LICENSE
![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X

![]()
Creative Commons License This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Online ISSN Number 2455-538X
Management options and Decision making algorithm for Distal Femur fractures
/in Jan - April 2016 | Volume 2 | Issue 1Volume 2 | Issue 1 | Jan-Apr 2016 | Page 7-12|Mohsin e Azam
Author: Mohsin-e-Azam[1]
[1] iCare Clinics, Dubai UAE.
Address of Correspondence
Dr. Mohsin e Azam,
.Dr Mohsin-e-Azam
MBBS, MCPS, FCPS, Dip IT, Dip Bioethics
Specialist Orthopaedic Surgeon
iCare Clinics, Dubai UAE
Email: mohsindoc@gmail.com
Abstract
Distal femur is a complex fractures and most of times a personalized approach is needed for these fractures. Over a period of time variety of approaches and implants have been used for these fractures. The guiding principles for achieving good prognosis is meticulous surgical technique, preservation of fracture biology, restoration of articular surface and overall alignment of the limb. In case of geriatric fractures factors like long terms health and functional goals also need to be taken into consideration in planning treatment. This review focusses on providing an overview of the management options and lay down the premise for the symposium
Keywords: .Distal femur fractures, surgical management, decision making
Introduction
Distal femur fractures have been reported to account for between 4% and 6% of all femoral fractures[1, 2]. The distribution of fractures of this region is bimodal both in terms of age and mechanism. Distal femur fractures can result from either high-energy trauma or low-energy trauma. High-energy trauma such as road traffic accidents and sports accidents are more likely in men ages 15–50, whereas low-energy trauma such as falls from standing height at home are more likely to lead to distal femur fractures in women aged 50 and above. There is also the addition of the peri-prosthetic fracture group in the geriatric population with osteoporosis. In both cases axial loading of the leg is the most common mechanism of injury[2]. The fractures can be open or closed, due to their peri-articular location, can also have associated injuries of the patella and tibia. Proper antibiotic prophylaxis is essential to reduce the rate of infection in open fractures[3]. In cases of high energy trauma there can be associated neurovascular injury. Hence the neurovascular status of the extremity should be monitored closely in the perioperative and postoperative period. For evaluation of the fractures AP and Lateral X-Rays are obtained. Where articular comminution is present CT (computerized tomography) can aid in better understanding of the fracture geometry. 3D reconstruction images can further clarify complex articular injuries and coronal plane fractures[4]. As for all peri-articular fractures the restoration of articular surface and joint alignment requires thorough assessment of the fracture character and proper preoperative planning. Failing to do so can result into severe permanent disability specially if there is loss of knee stability and function[5].
Classically, the treatment of choice for management of femoral fractures, including supracondylar fractures, was with different types of splints. In 1907 and 1909, Steinmann and Kirschner, respectively, developed the first traction treatment modalities with the use of pins or wires under tension. A single pin is usually placed in proximal tibia when applying skeletal traction for treating these fractures[6].
Retrospective reports during the 1960’s by Stewart et al. (1966) and Neer et al. (1967) favored simple non-operative methods of treatment. However, in the next decade the pendulum started to shift as new surgical methods and materials improved the results of surgery according to Miiller et al[1].
Progressively with time better understanding of anatomy and fracture characteristics led to improved implant designs and improved outcomes. The modalities for fixation of distal femoral fractures can be broadly classified into external fixation, Conventional plating (sliding screws, blade plates and Dynamic compression plates), Locked plate fixation, Intramedullary nailing and arthroplasty.
Non Operative Management
The options of non-operative management are splint, cast and traction. Thomas and Meggit compared different non operative modalities and observed that there was no significant difference in the malunion rates between the splint versus the cast brace treatment. Although there was delayed union associated with splints[7]. Butt et al. evaluated operative (dynamic condylar screw) versus conservative (skeletal traction) treatment in a randomized control trial for displaced distal femur fracture in elderly patients. Good or excellent results were obtained in 53% of the operative patients versus 31% in the conservative group. The non-operative group had an increased risk for deep vein thrombosis (despite anticoagulation therapy), pulmonary and urinary tract infections, non-unions, mal-unions, knee joint stiffness, skin related complications and pin tract infections[8]. Therefore the application of the non-operative treatment is limited to only certain conditions like non-displaced fractures, bed bound patients, patients unfit to undergo surgery due to comorbidities[9].
