LICENSE
![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X

![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X
Digastric Trochantric Flip Osteotomy When and How to do it in Acetabular Fractures-?
/in Volume 3 | Issue 1 | Jan-April 2017Vol 3 | Issue 1 | Jan – Apr 2017 | page:24-26 | Harish Makker
Author: Harish Makker [1]
[1] Consultant Orthopaedic Surgeon, Lucknow, India
Address of Correspondence
Dr.Harish Makker.
282, Rajendra Nagar,opp.water Tank, Lucknow, India 226004 India.
Email: drharishmakkar@gmail.com
Abstract
There comes a time in acetabular fractures-posterior wall and or posterior column fractures when simple Kocher-Langenbeck Approach seems handicapped and you need to have some extension, as in cases of cranial extension of posterior wall fractures and /or need to retrieve loose segments from acetabular joint when with all efforts made by traction, space seems wanting.
Kocher-Langenbeck Approach used for posterior and posterior column injuries and also for some T type fractures, gives very little access to intra articular injuries despite a good traction.
Gluteus medius tenotomy and Trochantric osteotomy was done earlier [still being done by some ] but of late Digastric Flip Osteotomy is gaining popularity as it is less traumatic and helps saving blood supply and ,thus reduce chances of AVN.
The femur head is dislocated anteriorly or posteriorly, without much difficulty and internal status of the joint is observed without having to worry about devascularization of acetabular wall leading to further complications.
So to enumerate the need for Digastric Flip Osteotomy in acetabular fractures are-
1.-intra-articular fragments,
2. Impaction of fragments
3. Posterior wall comminution free fragments,
4. Superior acetabular rim or dome fractures,
5. Assessment of the reduction of the anterior Column, and finally
6. Intra-articular assessment of placement of a long screw inserted into the anterior column.
Keywords: Digastric flip osteotomy posterior wall, posterior column, intra articular fragments, head dislocation.
Introduction
Pelvi acetabular injuries are almost 6 percent of all trauma. The figure has recently increased in big and small cities due to introduction of high speed vehicles- two and four wheelers, and youngsters more affected [1] because of their experimenting more on these vehicle die to adrenalin rush. Mostly these are high impact injuries [2]
The other sector involved is old and osteoporotic adults, who encounter minor mishaps at home, or fall from height in both the categories. The protocol of treatment changes with age involved and facility /or absence of experienced surgeons in this sub specialty of orthopaedics, availibity of implants and instrumentations and high demand units in the hospital
Surgical Technique—
The technique was described Siebenrock et al.[3]
The initial steps are same as Kocher Langenbeck approach. Skin Incision is followed by, incision of fascia lata in line with skin incision, on deep dissection interval between gluteus maximus and
Medius fibres are seen, this interval is seen in proximal part only. Further dissection is done on
Ilio tibial tract distally. In some cases we may have to detach a small portion of gluteus maximus from lateral part of femur in distal part of dissection. Now the gluteus medius muscle fibre are split with utmost care, next – the trochanteric bursa is dissected and the posterior border of the gluteus medius muscle is exposed at the postero superior border of greater trochanter, along with tendinous insertion of gluteus medius. Fascia of gluteus medius and muscle belly of gluteus maximus are now mobilized preserving blood supply from superior gluteal artery.
Now we need to identify the external rotators of hip and here comes the help from two vascular anastomosis. first is Trochantric anastomosis communicates with ascending branch of medial circumflex artery at the superior border of Quadratus Femoris Muscle ,second vascular marking is branch of superior gluteal artery which is seen on the inferior border of piriforms muscle, this also anastomoses with ascending branch of medial circumflex artery.
By far we are missing an important structure ie Sciatic Nerve, which is now to be identified in its path, posterior to Quadratus Femoris Muscle.
In Arthoplasty cases we usually do not try to see any further but here we need to trace the Sciatic Nerve proximally upto Piriformis Muscle and try to assess its anomalies –if any.[ there are various anomalous positions of Sciatic Nerve which may prove harmful if not identified at this juncture-viz- front of Piriformis, Behind Piriformis ,In between two bellies of Piriformis ,more than one branch of Sciatic Nerve taking different positions in relation to Piriformis Muscle ] and at the risk of being damaged if not traced pre hand. The Nerve is traced where it enters the
Greater Sciatic Notch. In cases where there is single bundle in front of Piriformis Muscle, no
further attempt is made and we come back and no cutting of external rotators, but if there are two bundles of Sciatic Nerve at different positions, we might cut the Piriformis away from GT by at least 1 cm, avoiding damage to nerve in dislocating femoral head.
Next step is, developing Piriformis Muscle, for this Piriformis is retracted inferiorly, while Gluteus Medius is retracted superiorly and Gluteus Minimus is separated along its inferior fascial border. This release is extended upto greater sciatic notch taking care not to damage superior gluteal vessels and nerves. This will clear the area upto mid supra acetabular area.
The Gluteus Minimus can now be seen beneath Gluteus Medius and separation between piriformis and minimus is now carried out, we need to retract piriformis as Minimus carries the circumflex vessels with it and as such needs to be sharply separated from retro acetabular area.
Trochantric anastomosis is now cauterized and osteotomy site is marked by a marker pen or the cautery itself. Now a oscillating saw is used [refr-1] from the tip of greater trochanter to base of
Vastus tubercle.It is better to pre drill the GT so as to ease the fix with screws after job is over.it
is also better to leave a small portion of medius anteriorly with femur ,initially ,till the trochanter is mobilized. This small step provides a prevention from possible injury to retinacular vessels from thick osteotomy. The osteotomy runs lateral to short extensors ,which are left attached to femur and this also helps protect deep branch of medial circumflex artery, which lies deep to obturator externus muscle,[ref-4]
The fascia of vastus lateralis is incised from vastus tubercle, the trochanter is slowly and
cautiously lifted anteriorly and at this stage the remaining fibre attachment of gluteus medius detached from greater trochanter .The piriformis muscle is mostly attached to intact part of GT,
but if its fibres are attached to detached part-they are cut. The hip is now flexed and externally rotated; this causes gluteus minimus mobilization from retro acetabular surface along the capsule to its attachment to femur.
If the gluteus minimus comes in the way of greater trochanter, it can be released from femur to give full displacement to greater trochanter. The trochanteric flip osteotomy, per se ends here but the exposure to operating surface requires visualization of acetabular rim and capsule. The flexion and ext. rotation of hip and mobilization of vastus medialis does the job and entire hemi circumferential rim of capsule is visualized.
A z shaped capsulotomy is performed starting from superior part of capsule and coming down. This aids in intra articular visualization of loose fragments and its restoration.
Here we should see if posterior wall is fractured because if it is fractured, we should modify capsulotomy .carefully incorporating posterior wall. Now this is reflected inferiorly to visualize
the joint. The labrum may be avulsed with posterior wall segment.
The fractured column is now brought close by various instruments and plating is attempted on column. If piriformis or conjoint tendon of obturator internus and gemeli come in the way of plating, they are released two cm posterior from its insertion.
Finally when the plating is over, capsule is stitched loosely, greater trochanter is reattached with
3.5-4 mm screws, Vastus lateralis fascia is stitched and short ext. rotators are reattached. Gluteus
Muscles are reattached over deep drains, ilio tibial tract stitched and then the skin.
Conclusion
This is a very good approach for posterior wall and /or column fractures with superior extension and some T type fractures and saves the morbidity caused by extended approaches. This is now being more often than before.
References
1..Judet R, Judet J, Letournel E (1964) Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am 46:1615–1646
2. Liebergall M, MosheiV R, Low J et al (1999) Acetabular fractures: clinical outcome of surgical treatment. Clin Orthop Relat Res 366:205–216.
3. Siebenrock KA, Gautier E, Ziran BH et al (2006) Trochanteric flip osteotomy for cranial extension and muscle protection in acetabular fracture Wxation using a Kocher–Langenbeck approach. J Orthop Trauma 20:S52–S56.
4. Glas PY, Fessy MH, Carret JP et al (2001) Surgical treatment of acetabular fractures: outcome in a series of 60 consecutive cases. Rev Chir Orthop Reparatrice Appar Mot 87:529–538
5. Rommens PM, Gimenez MV, Hessmann M (2001) Posterior wall fractures of the acetabulum: characteristics, management, prognosis. Acta Chir Belg 101:287–293.
(Abstract) (Full Text HTML) (Download PDF)
A Rare Case of Simultaneous Bilateral Elbow Dislocation in a 25 year old Lady following a Simple Fall – An Unusual Mode of Injury
/in Volume 3 | Issue 1 | Jan-April 2017Vol 3 | Issue 1 | Jan – Apr 2017 | page:46-48 | Supreeth Nekkanti, C Vijay, Sujana Theja, R Ravi Shankar, Ishani Patel
Author: Supreeth Nekkanti [1], C Vijay [1], Sujana Theja [1], R Ravi Shankar [1], Ishani Patel [1]
Department of Orthopaedics, JSS Hospital,
Mysore, Karnataka, India
Address of Correspondence
Dr. Supreeth Nekkanti,
No. 160, 11th Cross, 5th Main, 1st Stage, NGEF Layout, Nrupatunganagar, Nagarbhavi,
Bengaluru-560 072, Karnataka, India.
Email: drsupreethn@gmail.
Abstract
Introduction: Bilateral elbow dislocation is a rare injury, with only a small number of case reports in the literature. The majority of these reports describe associated ligamentous injuries only. Simultaneous bilateral radial head fracture in association with bilateral elbow dislocation has only been described on two occasions previously.
Case Report: We report an extremely rare case of simultaneous bilateral elbow dislocation in a 25 years woman following self-fall. Bilateral elbow dislocation with bilateral radial head fractures was confirmed radiographically. Closed reduction under sedation was performed in the emergency room. The patient was immobilized for 5 weeks. The patient was mobilized and had good function of bilateral elbow at 8-month follow-up.
Conclusion: The purpose of this report was to describe a very rare injury pattern, to present the treatment approach chosen for this case, and to emphasize the importance of early mobilization following bilateral elbow dislocation.
Keywords: Bilateral elbow dislocation, female, rare case report, simultaneous.
What to Learn from this Article?
Simultaneous bilateral elbow dislocations are extremely rare injuries in non athletic patients in the absence of generalised ligament laxity. There should be a high index of suspicion for associated injuries by careful examination and evaluation with radiographs. Prompt reduction and early rehabilitation ensures an excellent functional outcome.
