patients. Supplementary wrist splint or below elbow plaster cast, was given in all cases for 3 wks. Period. Gradual mobilization was started after 3 weeks with intermittent splint use. At 6 wks. External support was discarded and further mobilization continued. Figure 1 and 2 show two typical cases of our series. The key to the procedure is the iliac crest block graft that offered stability and restored length (Fig 3).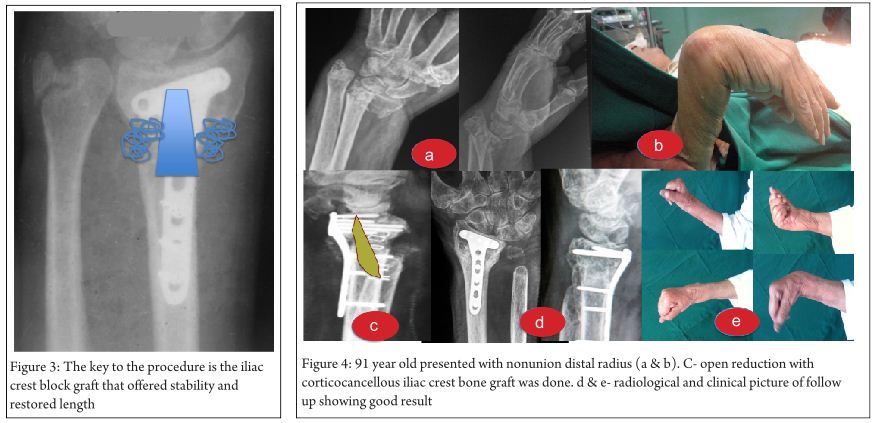
Results
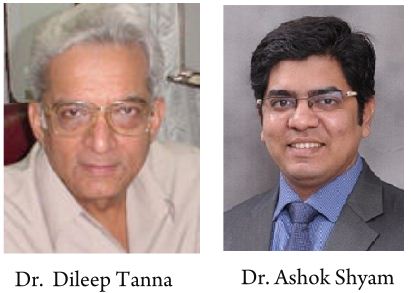
All patients showed, radiological union at mean 4 months (range 3 to 6 months). Range of flexion extension at wrist and supination and pronation improved over 4 months period in all cases. Grip strength was 30 % weak compared with opposite side in 5 patients. In one patient of 91 yrs old who was operated after 6 months of non-union had wrist drop pre operatively, (Fig 4) showed improvement in the wrist strength, and other functions, but grip strength, improved only by about 50%. He had tendon rupture after first surgery and hand function improved after tendon grafting was done. Whether additional k wires and external support was mandatory, is difficult to establish. But in this unstable situation, it did not result in decreased movements. One medical student who had compound fracture (Fig 5), which was treated with 3 surgical procedures before he ended up in non-union had with radio carpal radiological involvement, was offered, wrist fusion.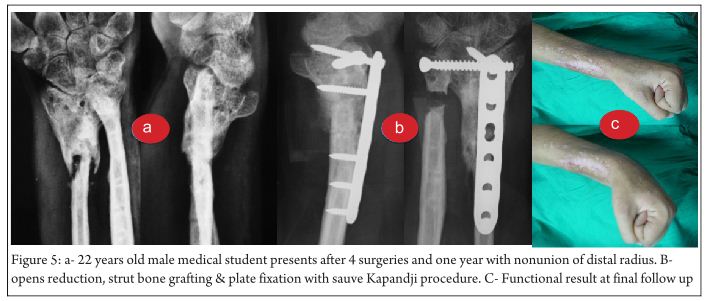 He being a medical student and desiring orthopedic surgical carrier was reassessed carefully. He demonstrated inter carpal movements, and requested, to preserve that movement. He was treated by volar long dynamic compression plate without wrist fusion. He preserved his decent inter carpal movements with fracture union. How long he will remain painless is uncertain. There were no subsequent complications in our series and all patients reported satisfaction with their final functional results
He being a medical student and desiring orthopedic surgical carrier was reassessed carefully. He demonstrated inter carpal movements, and requested, to preserve that movement. He was treated by volar long dynamic compression plate without wrist fusion. He preserved his decent inter carpal movements with fracture union. How long he will remain painless is uncertain. There were no subsequent complications in our series and all patients reported satisfaction with their final functional results
Discussion
Nonunion of distal radius fractures are rare and no definite guidelines are available. We operated 6 of such cases using principles of strut graft, internal fixation and a DRUJ procedure. Union was achieved in all cases with good functional results.