Operative Management
Fractures of the distal femur can be managed successfully with surgery. A good result depends on identification of all fragments, adequate repair of soft tissue, appropriate bone grafting, meticulous inter-fragmentary compression, and complete reduction of the joint space[10].
Indications for operative management include open fractures, displaced fractures, intra-articular fractures, fractures associated with neurovascular compromise, ipsilateral lower extremity fractures, irreducible fractures, pathologic fractures and non-unions.
The implant and technique used is determined by fracture pattern, bone quality, the hemodynamic stability of the patient, and the skill and experience of the surgeon[11].
Surgical Techniques
ORIF Approaches
Surgical approach usually depends upon the character of the fracture and the choice of the implant. Most commonly performed approach is the lateral approach.
Lateral Approach
This approach is employed for fractures without articular involvement or simple articular extension. It is performed in the supine position with the knee flexed to 30 degrees. Flexing the knee releases the traction caused by gastrocnemius muscle and prevents extension of the distal fragment. This approach can be extended as required proximally to mid-thigh and to the lateral parapatellar region distally. The approach relies on an atraumatic elevation of the vastus lateralis from the lateral aspect of the distal femur, and a lateral arthrotomy for joint access. Articular reduction and lateral plate placement can both be achieved with the same approach. When extended proximally this approach can provide access to the entire length of the femoral shaft. Fractures of the medial femoral condyle and more complex fractures can also be handled with a lateral approach[12]. Occasionally a medial para-patellar approach may be utilized to provide good view of the articular surface of the distal femur.
Medial parapatellar
A medial approach to the distal femur may be used for a medial distal femoral fracture or in case of a coronal split (Hoffa-type fracture) of the femoral condyles. It can also be used in conjunction with lateral exposure when double plating of the distal end of the femur is indicated for severe supracondylar comminution or for bone defects requiring additional medial stabilization and in patients with complex combined supracondylar and intracondylar fractures. The vastus medialis is reflected anteriorly to expose the distal medial shaft of the femur. Structures to be protected in this approach are medial collateral ligament, the medial meniscus and the femoral artery and vein as they leave the adductor canal[13].
Surgical Algorithm
For extra articular distal femur fractures a minimally invasive surgical approach can be utilized, this approach preserves the fracture biology. This can be achieved by minimal invasive plate osteosynthesis or retrograde intramedullary nailing. Either approach allows for bridging of the fracture. This approach is superior to open reduction and internal fixation of intermediate fragments where blood supply may be impaired. Compression mode plating has been found superior to bridging mode and should be performed where feasible[14].
For simple articular fractures open reduction of the affected femoral condyle is required to achieve anatomic reduction. Lag screws can be used to reduce the articular fragments followed by a plate for osteosynthesis.
In case of the comminuted articular fractures visualization of the knee joint is required in order to reduce and anatomically reconstruct the articular surface. Temporary k-wire fixation can be performed followed by placement of lag screws using 3.5 mm screws. Afterwards the articular bloc is fixed to the femoral shaft. No matter which kind of fixation is performed it is imperative to restore axial alignment, length and rotation of the lower limb for good functional recovery[15].
In severely comminuted fractures a spanning external fixator may be used as a salvage procedure. The external fixator may be applied for several weeks in order to achieve adequate conditions for later total knee arthroplasty[16].
External Fixation
External fixation is commonly used as a temporary measure of these fractures, in particular for displaced intra-articular fractures. Mainly used when there is an open fracture, significant comminution, bone loss, vascular compromise or extensive soft tissue damage. A bilateral fracture or a floating knee are also examples of complex fractures requiring external fixation. Proper placement of pins away from the zone of injury will reduce the risk of infection and maintain the integrity of the soft tissue for definitive management at a later stage[17].