Introduction
In adults, elbow dislocations are the second most common dislocation after that of the shoulder, with an estimated incidence of 5.21 dislocations per 100 000 person-years. Simultaneous elbow dislocations are rare,some injuries may be associated with radius head and neck fractures, however, with only a handful of cases described in the literature so far. Our proposition is to report this rare case of bilateral elbow dislocation with bilateral radial head fracture and to present the treatment approach chosen for this case.
Case Report
A 25-year-old female, housewife weighing 95kgs was brought to the emergency department by ambulance with simultaneous bilateral elbow dislocations after landing on both hands with extended elbows. The parents reported no of history consistent with joint hyperlaxity of the patient. There was no positive family history for joint hyperlaxity
Clinical examination showed deformity of both elbows with loss of posterior triangular relationships of the olecranon and epicondyles suggesting bilateral posterolateral elbow dislocation associated with swelling and haematoma formation. There was no neurovascular deficit.Radiographs showed bilateral posterolateral elbow dislocations with a bilateral radial head fracture. (Figure1) Both elbows were reduced under sedation within an hour of the injury. The radial head fracture was undisplaced. She was splinted at 90° of flexion for 3 weeks with an above elbow slab. A check radiograph of both the elbows was taken to confirm the reduction of the elbow joints. (Figure 2) After seven days, the swelling subsided and slab was converted to an above elbow cast. At the end of five weeks both the casts were removed and she underwent physiotherapy. By the end of the 8th week the patient had regained functional range of movement and at twelve weeks she was doing her regular house work. (Figure 3, 4, 5)
Discussion
Elbow dislocation is a common event, being the most frequent joint subject to dislocation after the shoulder, the majority being posterior [2,3,4]. It is common for children to suffer an associated fracture and many are the result of sporting injuries [1]. Bilateral elbow dislocations occurring simultaneously however are extremely rare. Reported cases of bilateral elbow dislocation have been limited to young female gymnasts with proven joint hyperlaxity [3,4,5] and an isolated hang-gliding accident in an adult male, [3] and remain rare.The rarity of bilateral elbow dislocation stems from the fact that it may only occur under special circumstances with both the elbows extended and most of the body weight acting through the elbow joints with elbows in extension and hands outstretched [3,4,5].
Elbow dislocations form 11 to 28% of all injuries to the elbow [3,4]. The most common mechanism of injury is fall on outstretched hand. The body weight generates a downward force with vertical and horizontal component which unlocks the ulna out of trochlea [3]. As the elbow joint continues to hyperextend, the anterior capsule and collateral ligaments fail leading to posterior dislocation of the elbow joint [2,6]. Bilateral posterior elbow dislocations occur in special instances where the patient tries to stop his fall with both hands outstretched at the time of impact [3,4,5].
Cadaveric studies have shown that posterior dislocation is most likely with the elbow between 15 and 30° of flexion [7] and that a rotatory torque applied to the ulna, e.g. in a fall with the forearm pronated, plays a role in the mechanism of dislocation [6]. With the elbow in full extension, the majority of stress is directed on the tip of the coronoid process [7].
Josefsson et al, [8] in 1987, reported outcomes achieved through the analysis of surgical treatment of the elbow dislocation against the non-surgical one, concluding that surgical treatment should not be provided in a simple dislocation, which can be reduced by closed means.
It is agreed that prolonged immobilisation results in poor outcome, [2,3,4] and periods of acceptable immobilisation vary from immediate mobilisation to four weeks immobilisation, although this depends on the post-reduction stability of the elbow [2,4].
In the present study, the patient totally recovered the flexion- extension motion of the left elbow, with good valgus and varus stability. In the eighteen-month follow-up period, the X-ray control was shown to be normal, and the patient returned to all her daily activities
Complications like adhesions, fibrosis, myositis and contractures have been observed by Syed et al [3,9]. Protzman [3,10] had studied the degree of remnant flexion contractures of the elbow after immobilisation to vary from 3 to 21 degrees depending on the duration of immobilisation. In our patient we observed a remnant flexion contracture of around 5 degrees. However our patient did not present with any instability of the elbow or recurrence of the posterior dislocation. She had good functional range both the elbows
Conclusion
He purpose of this report was to describe a very rare injury pattern, to present the treatment approach chosen for this case, and to emphasise the importance of early mobilisation following bilateral elbow dislocation.
References
1. J.A. Mehta, G.I. Bain Elbow dislocations in adults and children. Clin Sports Med, 23 (4)(2004), pp. 609–627
2. A.A. Syed, J. O’Flanagan. Simultaneous bilateral elbow dislocation in an international gymnast. Br J Sports Med, 33 (2) (1999), pp. 132–133
3. A. Wilson. Bilateral elbow dislocation.Aust N Z J Surg, 60 (1990), pp. 553–554
4. A.A. Tayob, R.A. Shively. Bilateral elbow dislocations with intra-articular displacement of the medial epicondyles. J Trauma, 20 (4) (1980), pp. 332–335
5. J.O. Søjbjerg, P.Helmig, P. Kjærsgaard-Andersen. Dislocation of the elbow: an experimental study of the ligamentous injuries.Orthopedics, 12 (3) (1989), pp. 461–463
6. H. Wake, H. Hashizume, K. Nishida, et al. Biomechanical analysis of the mechanism of elbow fracture-dislocations by compression force.JOrthopSci, 9 (2004), pp. 44-50
7.Josefsson PO, Gentz CF, Johnell O, Wendeberg B. Surgical versus non-surgical treatment of ligamentous injuries following dislocation of the elbow joint. A prospective randomized study. J Bone Joint Surg Am. 1987; 69: 605-8.
8.MelhoV TL, Noble PC, Benett JB, et al. Simple dislocation of the elbow in the adult. Results after closed treatment. J Bone Joint Surg [Am] 1988;70:244–9.
9.Protzman RR. Dislocation of the elbow joint. J Bone JointSurg [Am] 1878;60:339–41.
(Abstract) (Full Text HTML) (Download PDF)
Functional Outcome of Unstable Intertrochanteric Femur Fracture Patients Treated with Trochanteric Fixation Nail
/in Volume 3 | Issue 1 | Jan-April 2017Vol 3 | Issue 1 | Jan – Apr 2017 | page:32-37| Yashwant J Mahale ,Vikram Vilasrao Kadu
Author: Yashwant J Mahale [1] ,Vikram Vilasrao Kadu [1]
[1] ACPM Medical College, Dhule – 424001 , Maharashtra India ,
Address of Correspondence
Dr. Vikram Vilasrao Kadu,
C/O Vilas Shamrao Kadu, Plot No. 20, Kadu House, Barde Layout, Friends Colony, Katol Road, Nagpur – 440 013, Maharashtra, India.
E-mail: dr.yashwant.mahale@gmail.com
Abstract
Introduction: Intertrochanteric fractures are disabling injuries that most commonly affect the elderly population. These fractures have a tremendous impact on both the health-care system and society in general. These fractures can be managed by conservative methods, but mal-union and complications of prolonged immobilization are the result. Thus, surgery by internal fixation is the ideal choice. Dynamic hip screw was the gold standard treatment for intertrochanteric fractures before intramedullary devices were developed. These devices have the advantage of being an intramedullary fixation device, shorter lever arm of devices causing less tensile strain on the implant, controlled fracture impaction due to the incorporation of sliding hip screw, shorter operative duration, and less soft tissue dissection. In view of these consideration, this study of management of unstable intertrochanteric fractures using trochanteric fixation nail (TFN) is taken up to assess the outcome in terms of adequacy of fixation and results.
Methods: In a retrospective controlled study, 40 patients of unstable intertrochanteric fracture were treated by TFN. Mean age group of the patient was 61.78 years. 26 cases showed union at 3 months, 13 cases showed union at 4 months, and 1 case showed union at 5 months duration.
Results: Functional results were assessed in the 40 cases available for follow-up. Excellent results were noted in 10 cases, good in 27 cases, fair in 3 cases, and none had poor result. Anatomical results were assessed by presence or absence of shortening and range of movements. 37 cases had good results and 3 had poor result.
Conclusion: At present, we consider that the TFN is a good minimally invasive implant for unstable intertrochanteric fracture when closed reduction is possible. Technical and mechanical complications were mostly related to the operative technique and the type of fracture and pre-operative reduction of the fracture.
Keywords: Shortening, trochanteric fixation nail, unstable intertrochanteric fractures.
What to Learn from this Article?
TFN is a novel implant based on the experience of gamma nail. Minimally invasive TFN, despite few
unfavorable results and complications is a satisfactory method in treating unstable it fractures. It requires closed monitoring during pre,
intra and post-operative period to avoid complications, which can be easily managed.
Introduction
Inter-trochanteric fracture most commonly affect the elderly population and also in young. The incidence has increased significantly during recent years due to the advancing age of the world’s energy trauma, whereas in the elderly age group most of the fractures are osteoporotic, resulting from a trivial fall. [1] These fractures have a tremendous impact on the health care system and society in general. These fractures can be managed by conservative methods, but mal-union and complications of prolonged immobilization is the end result. Thus, surgery by internal fixation is the ideal choice. DHS is the gold standard treatment for inter-trochanteric fractures. [2] In cases of unstable inter-trochanteric fractures, the incidence of limb shortening, medialization of distal fragment and implant cut-outs is high. [1] This led to the development of intramedullary devices. Numerous variations of intramedullary nails have been devised to achieve a stable fixation and early mobilisation of trochanteric fractures. Among these the trochanteric fixation nail (TFN) devised by the AO/ ASIF group in 1996 has proven to be a promising implant in per-, inter- or subtrochanteric femoral fractures. [3] These devices have the advantage of being an intermedullary fixtion device, shorter operative duration and less soft tissue dissection.
Purpose of the Study
To study the outcomes in terms of adequacy of fixation and stability and to evaluate end results
and complications.
Material and Methods
The study consisted forty cases of unstable inter-trochanteric fractures of femur treated surgically with Trochanteric fixation nailing at our institute between 2010 to 2014. The fractures were classified according to Boyd & Griffin’s classification. Type-IV cases were mainly excluded because of extension of the fracture onto the proximal shaft since problems were encountered with fixation of the distal locking screw which mainly crossed the fractured fragment while using conventional TFN (180mm). All the 40 Patients were available for follow-up.