A detailed literature review revealed 20 publication on distal radius fracture nonunion with total of 77 cases reported (Table 2) [1-4, 7-22]. Variety of factors were considered while making a clinical decision in these articles. Wrist fusion was reported by early articles and may be needed in cases with severe collapse, poor bone quality and as salvage procedure after repeated surgery [1, 19]. Earlier the size of distal radius fragment was considered to be very critical. Segalman and Clarke suggested that in cases with less than 5 mm distal fragment size, reconstruction will fails and thus primary wrist fusion should be attempted [6]. Four years later, Prommersberger et al suggested that in cases with less than 5 mm distal fragment can still be reconstructed if bone stock is good and stable fixation can be achieved [12]. The main surgical procedure for nonunion distal radius is open reduction, freshening of nonunion, iliac crest bone grafting to achieve as much radius length as possible and stable internal fixation using a plate construct. Stability is one of the key elements in treatment of distal radius nonunion. In present series a combination of techniques are used to archive stable fixation. Corticocancellous graft not only provides a biological stimulation but also behaves as a mechanical support to maintain the radial length. Volar plating and additional K wires were used to achieve stable fixation and good results were achieved in all our cases. Two studies have reported use of biplanar fixation of distal radius by using two plates at right angle to each other [15,16], however in our series we could achieve good results with single volar locking plates.
Procedures on DRUJ are needed in cases with arthrosis, instability and incongruity of DRUJ or where there is severe shortening of radius [2]. There are two procedures that have been used, the Darrach’s procedure and Sauvé Kapandji procedure. The indications and preference of one procedure over other is still debatable. Advantage of Sauvé Kapandji is that it provides a broad support to carpus bones and thus may prevent deformities or subluxation of the carpus and maintains good load transmission [7]. Again it is reported older patients with less demands will do well with a simpler Darrach’s procedure while Sauvé Kapandji is preferred in younger individuals. We preferred Darrach’s procedure in elderly patients in our series and did Sauvé Kapandji for younger patients. One specific disadvantage of Sauve Kapandji procedure was mentioned by Karuppiah and Johnson [7]. They recommended against use of this procedure in cases where severe radial collapse has occurred but length was restored by surgery. They hypothesized that due to restoration of length there will be significant amount of tension on the ulna soft tissue sleeve which may lead to restricted forearm rotation. They also pointed on importance of maintaining adequate tension in this soft tissue sleeve to prevent ulna stump instability. Justin and Sheung-tung reported a case where mid-shaft ulnar shortening osteotomy was done to reduce the DRUJ [20]. They fixed the ulna osteotomy with additional plate and reported good result. Probably this procedure can be used in cases with no DRUJ arthrosis. Failure to address issues of DRUJ have led to persistent pain even in cases with good radius union [5] and thus DRUJ should always be considered while treating distal radius nonunion.
Various factors have been proposed as cause of these nonunions. Tobacco and alcoholism are linked with increased incidence of distal radius nonunion [12], however none of our patients was a smoker or alcoholic. Diabetes, obesity, open fractures with soft tissue injuries are all implicated as compounding factors [3,12]. Presence of combined distal radius with distal ulna fracture [2,5], use of external fixation and used of pins and plasters [5,20] are also indicated to add to occurrence of nonunion. We feel the main reason for nonunion is unstable fixation or inadequate immobilization [2]. In one of our case primary fracture was compound and may have contributed to nonunion. In all stability was the main issue and when a stable fixation with bone grafting was done it could achieve good results in all our cases. Although over good union rates are reported, complications like plate breakage, persistent nonunion and graft donor site infection are reported with revision surgeries. In our series we had one case which presented as failure of revised fixation and bone grafting. However repeat revision with same procedure finally achieved union. No other complications were noted.
Our series has the inbuilt shortcomings of a retrospective study. However the event of distal radius nonunion is rare and hence difficult to plan large size prospective study. Different in patient profile and also available implants confound the surgical choice, however the principles of surgery remained the same and thus provide valuable inferences.
Conclusion
In conclusion, as brief guideline, we can say that in cases of distal radius nonunion, the nonunion should be treated with open reduction, strut bone graft and stable fixation. If DRUJ procedure is needed, Sauvé Kapandji procedure should be preferred in young patients while in old patients a Darrach’s procedure will give good results. Wrist fusion should be the last resort as a salvage procedure. Most nonunions will respond well to this approach with good clinical and functional results.