With Monolateral fixators, it is difficult to control alignment, the stability is often poor, there is no fixation of the articular component and stabilization of the fracture requires bridging the knee, which increases the risk of stiffness. As a damage control measure external fixation provides opportunity for medical management, reduction in pain and facilitates nursing care till definitive treatment can be performed. Severely comminuted fractures can also be treated definitively with tensioned external fixation devices such as the Ilizarov fixator.
Oh et al. reported results of a series of 59 complex intra-articular fractures with temporary bridging external fixation. There were seven complications including four that developed in distal femoral fractures which were infection and the unsuccessful control of leg length[18]. Parekh et al. reported good results in staged management of complex intra-articular fractures around the knee, with 16 distal femoral fractures in a series of 47 cases[19]. Zlowodzki et al. reported an average 7.2% nonunion rate, 1.5% rate of fixation failure, 4.3% rate of deep infection, and 30.6% need for secondary surgical procedures when distal femoral fractures were treated with external fixation[20]. Arazi et al. evaluated 14 complex fractures treated with Ilizarov external fixator and found that union occurs around 16 weeks with a mean ROM of 105 degrees at the knee. With the only complication being an infected nonunion, they concluded that the fixator is a safe option that provides adequate stability[21]. Kumar and colleagues examined the outcomes of the Ilizarov fixator in open supracondylar fractures and found that union occurred much later at 39 weeks, with at least 4 cm of shortening noted in 40% of fractures and pin-track infections in 21% of patients[22].
Conventional Plate Systems
After the 70s, better results to support ORIF in fractures of the distal femur were reported in literature[1, 23] Shahcheraghi et. al. compared ORIF with closed reduction directly, preferred ORIF with good or excellent clinical results registered, 81% open versus 42% closed and a significantly reduced malunion rate, 3% open versus 37% closed[15]. With the availability of the fixed angle blade plate the care for the distal femur fracture got transformed. This construct provided polyaxial stability and inherent rigidity. Earlier designs constituted an angled side plate that could be impacted into the distal femur and fixed to the distal femur by the precontured region of the plate across the metaphyseal flare. The angle of the blade was commonly 95 degrees and careful implantation ensured that length and alignment could be restored even in injuries with metaphyseal comminution. The major drawback of this design was that it required a large exposure. Furthermore, it could not be used in cases of osteoporosis and was unable to address the coronal plane fractures[5]. Later another implant was designed on the fixed angle concept with a sliding screw and was called the Dynamic Condylar Screw (DCS). This implant provided the ability to compress the intercondylar fragments. This design was adopted for the ease of application and smaller exposure. But it still did not address the coronal fracture limitation of the angled blade plate and also resulted in more bone loss upon insertion which made revisions difficult[24].
In general open reduction and internal fixation requires extensive dissection and can therefore lead to devascularization of fracture fragments, hence there is an increased risk of delayed union, non-union and infection[25]. To decrease these complications, concepts evolved applying indirect reduction techniques to restore length, rotation, and the mechanical axis without direct exposure of the fracture site and therefore maintaining the blood supply to the fracture region. Indirect reduction techniques were shown to have a biological advantage. Bolhofner et al. treated 57 patients with distal femoral fractures with conventional plates using only indirect reduction techniques. The average time to fracture union and full weight bearing was 10.7 weeks with no non-unions or hardware failures reported. These results could be achieved although 11 patients with open fractures were included[26].
Keeping in view the problems with open reduction and internal fixation and advantages of indirect reduction and preservation of vascularity of fracture fragments evolution occurred to wards minimally invasive surgery[27]. Studies have shown the preservation of soft tissue perforators and specially of the periosteal blood supply while using minimally invasive plate osteosynthesis (MIPO) techniques. Furthermore it decreased the incidence of infection, implant failure and led to earlier callus formation and decreased the need for subsequent bone grafting[20].
Locked Plate Fixation
With the development of different options in plate osteosynthesis, the locked pre-contoured plates have become widely used in orthopedics for many different fractures. Unlike the previously used (conventional) plates, which required friction between the plate bone interface for stability, the locking plates have mechanisms to secure the screw heads to the plate. This allows for the screws to be placed at different angles. The major advantage is that the plate doesn’t not have to be in contact with the bone. This allows for preservation of the periosteal blood supply[27].