The age of the patients in the study, ranged from 30 years to 88 years, average being 61.78 years. Out of forty patients, sixteen were females and twenty four were males. The Most common mode of Injury in our series were trivial fall accounting for 19 cases, followed by road traffic accidents in 14 cases and fall from height in 7 cases. Right side was affected in 19 cases and left in 21 cases. Our series consisted of 40 cases of unstable inter-trochanteric fractures. Inter-trochanteric fractures were classified according to Boyd & Griffin classification. Cases were followed at regular intervals. This study was conducted with due emphasis for clinical observation and analysis of result after surgical management of unstable inter-trochanteric fractures of femur with Trochanteric fixation nail. Following the treatment, patients were discharged and followed up at regular intervals for clinical and radiological evaluation. The patients were followed up till fracture union and functional recovery was achieved. If necessary, subsequent follow up was done. At the arrival of the patient with suspected trochanteric fracture, patients were resuscitated depending on their general conditions. Fractures were stabilized using skin traction, alternatively with Thomas Splint.
A thorough preoperative assessment of patients were done, which include general condition of patients, clinical and radiological assessment of fractures, type and size of fragments. Once stabilized, all the patients were shifted to ward & skin traction was applied varying on the built of the patient. Analgesics were given accordingly. Patients were evaluated for associated medical problems and reference was taken from respective departments and necessary treatment started. Associated injuries were evaluated and treated simultaneously. Functional results were assessed based on the functions gained by the patients following surgery and points were awarded accordingly. The factors taken into consideration in assessing were Hip pain, Ambulatory status, Ability to squat, Walking distance, Sitting cross legged.
Observation and Results
Surgery was performed on average of 8 days with a range of 4-14 days Due to financial constrain and other comorbid conditions. The delay was due to the general and medical conditions of the patients and managing associated injuries. Duration of surgery was longer in the initial operated cases. With frequent use of the nail system the duration has come down. Duration was longer in managing inter-trochanteric with subtrochanteric extension fractures type III, due to the difficulty in achieving anatomical reduction. Reduction was easier in type II inter-trochanteric fractures. Difficulty was noted in comminuted fractures and in cases with longer delay for surgery. Amount of blood loss was very less as compared to an average hip surgery. Blood loss was measured in terms of mop count and suction collection. The average amount of blood loss was 80 ml (range 60-120ml).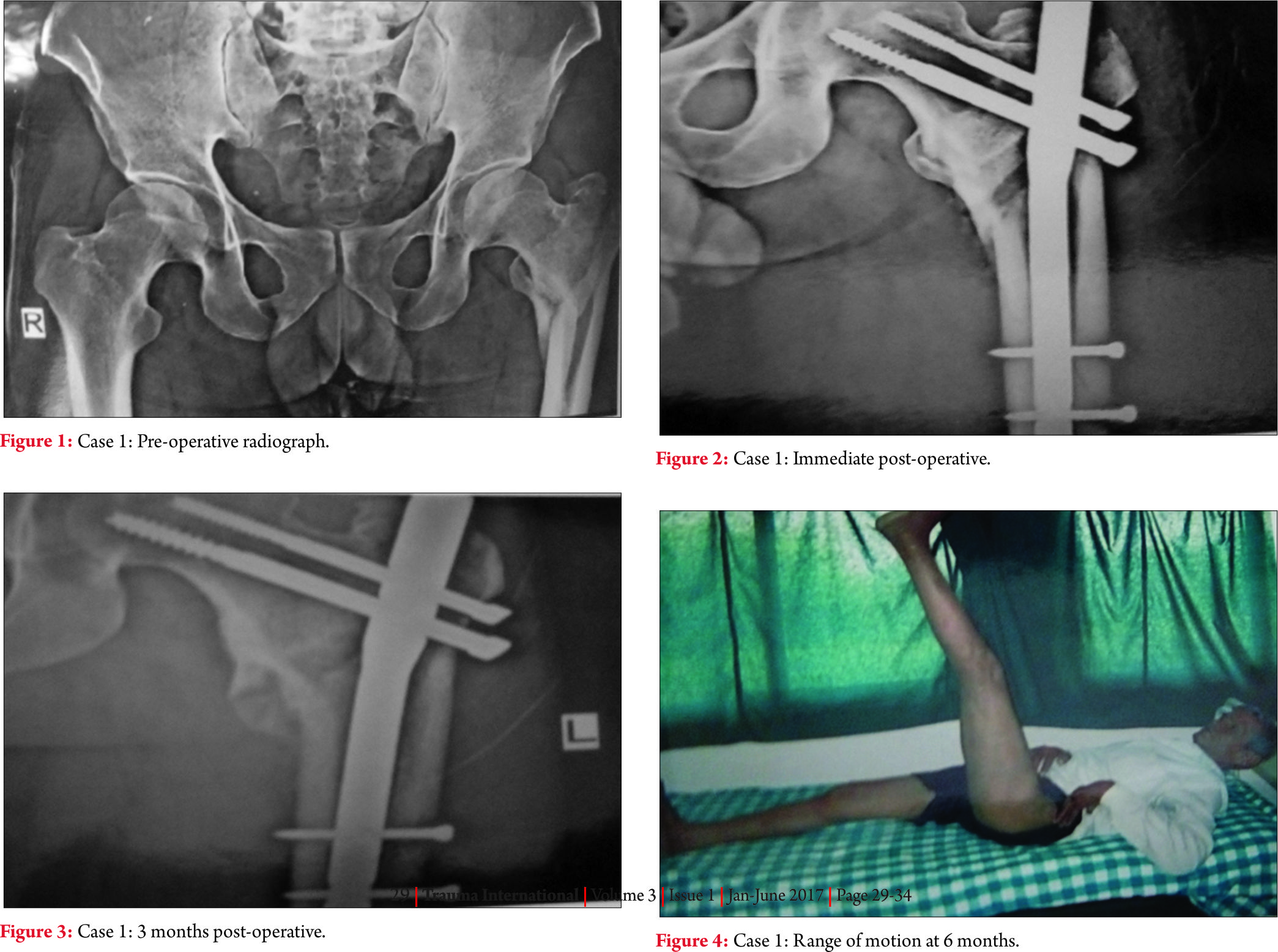
We encountered few complications in our study intra-operatively
1.Jamming of nail in the proximal fragment while insertion was noted, requiring progressive reaming of the proximal fragment and use of lesser diameter nail.
2.In one case manual distal locking had to done due to mismatch of the zig and nail, occurring intra-operatively.
3.In one case fixation of the fractures in varus angulation took place.
4.In one case iatrogenic fracture of lateral cortex of proximal fragment was noted.
Post Operative complications
In our series we had 2 cases of superficial wound infection which required appropriate intravenous antibiotics for 2 weeks period followed by 4 weeks oral antibiotics. No other complication like deep venous thrombosis, systemic infection, acute respiratory distress syndrome, fat embolism etc were noted.
Delayed complications
A case of varus collapse was noted in inter-trochanteric fracture type III with shortening of up to 1cm, due to the prominence of the screw laterally which was managed with regular follow up, to wait for the fracture to unite & implant removal. Stiffness of knee was noted in 2 cases which required vigorous physiotherapy, with full recovery of the range of movements. Stiffness of hip was noted in 2 cases due to the complications associated (Z effect and reverse Z effect) which were managed subsequently.
Duration
The average duration of hospital following surgery was 21.35 days ranging from 15-28 days. Patients were prescribed supportive drugs such as analegesic, antibiotics and other drugs as per associated medical conditions. Patients were advised to do physiotherapy such as quadriceps strengthening exercise, knee bending exercises and chest physiotherapy. Patients were instructed non weight bearing with bed rest upto 6 weeks post-operatively and were gradually made ambulatory with partial weight bearing using walker or crutches depending on the radiological signs of union and pain tolerability at subsequent follow up.
Morality
There was no mortality in this series of study.
Follow up
The average duration of follow up was 3 months ranging from 1-6 months, of which all the patients were available for follow-up.
Radiological union
Radiological union was said to be achieved on the evidences of presence of bridging callus and haziness of the fractures line on antero-posterior and lateral radiographs. 26 cases showed union at 3 months, 13 cases showed union at 4 months duration and 1 cases showed union at 5 months duration.
Anatomical result
Anatomical results were assessed by presence or absences of shortening, deformities and range of movements. 92.5% of the cases had good results and 7.5% had poor results.
Functional results
Functional results were assessed in the 40 cases available for follow up. Excellence was noted in 10 cases, good in 27 cases, fair in 3 cases and none had poor results.
Discussion
Inter-trochanteric fractures of the femur are relatively common injuries among the elderly individuals. Sometimes the associated generic problem makes it a terminal event in the lives of elderly individuals. In order to reduce the morbidity and mortality associated with conservative management of inter-trochanteric fractures, surgical management of the inter-trochanteric fractures is advocated as the best modality of management of these fractures.
Various fixation devices are available for the fixation of inter-trochanteric fractures. Most of the fixed angle nail plates were associated with many complications. Many intramedullary devices have been introduced after the development of the sliding hip screw with side plate assembly, but have their own restrictions.
In cases of unstable inter-trochanteric fractures the incidence of limb shortening, medialization of distal fragments and implant cutouts is high. This led to the development of intramedullary devices. These devices have the advantage of being an intramedullary fixation device, shorter lever arms of devices causing less tensile strain on the implant, controlled fractures impaction due to incorporation of sliding hip screw, shorter operative duration and less soft tissue dissection but however radiation exposure were high in the initial cases due to lack of experience and in cases of difficulty in reduction as compared to other modality of treatment. The average duration of radiation exposure was 60 seconds in cases of TFN which is comparatively more as compared to DHS plating which averages to 40 seconds. [4]
Amount of blood loss using trochanteric fixation nail was very less compared to an average hip surgery. Blood loss was measured in terms of mop count and suction collection. The average amount of blood loss was 80 ml (range 60-120ml) which is comparatively less as compared to DHS plating which average to 300ml. [5]
Trochanteric fixation nail attempts to combine the advantages of a sliding lag screw with those of intramedullary fixation while decreasing the moments arm as compared with that for a sliding nail plate system. It can be inserted by a closed procedure which retains the fractures haematoma, are important consideration in fracture union (MC Kibbin1978) and reduced both exposure and dissection.