References
1. Prommersberger KJ, Fernandez DL. Nonunion of distal radius fractures. Clin Orthop Relat Res. 2004 Feb;(419):51-6.
2. McKee MD, Waddell JP, Yoo D, Richards RR. Nonunion of distal radial fractures associated with distal ulnar shaft fractures: a report of four cases. J Orthop Trauma. 1997 Jan;11(1):49-53.
3. Segalman KA, Clark GL. Un-united fractures of the distal radius:Areport of 12 cases. J Hand Surg. 1998;23A:914–919
4. Gómez EA, Mena RV. [Treatment of distal radius non-union in a three-stage procedure. Case report]. Acta Ortop Mex. 2009 Jan-Feb;23(1):26-30
5. Prommersberger KJ, Fernandez DL, Ring D, Jupiter JB, Lanz UB. Open reduction and internal fixation of un-united fractures of the distal radius: does the size of the distal fragment affect the result? Chir Main. 2002 Mar;21(2):113-23
6. Watson-Jones R. Fractures and other bone and joint injuries. 2nd edition. Edinburgh: Livingstone; 1942.
7. Karuppiah SV, Johnstone AJ. Sauvé-Kapandji as a salvage procedure to treat a nonunion of the distal radius. J Trauma. 2010 May;68(5):E123-5
8. Hamada G. Extra-articular graft for non-union in Colles’s fracture. J Bone Joint Surg 1944;26:833-835.
9. Bacorn RW, Kurtzke JF. Colles’ fracture: a study of two thousand cases from the New York State Workmen’s Compensation Board. J Bone Joint Surg 1953;35A:643-658.
10. Harper WM, Jones JM. Non-union of Colles’ fracture: report of two cases. J Hand Surg 1990;15B:121–3.
11. Saleh M, Ribbans WJ, Meffert RH. Bundle nailing in nonunion of the distal radius: case report. Handchir Mikrochir Plast Chir 1992;24:273-275.
12. Smith VA, Wright TW. Nonunion of the distal radius. J Hand Surg Br. 1999 Oct;24(5):601-3
13. Fernandez DL, Ring D, Jupiter JB. Surgical management of delayed union and nonunion of distal radius fractures. J Hand Surg 2001;26A:201–9.
14. Grecco Marco Aurélio Sertório, Angelini Luis Carlos, Oliveira Marcelo Tavares de, Trombini Nelson, Martins Francisco Carlos, Barbosa Sônia Maria de Almeida Pacheco. Treatment of nounion in the third distal of the radio. Acta ortop. bras. 2005;13(2): 95-99.
15. Ring D. Nonunion of the distal radius. Hand Clin. 2005 Aug;21(3):443-7
16. Crow SA, Chen L, Lee JH, Rosenwasser MP. Vascularized bone grafting from the base of the second metacarpal for persistent distal radius nonunion: a case report. J Orthop Trauma. 2005 Aug;19(7):483-6
17. De Baere T, Lecouvet F, Barbier O. Breakage of a volar locking plate after delayed union of a distal radius fracture. Acta Orthop Belg. 2007 Dec;73(6):785-90.
18. Villamor A, Rios-Luna A, Villanueva-Martínez M, Fahandezh-Saddi H. Nonunion of distal radius fracture and distal radioulnar joint injury: a modified Sauvé-Kapandji procedure with a cubitus proradius transposition as autograft. Arch Orthop Trauma Surg. 2008 Dec;128(12):1407-11.
19. Cao J, Ozer K. Failure of volar locking plate fixation of an extraarticular distal radius fracture: A case report. Patient Saf Surg. 2010 Nov 25;4(1):19.
20. Koo Siu-Cheong Jeffrey Justin, Ho Sheung-Tung, Non-union of Fracture of Distal Radius: A Case Report and Literature Review, Journal of Orthopaedics, Trauma and Rehabilitation, June 2011; 1(1):21-24
21. Nusem I, Moghaddam AK. Darrach’s ulnar resection and ulna intercalary bone graft for non-union of the distal radius: two birds one shot. Eur J Ortho Surg Traumatol 2011;21:345-349
22. Rappo TB, Kanawati AJ. Non-Union Of Fractured Distal Radius Treated With A Volar Locking Plate: A Case Report. The Internet Journal of Orthopedic Surgery. 2012 Volume 19 Number 2.
| How to Cite this article: Tanna DD, Shyam AK. Nonunion distal radius fracture – Case series of 6 cases with Review of Literature. Trauma International July-Sep 2015;1(1):31-35 |
{kind=link}