Locking plate can be used in an open reduction and internal fixation procedure when the fracture is intraarticular, or with minimally invasive surgery using the less invasive stabilization system (LISS) in case of an extra-articular fracture or a simple non- displaced fracture[28]. One of the disadvantages of locking plate is the lack of interfragmentary compression with locking screws, this requires fixation of fragments with placement of lag screws prior to plate fixation. Extra care while insertion is required to prevent the interference of lag screws with the locked screws. There is a learning curve associated specially when using LISS in order to achieve union and prevent malunion and mechanical failure[29].
Although locking plates provide the biological advantage, at the same time they create rigid constructs which can suppress fracture union. As micro motion across the fracture site has been long known to cause stimulation of healing across the fracture fragments. Making the construct too rigid can affect the callus formation[30]. Choice of material also affects rigidity, stainless steel being more rigid, whereas titanium and associated alloys provide more flexibility[31].
In locking plates there are variations that exist based on the locking mechanism of the screws. One type has the unidirectional screws and the other has polyaxial screws. Polyaxaial system allows for more accurate screw placement, especially in the peri-articular regions. As a further development, a hybrid locking plate was made known as the Locked compression plate (LCP) which contains holes for both locking screws and cortrical screws. This system allowed for interfragmentry compression similar to a dynamic compression plate (DCP)[32].
In the literature there are many biomechanical studies that evaluate locking plate fixation systems. Beingessner et al. compared titanium plates to steel plates as well as unicortical to bicortial screws. They concluded that strength under torsion is reduced in titanium plates and strength is improved with bicortical screws. Whereas there is no difference for axial compression strains and plastic deformity[33].
Lujan et al. demonstrated that titanium plates favor the formation of callus due to elasticity in fixation material[31]. Stoeffel et al. when comparing LCP, DCP and Hybrid fixation showed that locking system results in less loss of reduction under axial compression with less plastic deformity and the DCP system provides better strength under torsion. The conclusion was that Hybrid fixation is preferred[34]. Wilkens et al. showed that the placement of polyaxial screws increased strength under axial compression and torsion and reduces deformation when loaded[35]. Freeman et al. compared load to failure, axial stiffness, and screw extraction torque for distal femoral locking plates with locked or cortical screws. Results demonstrated that locked fixation was superior in the osteoporotic model only[36]. Buckley et al. brought forward the issue of mal-rotation following MIPO if careful intra operative assessment is not done[37].
Recently, Tank et. al. concluded that early mechanical failure with the variable angle distal femoral locking plate is higher than traditional locking plates (LCP and LISS) for comminuted intraarticular distal femur fractures. They advised against use of this plate for metaphyseal fragmented distal femur fractures[38].
In a randomized prospective multicenter controlled trial comparing the Less Invasive Stabilization System (LISS) with the minimally invasive Dynamic Condylar Screw System (DCS) published by the Canadian orthopedic trauma society, they concluded that there was no statistically significant difference between LISS and DCS in terms of the number of fractures healed, time to union, or functional scores. Complications and revisions were more common in the LISS group. Only 52% of the LISS group healed without intervention by 12 months compared with 91% in the DCS group[39].
Interlocked IM nail
Intramedullary nailing is a good surgical option for distal femur fracture. It helps avoid extensive soft tissue dissection and minimize secondary damage of devascularization of fracture fragments[40]. This method has been recommended for non-comminuted fractures with intact distal femur to allow for interlocking. Both ante- and retrograde nailing have successfully been applied in the treatment of even comminuted and intraarticular fractures, but antegrade nailing has lost appeal[41]. Antegrade nailing has now been reserved for extraarticular fractures with fracture line > 5 cm proximal to the articular surface to allow for adequate distal fixation. The only advantage of antegrade nailing is the avoidance of an arthrotomy[32]. Retrograde nailing prevailed due to availability more options of distal fragment fixation. As with minimally invasive plate osteosynthesis, indirect fracture reduction and a minimally invasive approach were adopted for nailing as well.