Inter-trochanteric fractures almost invariability occur as a result of a fall, involving both direct and indirect forces. [6,7] Mulley and espley [8] demonstrated that inter-trochanteric fractures which occurred in hemiplegic patients sustained a trauma directly over the side secondary to impaired locomotor function and discuses osteoporosis on that side. Direct force act along the axis of the femur or directly over the greater trochanter to result in an inter-trochanteric fracture. Indirect forces include forces including pull of the iliopsoas muscle on the lesser trochanter and the abductors on the greater trochanter have also been incriminated as a cause of the fracture. [6]
When there is cortical instability on one side of a fracture due to cortical overlap or destruction, a fracture tends to collapse in the direction of such instability. [9] A truly stable inter-trochanteric fracture, therefore, is one that, when reduced, has cortical contact without a gap medially and posteriorly. [10,11]
Early operative treatment of trochanteric fractures reduces both mortality and morbidity (laskin, gruber and Zimmerman,1979) giving best chance of early independence and reducing the risk of prolonged bed rest. In the management of inter-trochanteric fractures of femur, it is important to re-establish bone to bone contact to the postero-medial cortex.
The trochanteric fixation nail (TFN) AO-ASIF device introduced in 1996 was designed to reduce the risk of implant complications. Studies have shown that screw cut out occurred by varus collapse and concomitant rotation of the femoral head around the neck axis (seral B et al 2004, sommers MB et al 2004 ) therefore in addition to the 8mm load bearing femoral neck screw, the TFN has a 6.5 mm autorotation screw to increase the rotational stability of the fragment. The derotation screw is inserted first to prevent possible rotation of the proximal fragment at the time of insertion of hip screw. An anatomic 6 degree neck valgus bend in the coronal plane, a narrower distal diameter and distal flexibility of the nail eliminates the need for routine reaming of the femoral shaft and also minimizes stress concentration and postoperative femoral shaft fractures.
The aim of our study was also to assess the epidemiology and functional outcomes of inter-trochanteric fractures with newer method of intramedullary fixation with trochanteric fixation nail.
The Z effect was seen in one patient mainly because of comminution of the medical cortex. The postoperative reduction of the fracture was not anatomic and the proximal screws had been placed higher than the level of the tip of the nail. A possible explanation the Z- effect phenomenon is the impaction of the hip pin into the proximal hole of the nail while the neck screw is normally sliding back during the weight-bearing period. The proximal fragment and the femoral head are moved back normally, whereas the impacted hip pin protrudes through the head. The reverse Z- effect occurred with the movement of the hip pin towards the lateral side. The mechanism is similar, but here the hip pin is sliding back, whereas the neck screw remains impacted to the hole of the nail.
Failure of fixation was seen in 3 cases which included one case of z effect, one case of reserve Z effect as mentioned above and one case of varus collapse of the fracture due to excessive comminution of the fracture. All these patients were managed with regular follow up to wait for the fracture to unite & subsequently implant removal.
One case of delayed union was seen due to varus collapse of the fracture because of excessive comminution and severe osteoporosis.
In 2 of our cases we had to perform open reduction due to wide displacement of fragments, comminution of fragment and in cases with delay in surgery of days due to comorbid conditions.
Trochanteric fixation nail can be used in cases of open injuries, which as compared to closed fracture is however extremely rare. Since it is an intermedullary device, it provides better strength and stability but on the contrary when using in open injuries the wound should be devoid of any contamination and should be healthy and clean. The patient should be operated as early as possible within 6 hrs since the time of accident.
Conclusion
TFN is a novel implant based on the experience of gamma nail. In the light of these results, one can conclude that the TFN, despite few unfavourable results and complications is a satisfactory method in treating unstable IT fractures. It requires closed monitoring during pre, intra and post – operative period to avoid complications, which can be easily managed. It however requires large study population with a long term follow-up.
Reference
1.Robert W Bucholz, James D Heckman, Charles M Court-Brown, Rockwood and Greens volume 2, 6th edition; pages 1827-44.
2.GS kulkarni, Rajiv Limaye, Milind Kulkarni, ‘ intertrochanteric fractures- Current concept review’ Ind J Orth, 2006, vol 40, 16-23.
3.Boldin, Christia, Seibert, Franz J, Fankhauser, Wolfgang, Szyszkowitz, Rudolf (2003) et al. Acta Orthopaedics, 74:1, 53-58.
4.Wei-Chao Sheng, Jia-Zhen Li, Sheng-Hua Chen and Shi-Zen Zhong. International orthopaedics, vol 33, number 2, 537-42.
5.Patil Suresh S, Panghate Atul. J orthopaedics 2008, 5(3) E7.
6.Ganz R, Thomas R.J, Hammerle CP. Clin Orthop 1979; 138:30-40.
7.Cleveland, m. Bosworth, D. M and Thompson, F.R. JBJS, 29:1049-67, 1947.
8.Mulley G and Espley, A. J. Postgrad Med. J, 55:264-265, 1979.
9.Evans EM. JBJS 1949; 31B: 190-203
10.Wolfgang GL. Clinical Orthopaedics and related research 1982; 163: 148-158.
11.Sarmeinto, A. Clin.Orthop, 53:47-59, 1967.
(Abstract) (Full Text HTML) (Download PDF)
Definitive Management of Pelvic Fractures
/in Volume 3 | Issue 1 | Jan-April 2017Vol 3 | Issue 1 | Jan – Apr 2017 | page:17-23 | Vivek Trikha, Saubhik Das.
Author: Vivek Trikha [1], Saubhik Das [1]
[1] Department of Orthopaedics, AIIMS & JPNATC, New Delhi, India..Address of Correspondence:
Address of Correspondence
Dr. Vivek Trikha,
Department of Orthopaedics, AIIMS & JPNATC, New Delhi, India.
E-mail: vivektrikha@gmail.com
Abstract
Pelvic fractures constitute one of the most severe orthopedic injuries causing significant mortality and morbidity. It poses a diagnostic and therapeutic challenge to orthopedic surgeons. Once the patient is resuscitated and stabilized, definitive reconstruction of pelvic fracture is planned. Management depends on patient’s physiologic status, fracture characteristics, and associated injuries. Early fixation has proven to be beneficial. Our paper focuses on definitive management of pelvic fracture, with emphasis on surgical approach, fixation methods and principles.
Keywords: Complication, definitive management, functional outcome, pelvic fracture.
Introduction
Pelvic fractures constitute one of the most severe orthopaedic injuries causing significant mortality and morbidity. Pelvic fractures can either be stable fractures resulting from low energy trauma, for example iliac wing or isolated ramus fractures, or more importantly, unstable fractures from high energy injury. Most of these results from road traffic accidents, falls from height, or occasionally, work place crushing accidents, and are often associated with other injuries like injuries of the abdomen or pelvic viscera, urogenital injuries, neurovascular injuries in the pelvis retroperitoneal region and other lower limb fractures. Once patient is optimised and fully resuscitated with haemorrhage control and temporary pelvic stabilisation, definitive surgical fixation is contemplated to address pelvic instability and improve long term outcomes. Surgical decision making is a complex process and challenging even to the most experienced orthopaedic surgeons.
Classification
There are various classifications proposed for the pelvis fracture like Tile’s, Young- Burgess and AO/OTA Classification. The classification described by Young and Burgess is widely followed [1]. It reflects the mechanism of injury as well as the degree of injury. Based on mechanism, pelvic fractures are classified into four types- anteroposterior compression (APC), lateral compression (LC), vertical shear (VS) and combined type in this classification
1) Antero-posterior compression (APC, Fig-1A):
Antero-posterior direct compression force leads to diastasis of the symphysis pubis or vertical rami fractures anteriorly. In type I injury, diastasis of pubic symphysis is typically <2.5cmand posterior pelvic ligaments (anterior and posterior sacroiliac, sacrotuberous, and sacrospinous) are intact. With greater force, injuries progress to APC type II, which is characterised by the symphyseal diastasis>2.5cm, with anterior opening of sacroiliac(SI) joint. There is disruption of anterior sacroiliac (SI), sacrotuberous(ST), and sacrospinous(SSp) ligaments; however the posterior SI ligaments remain intact. With still greater force, there is complete disruption of anterior and posterior SI ligaments, producing unstable SI joint and APC type III pattern.
2) Lateral compression (LC, Fig-1B):
Lateral compression injuries are the most frequently encountered pattern. They result from side impact during motor vehicle collision or fall from height. Anterior injury typically demonstrates transverse pubic rami fractures. In LC type I injuries, there is sacral impaction fracture posteriorly. LC type II pattern has iliac wing or crescent fracture posteriorly. LC type III injuries (‘windswept pelvis’) are characterised by composite injury of LC I or LC II on side of impact, with contralateral open book (APC) injury.
3) Vertical Shear (VS, Fig-1C):
A vertically directed force results in disruption of both anterior and posterior elements, with vertical displacement of one hemipelvis with respect to the other. A fracture of the transverse process of L5 vertebra is often a tell-tale sign of such an injury.
4) Combined:
A combination of the above mechanisms of injury is classified as “combined” pattern. It usually involves the LC and the VS pattern of injury.
Definitive management
Definitive management of pelvic fractures is contemplated after patient is optimised and conducive for surgical intervention. Pelvic radiographs (anteroposterior, inlet, outlet view), CT scan with 3D reconstruction are carefully evaluated to define fracture configurations. Dynamic stress view is often sought for elucidation of occult instability.
Some basic tenets of pelvic fracture management are
1. Integrity of posterior pelvic ring is most critical for overall pelvic stability.
2. If there is disruption of posterior pelvic ring (sacral fracture, SI joint disruption, iliac wing or crescent fractures), with vertical instability of hemipelvis, posterior fixation should ideally be augmented by some form of anterior fixation (ORIF/ external fixator) to restore stability [2].
3. Classically, fixation should proceed from posterior to anterior [3]. However, controversy surrounds this approach, with some advocating front first approach [4].
Indications for surgery
APC type I fracture is generally stable pattern (symphyseal widening< 2.5 cm), and usually treated nonoperatively with good results. Caution must be exercised to differentiate APC type I injury from APC type II injury. If concern exists, dynamic stress view and/or examination under anaesthesia must be performed to elucidate occult instability which necessitates fixation. Similarly, LC type I fractures are usually treated nonoperatively. Whereas, APC and LC type II and III fractures are rotationally unstable,which require surgical stabilisation. In vertical shear (VS) injury, there is complete disruption of ligamentous support with cephalad migration of hemipelvis. Surgical stabilisation is required in all VS injuries.
Tworare LC variants deserve special mention; locked symphysis and tilt fracture [5]. During lateral compression, intact pubis can cross midline and get entrapped into the obturator foramen. If closed reduction is unsuccessful and pelvic instability persists, open reduction and stabilisation is necessary. Similarly in tilt fracture, superior ramus is pushed posteriorly and inferiorly into the perineum. This can lead to dyspareunia in female patients. Surgical management is often considered to reduce this fracture and avoid later dyspareunia.