Handolin et. al. reported in a series of 44 patients with 46 distal femur fractures with retrograde nailing, that the final union rate was 95% and a mean union time was 17.5 weeks. However, there were three patients with a loss of reduction and two of them had to undergo a re-operation[42]. Henry et al. compared open versus percutaneous reduction techniques for retrograde nailing of distal femoral fractures. The authors concluded improved post-operative knee function with decreased operative time, blood loss, bone grafting, and non-union rates without differences in malunion rate[43]. Hartin et. al. compared nailing vs plate fixation in fractures of the distal femur. They demonstrated high union rates in both groups without any statistically significant difference between groups. They observed that the deep infection rate, knee range of motion and healing time was better in the nailing group but was not statistically significant[44].
Disadvantages of the nailing technique may be a lack of alignment control, posterior angulation, perforation of joint cartilage and intra-articular distribution of reaming debris. Stability is limited if small diameter and short nails are inserted[45].
Arthroplasty
Complex peri-articular fractures can be a challenging to treat especially in the elderly. Even after achieving anatomic reconstruction and rehabilitation, posttraumatic arthritis and knee pain are complaints that commonly arise in addition to any baseline osteoarthritis. In younger patients the use of primary arthroplasty or distal femoral replacement may not be a viable option but in elderly it can be a valuable consideration, especially in the presence of primary osteoarthritis and comminution of the femoral condyles. Thin cortices, wide intramedullary canal and osteoporosis can make stable primary fixation difficulty to achieve, especially in the presence of multiple medical co-morbids[46]. Preservation of knee function and early weight bearing should be the objectives of management in the geriatric population[47]. Careful pre-operative planning and imaging is required to gauge the extent of injury. Radiography of the contralateral limb can act as a template in planning. Depending on the extent of the fracture and its pattern implant choice can be made. Primary total knee arthroplasty implants for non-comminuted fractures, revision TKA implants in the presence of metaphyseal extension, distal femoral replacement in cases of significant metaphyseal comminution and hinged implants where there is ligamentous instability. Addition of plates, lag screws, cables and cement can be done to achieve the required stability[48]. Choi et. al. performed TKA with the Medial Pivot prosthesis in 8 patients with ages between 65 and 89 who had primary osteoarthritis along with a distal femur fracture. They reported a mean time of 15 weeks to union and a good clinical result for all patients. They concluded that primary TKA can be considered as an option for the treatment of minimally comminuted distal femoral fractures in elderly patients who have advanced osteoarthritis of the knee with appropriate bone stock[49]. Appleton et. al. reported results of hinged total knee replacement in treatment of 54 fractures in 52 patients with a mean age of 82 years. Within the first year after implantation 22 of the 54 patients had died, six required further operation and two required revision surgery. They concluded that hinged total knee is useful alternative treatment to internal fixation in elderly patients and has a high probability of surviving as long as the patient[50]. Arthroplasty for peri articular fracture may not be seen as a paradigm shift but instead as a good alternative, for a certain patient group, that requires a strict indication and an experienced surgeon[51].
:Conclusion
With the evolution of techniques and implants over time the treatment of the distal femoral fracture has improved. Although the advantage of one system of fixation over the other cannot be absolutely concluded, the main dependence of the surgical decision remains more on the fracture pattern and familiarity of the surgeon with the use of a certain implant and technique. The guiding principles for achieving good prognosis is meticulous surgical technique, preservation of fracture biology, restoration of articular surface and overall alignment of the limb. In case of geriatric fractures factors like long terms health and functional goals also need to be taken into consideration in planning treatment.
References
1. Kolmert L, Wulff K. Epidemiology and treatment of distal femoral fractures in adults. Acta orthopaedica Scandinavica. 1982;53(6):957-62.
2. Martinet O, Cordey J, Harder Y, Maier A, Buhler M, Barraud GE. The epidemiology of fractures of the distal femur. Injury. 2000;31 Suppl 3:C62-3.
3. Gillespie WJ, Walenkamp GH. Antibiotic prophylaxis for surgery for proximal femoral and other closed long bone fractures. The Cochrane database of systematic reviews. 2010(3):CD000244.
4. Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S, et al. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. The Journal of bone and joint surgery American volume. 2005;87(3):564-9.
5. Gwathmey FW, Jr., Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. The Journal of the American Academy of Orthopaedic Surgeons. 2010;18(10):597-607.
6. Al-Khateeb H, Peckham T, Ibrahim E. A novel technique in applying skeletal traction for long bone fractures. Annals of the Royal College of Surgeons of England. 2008;90(5):432-3.
7. Thomas TL, Meggitt BF. A comparative study of methods for treating fractures of the distal half of the femur. The Journal of bone and joint surgery British volume. 1981;63-B(1):3-6.
8. Butt MS, Krikler SJ, Ali MS. Displaced fractures of the distal femur in elderly patients. Operative versus non-operative treatment. The Journal of bone and joint surgery British volume. 1996;78(1):110-4.
9. Cass J, Sems SA. Operative versus nonoperative management of distal femur fracture in myelopathic, nonambulatory patients. Orthopedics. 2008;31(11):1091.
10. Foster TE, Healy WL. Operative management of distal femoral fractures. Orthopaedic review. 1991;20(11):962-9.
11. Jeffrey T, Jonna K, Patel D. Open Reduction And Internal Fixation Of Distal Femoral Fractures In Adults: Overview, Periprocedural Care, Technique 2016 [5 Jan. 2016]. Available from: http://emedicine.medscape.com/article/2000429-overview.
12. Florian Gebhard PK, Chris Oliver. Distal femur [30 Jan. 2016]. Available from: https://www2.aofoundation.org/wps/portal/surgery.
13. Krettek Christian DLH. Fractures of the Distal Femur. In: Browner BD, editor. Skeletal Trauma. Philadelphia, PA: Saunders; 1992. p. 1957-2011.
14. Liu F, Tao R, Cao Y, Wang Y, Zhou Z, Wang H, et al. The role of LISS (less invasive stabilisation system) in the treatment of peri-knee fractures. Injury. 2009;40(11):1187-94.
15. Shahcheraghi GH, Doroodchi HR. Supracondylar fracture of the femur: closed or open reduction? The Journal of trauma. 1993;34(4):499-502.
16. Papadopoulos EC, Parvizi J, Lai CH, Lewallen DG. Total knee arthroplasty following prior distal femoral fracture. The Knee. 2002;9(4):267-74.
17. Haidukewych GJ. Temporary external fixation for the management of complex intra- and periarticular fractures of the lower extremity. Journal of orthopaedic trauma. 2002;16(9):678-85.
18. Oh JK, Hwang JH, Sahu D, Jun SH. Complication rate and pitfalls of temporary bridging external fixator in periarticular communited fractures. Clinics in orthopedic surgery. 2011;3(1):62-8.
19. Parekh AA, Smith WR, Silva S, Agudelo JF, Williams AE, Hak D, et al. Treatment of distal femur and proximal tibia fractures with external fixation followed by planned conversion to internal fixation. The Journal of trauma. 2008;64(3):736-9.
20. Zlowodzki M, Bhandari M, Marek DJ, Cole PA, Kregor PJ. Operative treatment of acute distal femur fractures: systematic review of 2 comparative studies and 45 case series (1989 to 2005). Journal of orthopaedic trauma. 2006;20(5):366-71.
21. Arazi M, Memik R, Ogun TC, Yel M. Ilizarov external fixation for severely comminuted supracondylar and intercondylar fractures of the distal femur. The Journal of bone and joint surgery British volume. 2001;83(5):663-7.
22. Kumar P, Singh GK, Singh M, Bajraacharya S. Treatment of Gustilo grade III B supracondylar fractures of the femur with Ilizarov external fixation. Acta orthopaedica Belgica. 2006;72(3):332-6.
23. Schatzker J, Home G, Waddell J. The Toronto experience with the supracondylar fracture of the femur, 1966-72. Injury. 1974;6(2):113-28.
24. Sanders R, Regazzoni P, Ruedi TP. Treatment of Supracondylar-Intracondylar Fractures of the Femur Using the Dynamic Condylar Screw. Journal of orthopaedic trauma. 1989;3(3):214-22.