Timing for definitive fixation
Optimal time frame for definitive surgical stabilisation has not been clearly defined. There is recent trend towards acute surgical stabilisation; time frame varies in literature from as early as less than 24 hours to less than one week after injury [6, 7].Our preference is to fix most of the fractures within the first one week after injury once patient is optimised, albeit early fixation is associated with risk of bleeding and potential for second hit in multiply injured patients.Proponents for early fixation cites several advantages; improved fracture reduction, early mobilisation and pain relief, less risk of pulmonary complication and deep vein thrombosis, shorter hospital stay [7]. However, treatment should be individualised and several factors should be kept in mind to decide optimal time for surgery such as; patient’s haemodynamic status and co morbidities, associated injuries, and soft tissue condition etc.
Option for surgical fixation and approach for anterior pelvic ring
1. External fixation:External fixator has proved to be a valuable tool for emergent as well as definitive management of pelvic fractures. This device usually is employed during:
1. As a temporizing measure during Emergent stabilisation of unstable pelvic injury in haemodynamically unstable patient.
2. As a definitive method of fixation of anterior pelvic ring when internal fixation is precluded (extraperitoneal bladder rupture, or when open laparotomy wound poses potential risk of infection of internal fixation).
3. Occasionally as a supplemental fixation following posterior pelvic ring stabilisation.
Various external fixator configurations have been described for the traditional anterior external fixator. Although they are equally effective in resisting rotational forces, none of these fixators are sufficient enough to stabilise vertically unstable pelvis [8]. Moreover, anterior frame require intact posterior hinge to close and stabilise pubic diastasis.
Two sites for pin placement for anterior external fixator have been described; into the iliac crest (Fig. 2-A), and into the dense supraacetabular bone (Fig. 2-B). Compared to iliac crest pins, supraacetabular pin placement requires precise technique and fluoroscopic guidance. Pins are directed from anteroinferior iliac spine (AIIS) towards sciatic buttress. Starting point and interosseous path of screw between inner and outer table of pelvis is obtained by obturator oblique outlet view. Additionally, iliac oblique inlet view demonstrates trajectory of screw over greater sciatic notch and hip joint towards sciatic buttress. Recently internal external fixator using pedicle screws in place of supraacetabular pins(INFIX) [9], andplate internal fixator [10] have been described. Better biomechanical advantage and avoidance of pin site complications are potential advantages of these techniques.
2.Internal fixation
Pfannenstiel approach is the mainstay for internal fixation of anterior pelvic ring (Fig. 3). Transverse incision is placed twofingerbreadths above symphysis pubis. Usually longitudinal incision is made into linea alba. Very often, rectus abdominis is torn off at least on one side, this allow easy access without disturbing rectus insertion much. Sometimes fixation of rami fracture is considered especially in rotationally and/ or vertically unstable pelvic injury with significant soft tissue damage, as an adjunct to posterior fixation. In most of the cases, rami fractures can be treated nonoperatively, as intact periosteal hinge and inguinal ligament provide favourable biological and mechanical environment for healing. Options for internal fixation of rami fractures include; ORIF with plating, percutaneous screw(antegrade or retrograde). For ORIF of rami factures, Pfannenstiel incision is used and subperiosteal dissection is carried further laterally up to pelvic brim, or formal Stoppa’s approach can be performed. Caution should be taken to avoid injury to corona mortis (anastomosis between external iliac and obturator vessels), which should be protected and ligated.To avoid extensive surgical dissection, many surgeons are adopting percutaneous fixation with antegrade or retrograde screw (Fig. 4). Biomechanically retrograde ramus screw is found to be as effective as plating. Screw position and technique largely depends upon fracture configuration, location, associated soft tissue injury, and body habitus of patient. In general, antegrade screw (from supra-acetabular area and directed medially towards symphysis pubis) is used for rami fractures located in middle or lateral third, and in obese patient. Whereas retrograde screw (from pubic tubercle and directed laterally above the acetabulum) is preferred for medially based fractures [11]. Surgeon well versed with this technique and proper fluoroscopic view is paramount for accurate screw placement. Complications most often arise due to improper trajectory of screw leading to injury to adjacent structure such as; external iliac vasculature, corona mortis, bladder, urethra, and penetration into hip joint.
Option for surgical fixation and approach for posterior pelvic ring:
1. Percutaneous iliosacral screw:
Percutaneous iliosacral screw is increasingly being used for SI joint dislocation as well as some sacral fractures. Minimally invasive nature, and equivalent biomechanical properties compared to transiliac fixation and anterior SI plating, has led to the popularity of this method [12]. Well trained pelvic surgeon with in depth knowledge and orientation of anatomic as well as radiographic landmarks, is critical for proper execution of the procedure. Inlet, outlet and lateral sacral radiographic view is paramount to ensure safe trajectory of screw. Safe corridor for screw placement is marked by identification of radiographic landmarks such as; iliac cortical density corresponding to sacral ala on which L5 nerve rests, anterior cortex of sacral promontory where great vessels lie, posterior border of S1 corresponding to anterior aspect of sacral canal, S1 foramen. Detailed evaluation of preoperative x ray and CT scan with 3D reconstruction is paramount to identify sacral dysmorphism and spinal abnormalities, if any, that could alter placement of screw to avoid inadvertent injury to nearby structures. Recently, computer navigation and 3D imaging have been found useful for this procedure [13].
2. Open reduction and fixation:
SI joint dislocation requiring open reduction can be accessed through posterior or anterior approach. For posterior approach, patient is positioned prone on radiolucent table and paramedian incision is used. Clamp placement is easier from posterior approach. However, direct visualisation of fracture reduction is difficult. Palpation of anterior SI joint through greater sciatic notch helps to ensure anatomic reduction. Fixation options include percutaneous iliosacral screw, iliac bars, tension band plating. For SI joint dislocation requiring anterior approach, lateral window of ilioinguinal approach is employed. Fixation is achieved by anterior SI plating, percutaneous iliosacral screw, or combination of both; no biomechanical differences has been found between these. Due to proximity of L5 nerve over sacral ala, only one hole of the plate can be placed safely over sacral ala. Therefore two plates at an angle of less than 90° to each other are necessary to gain control of injured SI joint. Safe placement of reduction clamp and fixation device is imperative to avoid injury to L5 nerve.
For iliac wing fracture, anterior or posterior approach is used, whichever is deemed necessary. Two plates are generally required to neutralise deforming forces; one along iliac crest and pelvic brim (anterior approach), and sciatic buttress along with iliac crest (posterior approach). Additionally, lag screw along the crest can be employed to achieve compression.
Management of specific injury pattern:
1. Antero-posterior compression(APC) injury:
Rotationally unstable APC type II and III injuries necessitate surgical stabilisation. After exposure through Pfannenstiel type incision, there are several methods to achieve and maintain reduction. Internal rotation and taping of lower extremities along with Weber reduction clamp with its tines placed on each pubic tubercle can assist in reduction. Additionally, Farabeuf or Jungbluth clamp, which utilizes 3.5 or 4.5 mm screws, also assist in reduction. They are particularly useful to correct associated sagittal rotation (flexion/extension), and posterior translation of hemipelvis, often associated with posterior ring injury. Controversy surrounds concerning the plate configuration for symphyseal diastasis. Previously two hole plate have been advocated, which theoretically maintain physiologic motion at symphysis pubis. However, high failure and malunion rate with two hole construct prompted pelvic surgeons to use multi-hole construct with at least 2 point of fixation on either side of symphysis [14]. Our preference is to use multi-hole 3.5 mm symphyseal specific or pelvic reconstruction plate with at least 2 point of nonlocking fixation on either side (Fig. 3). Although locking plate could be beneficial in osteoporotic bone, their superiority over non-locked device is questionable [15]. Proper screw trajectory should be maintained to avoid inadvertent injury to bladder, which can be ascertained by finger palpation of posterior aspect of pubis.
In APC type II injury, need for posterior fixation is a point of debate. A recent literature tried to address this issue bysub classifying APC type II injury. In type IIa subtype, posterior sacroiliac (SI) ligaments are intact, and anterior fixation alone is sufficient. In type IIb subtype, posterior SI ligaments are attenuated (not disrupted), which contribute to the sagittal plane instability of hemipelvis. On dynamic stress view, sagittal plane displacement of hemipelvis > 1 cm signifies unstable injury, and necessitates supplemental posterior fixation via iliosacral screw [16]. Both anterior and posterior stabilisation is deemed necessary for APC type III injury (Fig. 5). Controversy exists regarding sequence of fixation. Posterior ringstabilisation followed by anterior ring is the classically described method of fixation. However, many authors have reported favourable outcome with the reverse sequence progressing anterior to posterior [4, 17]. It is imperative to keep in mind that proper reduction of anterior ring is paramount to gain control and anatomic restoration of posterior ring in this method.
2. Lateral compression (LC) injury:
LC type II injury involves either fracture through entire ilium, or crescent fracture posteriorly, associated with anterior rami fractures. In crescent fractures, the fracture goes through the iliac wing and into the SI joint with substantial disruption of SI joint ligament complex, yielding rotationally unstable hemipelvis [18]. The crescent fragment comprising Postero superior iliac spine (PSIS) and Postero inferior iliac spine (PIIS) remains attached to sacrum by posterior and interosseous SI ligaments. Surgical management is deemed necessary for this uncommon injury. Day et al. [19]proposed a functional classification of crescent fracture and suggested management algorithm, which can aid surgeons in deciding appropriate treatment. Type I fracture involves large crescent fragment with fracture line involving anterior third of SI joint. This can be addressed by lateral window of ilioinguinal approach with plate fixation. Type II fracture comprising intermediate size fragment with fracture line exiting through mid third of SI joint, can be addressed by posterior approach. Fixation by lag screw from PIIS towards sciatic buttress, parallel to SI joint, with supplemental plate fixation yield stable construct. Type III fracture involve most but not all of the SI joint with fracture line exiting through posterior part of SI joint. Crescent fragment is small in size. This is amenable to closed reduction with percutaneous iliosacral screw fixation. In case of delayed presentation with unsuccessful closed reduction, anterior approach with plate fixation can be considered.
LC type III injury with ‘windswept’ pelvis can be managed in line of APC and LC injury in combination. Evaluation of fracture configuration and instability pattern can aid in deciding systematic management strategy.
3. Vertical shear(VS) injury and sacral fracture:
VS injuries are very unstable pattern. If posterior component is pure SI joint dislocation, then anatomic reduction and iliosacral screw fixation is performed. Anterior fixation should be performed as an adjunct to posterior fixation to neutralise potential deforming forces (Fig. 6).
Concern arises regarding inadequate screw purchase in transforaminal, comminuted sacral fractures. Transsacral fixation with partially or fully treaded screw has proved to be beneficial demonstrating favourable results, especially with use of locking nuts [20]. Other fixation options include iliac bar, transsacral plating, spino-pelvic construct (Fig. 7 and 8). Substantial vertical instability with comminuted sacral fracture, spino-pelvic dissociation, disruption of L5-S1 facets, and late cases of VS injury with sacral fracture can be addressed by spino-pelvic fixation. Triangular osteosynthesis refers to spino-pelvic fixation combined with iliosacral screw [21].Literature supports superior biomechanical properties of these constructs compared to iliosacral screw (Fig. 8) [22].
4. Open pelvic injury:
If the pelvic fracture has a direct communication with the outside environment it is open in nature. It may communicate to the skin from the abdomen, scrotum, buttock or back, rectum or vagina. Its incidence is less than 5% of all pelvic injuries however, the mortality figures range from 5-45%, generally around 25%. Compounding, internal or external, worsens the prognosis [23]. This injury is the result of a very high energy impact and invariably has associated injuries. Any external wound on the lower abdomen, pelvis, scrotum or the genital region should be considered to be communicating with the pelvis injury until proven otherwise. Open fractures require provisional pelvic stabilisation with fixator, thorough wound debridement, and suprapubic catheterisation or diversion colostomy. A multidisciplinary approach is warranted, and communication with concerned specialities is paramount in placing diverting colostomy and suprapubic catheter as far as possible from planned surgical site to avoid potential contamination of internal fixation.
A Morel-Lavallee lesion is an equally sinister injury pattern [24]. It is described as an internal degloving injury around the hip when the skin and the subcutaneous tissues are traumatically separated from the underlying muscle fascia, fatty and soft tissue. A sizable amount of fluid may collect in the closed space which is characteristic of this lesion. It might be missed and the fracture treated as a closed injury with disastrous consequences. It needs a thorough open debridement with external fixation or percutaneous drainage in acute stage. Percutaneous fixation, if possible, can be done. Vacuum assisted closure has a role in the management of such wounds [25]. In such cases external fixation forms the mainstay of treatment initially, which may be converted to definitive stabilization once the soft tissue stabilizes.
Complications and Outcome:
In an analysis of more than 63 thousand patients, the odds ratio for mortality associated with a pelvic fracture was found to be 2.0, which were similar to that for an abdominal injury [26].Haemorrhage and closed head injury constitute the two most common causes of early mortality. Sepsis and multi organ failure are the major causes of late mortality. Besides the early and late mortality, pelvis fractures are also associated with late morbidity. The stable fractures usually do well and cause minimal disability while the unstable fractures have a higher rate of deformity and disability.
Pain is an important cause of morbidity after pelvic fractures. Its incidence is highest in patients with unstable pelvic injury and major pelvic disruptions. If the major weight bearing arch of pelvis i.e., the posterior pelvic element is displaced and not reduced, it may lead to malunion, non-union or osteoarthritis of the SI joint. This may cause disabling pelvic pain which is most common with combined or vertical shear type of fracture. It has been postulated that if the residual displacement is more than 1 cm, nearly 70% of patients shall have severe pain with abnormal function. Neurological injury is most common after unstable vertical shear fractures, posterior pelvic injuries and Denis type III sacral fractures. Careful evaluation and documentation is essential to look for the sensory deficits around perineum and sphincter function.
The incidence of genitourinary injury in pelvic fractures has been reported to be 4.6%. It is twice as common in males as in females. Patients with genitourinary injury have greater ICU stay and increased mortality rates as compared to those without genitourinary injury [27]. Posterior pelvic injuries are involved in the ejaculatory disturbances while the anterior injuries, especially the diastasis, cause the erectile dysfunctions. In females also, dyspareunia is common after diastasis or rami fractures.
Evaluation of outcome following pelvic fracture fixation is difficult to assess because of diversity of fracture pattern and treatment options, associated injuries, and lack of validated outcome measures. Literature unveils that posterior ring stabilisation with less than 1 cm of displacementproduces favourable long term outcome, especially in pure SI joint dislocation [28, 29]. Moreover bony injury of posterior ring is thought to do better as compared to ligamentous disruption, because of bone to bone healing is believed to restore strength and stability [30].However, there is no reference standard in literature what constitutes an accurate reduction, which is supported by the fact that despite near normal anatomic reduction, substantial proportions of patients continue to have chronic pelvic pain and some persistent impairment in longterm [31-34].A recent prospective observational study concluded that Two years after surgical treatment of pelvic ring fractures, patients reported substantially lower quality of life for both physical and mental domains, when compared with a reference population, even when radiological and clinical outcomes were considered favourable [35].
Conclusion
Pelvic fracture management is a complex decision making process which poses a therapeutic challenge to even most experienced orthopaedic surgeons. APC and LC type I injuries are successfully treated nonoperatively. Whereas APC and LC type II and III injuries require operative treatment with anterior and/or posterior fixation depending on fracture geometry and instability pattern. VS injuries are most unstable pattern requiring operative stabilisation. In general, anatomic restoration of posterior pelvic ring is paramount, which often is supplemented by anterior fixation to yield stable pelvic construct. Open pelvic fractures necessitate multidisciplinary approach with expeditious wound management, provisional pelvic stabilisation.
References
1. Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions:effective classification system and treatment protocols. J Trauma1990;30:848–56.
2. Stocks GW, Gabel GT, Noble PC, et al. Anterior and posterior internal fixation of vertical shear fractures of the pelvis. J Orthop Res. 1991;9:237–245.
3. Lefaivre KA, Starr AJ, Reinert CM. Reduction of displaced pelvic ring disruptions using a pelvic reduction frame. J Orthop Trauma. 2009;23:299–308.
4. Krappinger D, Larndorfer R, Struve P, et al. Minimally invasive transiliac plate osteosynthesis for type C injuries of the pelvic ring: A clinical and radiological follow-up. J Orthop Trauma. 2007;21:595–602.
5. Langford JR1, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 2. Contemporary indications and techniques for definitive surgical management.J Am Acad Orthop Surg. 2013 Aug;21(8):458-68.
6. Connor GS, McGwin Jr G, Maclennan PA, Alonso JE, Rue 3rd LW. Early versus delayed fixation of pelvic ring fractures. Am Surg. 2003; 69(12): 1019-1023 (discussion 1023-4).
7. Vallier HA, Cureton BA, Ekstein C, Oldenburg FP, Wilber JH. Early definitive stabilization of unstable pelvis and acetabulum fractures reduces morbidity. J Trauma. 2010;69 (3):677–684.
8. Tile M. Acute pelvic fractures: II. Principles of management. J Am Acad Orthop Surg. 1996;4(3):152–161.
9. Vaidya R, Colen R, Vigdorchik J, Tonnos F, Sethi A: Treatment of unstable pelvic ring injuries with an internal anterior fixator and posterior fixation: Initial clinical series. J Orthop Trauma 2012;26(1):1-8.
10. Cole PA, Gauger EM, Anavian J, Ly TV, Morgan RA, Heddings AA: Anterior pelvic external fixator versus subcutaneous internal fixator in the treatment of anterior ring pelvic fractures. J Orthop Trauma 2012;26(5): 269-277.
11. Starr AJ, Nakatani T, Reinert CM, et al. Superior pubic ramus fractures fixed withpercutaneous screws: What predicts fixation failure? J Orthop Trauma. 2008;22:81–87.
12. Yinger K, Scalise J, Olsen SA, et al. Biomechanical comparison of posterior pelvic ring fixation. J Orthop Trauma. 2003;17:481–487.
13. Zwingmann J, Konrad G, Mehlhorn AT, et al. Percutaneous iliosacral screw insertion: Malpositioning and revision rate of screws with regards to application technique (navigated vs. conventional). J Trauma. 2010;69:1501–1506.
14. Sagi HC, Papp S. Comparative and clinical and radiographic outcome of two-hole and multi-hole symphyseal plating. J Orthop Trauma. 2008 Jul; 22(6): 373-8.
15. Grimshaw CS, Bledsoe JG, Moed BR. Locked versus standard unlocked plating of the pubic symphysis: A cadaver biomechanical study. J Orthop Trauma. 2012;26:402-06.
16. Sagi HC, Coniglione FM, Stanford JH: Examination under anesthetic for occult pelvic ring instability. J Orthop Trauma 2011;25(9):529-536.
17. Mullis BH, Sagi HC: Minimum 1-year follow-up for patients with vertical shear sacroiliac joint dislocations treated with iliosacral screws: Does joint ankylosis or anatomic reduction contribute to functional outcome? J Orthop Trauma;22(5):293-298.
18. Borrelli J Jr, Koval KJ, Helfet DL: Operative stabilization of fracture dislocations of the sacroiliac joint. Clin Orthop Relat Res 1996;329:141-146.
19. Day AC, Kinmont C, Bircher MD, Kumar S: Crescent fracture-dislocation of the sacroiliac joint: A functional classification. J Bone Joint Surg Br 2007;89(5):651-658.
20. Tabaie SA, Bledsoe JG, Moed BR:Biomechanical comparison of standardiliosacral screw fixation to transsacrallocked screw fixation in a Type C – ZoneII pelvic fracture model.J Orthop Trauma. 2013 Sep;27(9):521-6.
21. Sagi HC: Technical aspects and recommended treatment algorithms in triangular osteosynthesis and Spinopelvic fixation for vertical shear transforaminal sacral fractures. J Orthop Trauma 2009; 23(5):354-360.
22. Schildhauer TA, Ledoux WR, Chapman JR, Henley MB, Tencer AF, Routt ML Jr: Triangular osteosynthesis and iliosacral screw fixation for unstable sacral fractures: A cadaveric and biomechanical evaluation under cyclic loads. J Orthop Trauma 2003;17(1):22- 31.
23. Brenneman FD, Katyal D, Boulanger BR, Tile M, Redelmeier DA. Longterm
outcomes in open pelvic fractures. J Trauma 1997;42:773–7.
24. Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallée lesion. J Trauma 1997;42:1046–51.
25. Labler L, Trentz O. The use of vacuum assisted closure (VAC) in soft tissue injuries after high energy pelvic trauma. Langenbecks Arch Surg 2007;392:601–9.
26. Sathy AK, Starr AJ, Smith WR, et al. The effect of pelvic fracture on mortality after trauma: an analysis of 63,000 trauma patients. J Bone Joint Surg Am 2009;91:2803–10.
27. Bjurlin MA, Fantus RJ, Mellett MM, Goble SM. Genitourinary injuries in pelvic fracture morbidity and mortality using the National Trauma Data Bank. J Trauma 2009;67:1033–9.
28. Dujardin FH, Hossenbaccus M, Duparc F, et al. Long-term functional prognosis of posterior injuries in high-energy pelvic disruption. J Orthop Trauma. 1998;12:145–150.
29. Hoffman MF, Jones CB, Sietsma DL. Persistent impairment after surgically treated lateral compression pelvic injury. Clin Orthop Relat Res. 2012Aug; 470(8): 2161-72.
30. Cole JD, Blum DA, Ansel LJ. Outcome after fixation of unstable posterior pelvic ringinjuries. Clin Orthop Relat Res. 1996;329:160–179.
31. Oliver CW, Twaddle B, Agel J, Routt ML Jr. Outcome after pelvic ring fractures: evaluation using the medical outcomes short form SF-36. Injury 1996;27:635– 41.
32. Pohlemann T, Gansslen A, Schellwald O, et al. Outcome after pelvicring injuries. Injury 1996;27(suppl 2):B31– 8.
33. Van den Bosch EW, Van der Kleyn, Hogervorst M, et al. Functional outcome of internal fixation for pelvic ring fractures. J Trauma. 1999;47:365–371.
34. Kabak S, Halici M, Tuncel M, et al. Functional outcome of open reduction and internal fixation for completely unstable pelvic ring fractures (type C): A report of 40 cases. J Orthop Trauma. 2003;17:555–562.
35. Borg T, Berg P, Fugl-Meyer K, Larsson S: Health-related quality of life and life satisfaction in patients following surgically treated pelvic ring fractures: A prospective observational study with two years follow-up. Injury 2010;41(4):400-404.
.
(Abstract) (Full Text HTML) (Download PDF)
Iliofemoral Approach to Acetabulum
/in Volume 3 | Issue 1 | Jan-April 2017Vol 3 | Issue 1 | Jan – Apr 2017 | page:14-16 | Ravi Gupta, Ashwani Soni
Author: Ravi Gupta [1], Ashwani Soni [1]
[1] Department of Orthopaedics Government Medical College Hospital, Chandigarh 160031India.
Address of Correspondence
Dr Ravi Gupta
Department of Orthopaedics
Government Medical College Hospital, Chandigarh 160031
Email: ravikgupta@yahoo.com
Abstract
Surgical approach to acetabulum fractures depend on the type of fracture and fracture displacement along with surgical preference of the surgeon. Ilio-femoral approach is one of the most important approaches for acetabular fractures. It allows access to anterior column as well as anterior wall fractures. This symposium article details the surgical technique as well as indications and shortcomings of this approach.
Keywords: Ilio-femoral appraoch, acetabulum fractures, anterior column fractures.
Introduction
Operative reduction and fixation is considered as accepted treatment method for displaced acetabular fractures now days. Surgical approach to acetabulum may be anterior (ilioin-guinal, ilio-femoral, Stoppa approach [1,2]), posterior (Kocher-Langenbeck approach and variants [3]) or combined (simultaneous or different sittings) [4]. The choice of approach depends on the type of fracture, displacement and the surgeon’s preference [5].
Ilio-femoral approach provides wide access to the entire internal iliac fossa including visualization of the anterior aspect of the sacroiliac joint. This approach also provides digital and some visual access to the quadrilateral surface and greater sciatic notch. Medially, along the anterior column this approach provides access up to iliopectenial eminence.
Combined with Kocher-Langenbeck approach, anterior column component of T-type fracture can be fixed by this approach. When combined with pfannenstiel approach for symphysis pubis, almost all types of anterior column and anterior wall fractures can be addressed by this approach.
Surgical approach to acetabulum fractures depend on the type of fracture and fracture displacement along with surgical preference of the surgeon. Ilio-femoral approach is one of the most important approaches for acetabular fractures. It allows access to anterior column as well as anterior wall fractures. This symposium article details the surgical technique as well as indications and shortcomings of this approach
Anterior column fractures where main displacement is cephalad to the joint are the best candidates for this approach. Associated anterior + posterior hemitransverse fractures are also addressed by this approach.
Skin incision
Skin incision begins proximally posterior to the gluteus medius pillar, runs parallel to the iliac crest to the anterior superior iliac spine and then extend distally between sartoreus and tensor muscle. In modification to this approach, the dissection stops the anterior extent of proximal limb of skin incision 1-2 cm lateral to the anterior superior iliac spine and then extends distally and laterally directly over the anterior aspect of the tensor muscle belly. This reduces the damage to lateral cutaneous nerve and prevent to some extent the skin problems at the junction of two limbs of incision. Position of the proximal limb of incision need to be modified according to the body habitus of patient as scar directly over the iliac crest in a thin patient can be problematic.
Superficial dissection
Deeper dissection is done through subcutaneous tissue. External oblique muscle is released from the iliac crest leaving thick fascio/periosteal cuff for subsequent repair at the time of closure. This release of muscle is started posteriorly where it overhangs the iliac crest and extends anteriorly to the level of planned anterior superior iliac spine osteotomy or sartorius/ inguinal ligament release. Internal iliac fossa is exposed by lifting the iliac muscle subperiosteally and packed with sponge.
Osteotomy of ASIS
Osteotomy of ASIS is done with block measuring 2 cm in depth and 2 cm in anteroposterior diameter. Tensor attachment to this bony block is released. This osteotomised bone block along with its attachments of iliacus, external oblique, Sartorius, and inguinal ligamanet is displaced medially.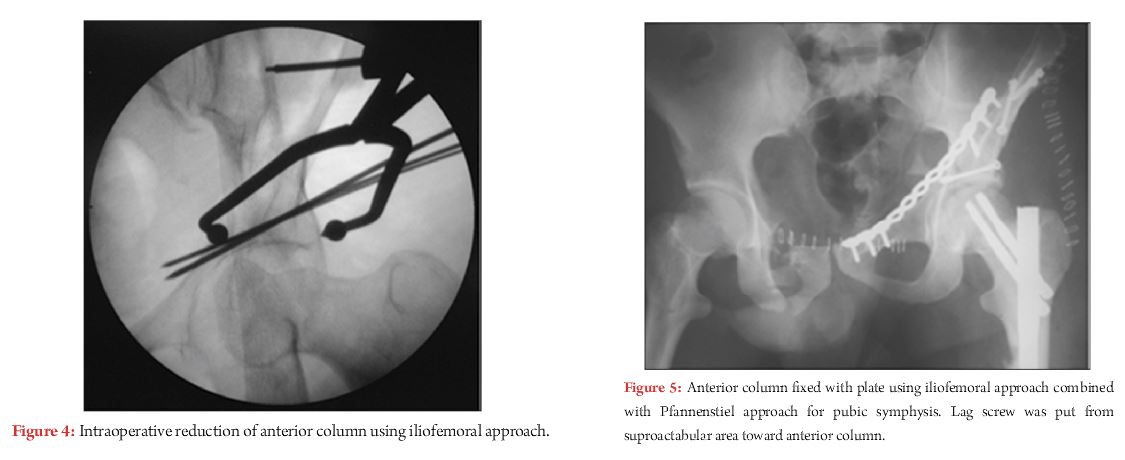
This osteotomy is not possible in cases where fracture line reaches to the area of osteotomy. In these cases Sartorius and inguinal ligament is released from ASIS as a single cuff of tissue.
Tensor-sartorius interval is identified and fascia of thigh is incised over tensor muscle belly starting 1-2 cm lateral to the ASIS. The tensor muscle is retracted laterally and the medial sheath of the tensor fascia is retracted medially protecting the lateral femoral cutaneous nerve. Subsequently the dissection is done through the floor of tensor sheath and the proximal and distal exposures and joined. Approximately 10 cm from the ASIS the ascending branches of the lateral femoral circumflex artery and vein are encountered under the aponeurotic fascial layer over the rectus femoris muscle which needs to be identified and ligated in case if wide exposure is required. True pelvis is accessed by releasing iliopectineal fascia from the pelvic brim starting just anterior to the SI joint and extending anteriorly to the level of the pubic root. subperiosteal elevation of the obturator internus from the quadrilateral surface can provide further access to pelvis.
At this stage entire iliac fossa and anterior sacroiliac joint is accessible. Quadrilateral lateral plate and greater sciatic notch is approached to certain extent either by direct visualisation or digital palpation. By retracting iliopsoas muscle medially, after relaxing it by doing flexion and adduction at hip joint; the exposure can be extended medially up to iliopectenial eminence.
Further access to anterior column, medial to iliopectineal eminence can be gained through a separate pfannenstiel incision for pubic symphysis. By doing this almost all types of fractures of anterior column can be addressed.
Corona mortise is an anastomosis behind the pubic symphysis between the obturator and external iliac arteries. By approaching medial most part of anterior column through pfannenstiel incision this anastomoses should be identified and ligated if present otherwise this anastamoses can be life threatening if injured.
Closure:
After placing the drain osteotomy of ASIS is fixed with 2.7 or 3.5 mm lag screws. External iliac muscle is sutured to iliac crest by fascial/periosteal repair. Fascial repair is done at distal limb of wound followed by subcutenous and skin closure.
.
(Abstract) (Full Text HTML) (Download PDF)
Where Do We Need More than One Approach for Acetabular Fractures and Which One First?
/in Volume 3 | Issue 1 | Jan-April 2017Vol 3 | Issue 1 | Jan – Apr 2017 | page:10-13 | Raju Vaishya, Vipul Vijay, Amit K Agarwal, Abhishek Vaish
Author: Raju Vaishya [1], Vipul Vijay [1], Amit K Agarwal [1], Abhishek Vaish [2]
[1] Department of Orthopaedics and Joint Replacement Surgery, Indraprastha Apollo Hospitals, New Delhi, India,
[2] Department of Orthopaedics, Canterbury Christ Church University, Kent, UK.
Address of Correspondence
Dr. Raju Vaishya,
Indraprastha Apollo Hospitals, New Delhi, India.
E-mail: raju.vaishya@gmail.com
Abstract
Acetabular fractures are often difficult to manage. The majority of fractures require anatomical reduction to prevent secondary
osteoarthritis and instability. Often a single approach is sufficient to fix these fractures. The choice of approach depends on the
major anatomical involvement of the acetabulum. However, some fracture patterns require more than a single approach to fixing the
fractured fragments adequately. This article addresses this particular issue.
Keywords: Acetabulum, fractures, pelvic, surgical approaches.
What to Learn from this Article?
The fixation of all the acetabular fractures cannot be achieved with a single approach, at all the times. Hence, it is necessary to do a good pre-operative planning and identify the fractures which may require a dual approach to achieve satisfactory fixation.
Introduction
The iPhone App Store was launched in July 2008 and was followed by the Google Play store in 2012. The above ones are the most popular mobile operating sys-tem in the world till date. The mobile apps have changed our lives and the way we com-municate with each other and go about doing things. So is the world of Medical and Orthopaedic Apps which have been on the forefront since last few years.
Here we present you a series of review of few Medical Apps which we regularly use and make a difference in our lives and the way we practice Orthopaedics and increase productivity.
Review
The basic fracture fixation principles in the lower extremity are anatomical reduction and the possibility of early rehabilitation. A combination of these two factors can help one achieve good prognosis and outcomes. The acetabular fractures are no different. They should be managed aggressively, and an attempt should be made to achieve anatomical reduction so as to prevent the most common complication of osteoarthritis (1). There are some restrictions on the surgical management of acetabulum fractures which may influence the decision of the treating surgeon towards an operative or conservative treatment. Factors like the proximity to important anatomical structures, the difficulty in achieving surgical exposure and the lack of experience in managing these fractures, all influence the decision-making (1).
With advances in imaging technology, a better understanding of anatomy and improved approaches for the management of the acetabulum fractures; focus is shifting towards an effort to achieve anatomical reduction (2). The first step in achieving anatomical reduction for any fracture is good surgical exposure. The most commonly used approaches are the Kocher Langenback and ilioinguinal approach, which have been the workhorse for acetabular surgeons. Recently, further modifications and some extensile approaches like iliofemoral, Stoppa’s, trochanteric osteotomy, etc have also been introduced (3-8). The type and combination of the surgical approach to be used is of paramount importance in achieving a good outcome.
Limitations of a Single Approach
The first step is to understand the anatomy, displacement and the direction of displacement of the fracture. The second step is to plan an approach which would allow proper visualization and accurate reduction of the fracture fragments (2). The ilioinguinal approach is useful for fixation of the anterior column and wall fractures, but they are unable to help in achieving an accurate reduction in cases of displaced posterior column fractures (1) (Figure 1). Similarly, the Kocher-Langenback approach can be used for good visualization of the posterior column and wall fractures, but they provide inadequate exposure to the anterior column and wall (1) (Figure 2).
Matta emphasized the need for anatomical reduction of the fracture fragments in acetabulum for optimal results (9). The key to anatomical reduction is good exposure and visualization of the fracture fragments. A single approach can adequately manage fractures involving a single column or wall. Also, certain bicolumnar fractures which have minimal displacement in one of the columns can also be managed by approaching the more displaced column directly.
However, in certain fractures like T-type fractures with significant displacement in both columns cannot be managed with a single approach. They require either the use of the described extensile approaches like iliofemoral, tri-radiate, etc. or the use of sequential approaches. These approaches are not without their sets of complications like increased rates of infection, delayed rehabilitation, higher rates of ectopic ossification and prolonged abductor weakness (2). Hence, whenever an extensile or a sequential approach is planned, the decision should be based on sound scientific judgement.
Fractures which can not be accessed through K-L approach alone
1. Both columns fractures
2. Anterior column fractures
3. Anterior column and posterior Hemi transverse fracture
Fractures which can not be accessed through ilioinguinal approach alone
1. T-type fractures
2. Isolated posterior column fractures
Fractures needing more than one approach
The fractures which may require more than one approach for an optimal result include –
1. T-type fractures
2. Selected both column fractures with significant displacement (>10mm) in both the columns.
3. Transtectal transverse fractures
4. Transverse fractures with posterior wall fracture with wide displacement
T-type and complete both column fractures
The T-type fractures and complete both column fractures need special mention. In these types of fractures, the femoral head is displaced medially, and both the columns rotate around the femoral head in opposite directions. This mechanism of rotation of the two columns can be understood as one similar to the two doors of a gate opening up in opposite direction around a central hinge. Any attempt at indirect reduction of the columns in these types of fractures will only lead to maintenance of the malrotation and the persistence of inaccurate reduction (1). These fractures are an absolute indication for open reduction, direct visualization, and internal fixation. Hence, these fractures may sometimes require the use of extensile approach or two sequential approaches for optimal fixation (2).
Transtectal fractures which have an anterior displacement also may require sequential approaches for fixation of these fractures. Some of the transtectal fractures may be fixed using a single anterior or posterior approach, especially if they have isolated posterior displacement. Some fractures with high anterior obliquity, on Judet views, with minimal displacement may also be fixed with an isolated posterior approach. Fractures with large displacement (>10 mm) in the anterior direction, usually need sequential surgical approaches (10).
In the transtectal fractures, the vertical nature of the fracture line makes it difficult to palpate the reduction through the greater sciatic notch (11). Moreover, since the fracture line passes through the supra-acetabular dome, imperfect reductions are very poorly tolerated (11). An adequate fixation may require in some of these fractures to utilize two approaches.
Transverse plus posterior wall fractures may make it difficult to be fixed through the isolated anterior approach. If approached through the K-L approach alone, the reduction of the transverse fractures may be difficult to assess through the posterior wall window, even after femoral head distraction. This may make it useful that the surgeon fixes the posterior wall using the K-L approach and then use the ilioinguinal approach for fixation and assessment of the transverse fracture reduction and fixation (1).
Decision making
The decision making for the choice of effective approach depends on the pre-operative CT scan (10). The first choice of fixation of the fractures mentioned is the Kocher-Langenback approach in preferably prone or lateral decubitus position. The pre-operative CT scan should be assessed and if there is a vertical fracture pattern or greater anterior displacement, then it would not be amenable to fixation through the isolated posterior approach but would require an additional anterior approach for optimal fixation (1,10).
Which approach first?
The decision of the first approach to be used depends on various factors. The amount of communication in one of the columns is one of the major determinants. The column which has a greater amount of communition should be fixed first. In the presence of a dislocation, the approach which gives direct access to the side of dislocation should be approached first. In case both the columns have equal comminution or are equally displaced, most of the surgeons prefer making the posterior approach first in the prone or the floppy lateral position (2). The anterior approach is made after making the patient supine.
The T-type fractures are a special case in the combined approach. It is often impossible to fix the posterior column through the K-L approach, without the screws passing through the anterior column fractures (11). Thus, the fractures of the anterior column must be reduced first, which makes the subsequent reduction of the posterior column and wall more amenable.
There have been some studies in the recent English literature, which have used the simultaneous anterior and the posterior approaches by two surgical teams (2). The advantages of simultaneous anterior and posterior approaches are decreased surgical time and simultaneous assessment of the reduction from anterior as well as the posterior directions. The disadvantages of this simultaneous approach are the requirement of two surgical teams which are equally adept and versed with acetabular fractures (2). Also, the anterior exposure is a bit difficult in the floppy lateral position, and the exposure is tough in obese patients (2).
Disadvantages
The disadvantages with the use of simultaneous or sequential approaches for acetabular fixation are –
1. Increased blood loss
2. Increased morbidity
3. Increased incidence of heterotopic ossification – due to increased soft tissue manipulation
4. Increased surgical time
Literature review
Combined exposures of the acetabulum have been used in the literature. Matta reported a very low incidence of 2% out of a total of 262 fractures operated (12). Letournel used a sequentially combined approach in only 3% of the cases, out of a total of 849 cases (3). Similarly, Mayo reported an incidence of 4% for combined approaches in their series of the acetabulum fractures (13).
The most important aim in acetabular fractures is anatomical reduction and adequate fixation. Even though all these studies emphasize that the number of fractures requiring more than one approach be limited, surgeon awareness is important so that an inaccurate reduction is not accepted. Adequate pre-operative planning using all the possible radiographic views and the CT scans available should be done, so that the surgeon is aware of the possibility of using two approaches based on the type of fracture and the displacement. This information can help the surgeon as well his team, including anaesthetists and assistants, be aware and prepared for the same.
The decision regarding whether the approach is made simultaneous or sequential and under the same or different anaesthesia, should be taken by surgeon expertise and OT backup. In most scenarios, the column with more comminution should be approached first and in the setting of equal comminution, the posterior column should be approached first.
References
1. Matta JM. Operative indications and choice of surgical approach for fractures of the acetabulum. Techniques Orthopaed 1986;1(1):13-22.
2. Harris AM, Althausen P, Kellam JF, Bosse MJ. Simultaneous anterior and posterior approaches for complex acetabular fractures. J Orthop Trauma. 2008 Aug;22(7):494-7.
3. Letournel E, Judet R, eds. Fractures of the Acetabulum. 2nd ed. Berlin, Germany: Springer-Verlag; 1993.
4. Mears DC, Rubash HE. Extensile exposures of the pelvis. Contemp Orthop. 1983;6:21–32.
5. Reinert CM, Bosse MJ, Poka A, et al. A modified extensile exposure for the treatment of complex or malunited acetabular fractures. J Bone Joint Surg. 1988;70A:329–337.
6. Routt ML Jr, Swiontkowski MF. Operative treatment of complex acetabular fractures. Combined anterior and posterior exposures during the same procedure. J Bone Joint Surg Am. 1990;72:897–904.
7. Griffin DB, BeaulA ˜ PE, Matta JM. Safety and efficacy of the extended iliofemoral approach in the treatment of complex fractures of the
acetabulum. J Bone Joint Surg Br. 2005;87:1391–1396.
8. Wey J, DiPasquale D, Levitt L, et al. Operative treatment of acetabular fractures through the extensile Henry approach. J Trauma. 1999;46: 255–260.
9. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients operatively treated within three weeks after injury. J Bone Joint Surg. 1996;78A:1632–1644.
10. Bogdan Y, Dwivedi S, Tornetta P 3rd. A surgical approach algorithm for transverse posterior wall fractures aids in reduction quality. Clin Orthop Relat Res. 2014 Nov;472(11):3338-44.
11. Bucholz RW, Heckman JD, Court-Brown C, eds. Rockwood Green’s Fractures in adults. 6th edn. New York, USA: Lipincott William & Wilkin’s;2006.
12. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients operatively treated within three weeks after injury. J Bone Joint Surg. 1996;78A:1632–1644.
13. Mayo KA. Open reduction and internal fixation of fractures of the acetabulum: results in 163 fractures. Clin Orthop. 1994;305:31–37.
.
(Abstract) (Full Text HTML) (Download PDF)