25. Stover M. Distal femoral fractures: current treatment, results and problems. Injury. 2001;32 Suppl 3:SC3-13.
26. Bolhofner BR, Carmen B, Clifford P. The results of open reduction and Internal fixation of distal femur fractures using a biologic (indirect) reduction technique. Journal of orthopaedic trauma. 1996;10(6):372-7.
27. Krettek C, Muller M, Miclau T. Evolution of minimally invasive plate osteosynthesis (MIPO) in the femur. Injury. 2001;32 Suppl 3:SC14-23.
28. Ehlinger M, Adam P, Abane L, Arlettaz Y, Bonnomet F. Minimally-invasive internal fixation of extra-articular distal femur fractures using a locking plate: tricks of the trade. Orthopaedics & traumatology, surgery & research : OTSR. 2011;97(2):201-5.
29. Ehlinger M, Adam P, Arlettaz Y, Moor BK, DiMarco A, Brinkert D, et al. Minimally-invasive fixation of distal extra-articular femur fractures with locking plates: limitations and failures. Orthopaedics & traumatology, surgery & research : OTSR. 2011;97(6):668-74.
30. Henderson CE, Lujan TJ, Kuhl LL, Bottlang M, Fitzpatrick DC, Marsh JL. 2010 mid-America Orthopaedic Association Physician in Training Award: healing complications are common after locked plating for distal femur fractures. Clinical orthopaedics and related research. 2011;469(6):1757-65.
31. Lujan TJ, Henderson CE, Madey SM, Fitzpatrick DC, Marsh JL, Bottlang M. Locked plating of distal femur fractures leads to inconsistent and asymmetric callus formation. Journal of orthopaedic trauma. 2010;24(3):156-62.
32. Crist BD, Della Rocca GJ, Murtha YM. Treatment of acute distal femur fractures. Orthopedics. 2008;31(7):681-90.
33. Beingessner D, Moon E, Barei D, Morshed S. Biomechanical analysis of the less invasive stabilization system for mechanically unstable fractures of the distal femur: comparison of titanium versus stainless steel and bicortical versus unicortical fixation. The Journal of trauma. 2011;71(3):620-4.
34. Stoffel K, Lorenz KU, Kuster MS. Biomechanical considerations in plate osteosynthesis: the effect of plate-to-bone compression with and without angular screw stability. Journal of orthopaedic trauma. 2007;21(6):362-8.
35. Wilkens KJ, Curtiss S, Lee MA. Polyaxial locking plate fixation in distal femur fractures: a biomechanical comparison. Journal of orthopaedic trauma. 2008;22(9):624-8.
36. Freeman AL, Tornetta P, 3rd, Schmidt A, Bechtold J, Ricci W, Fleming M. How much do locked screws add to the fixation of “hybrid” plate constructs in osteoporotic bone? Journal of orthopaedic trauma. 2010;24(3):163-9.
37. Buckley R, Mohanty K, Malish D. Lower limb malrotation following MIPO technique of distal femoral and proximal tibial fractures. Injury. 2011;42(2):194-9.
38. Tank JC, Schneider PS, Davis E, Galpin M, Prasarn ML, Choo AM, et al. Early Mechanical Failures of the Synthes Variable Angle Locking Distal Femur Plate. Journal of orthopaedic trauma. 2016;30(1):e7-e11.
39. Society COT. Are Locking Constructs in Distal Femoral Fractures Always Best? A Prospective Multicenter Randomized Controlled Trial Comparing the Less Invasive Stabilization System With the Minimally Invasive Dynamic Condylar Screw System. Journal of orthopaedic trauma. 2016;30(1):e1-e6.
40. Kim J, Kang SB, Nam K, Rhee SH, Won JW, Han HS. Retrograde intramedullary nailing for distal femur fracture with osteoporosis. Clinics in orthopedic surgery. 2012;4(4):307-12.
41. Butler MS, Brumback RJ, Ellison TS, Poka A, Bathon GH, Burgess AR. Interlocking intramedullary nailing for ipsilateral fractures of the femoral shaft and distal part of the femur. The Journal of bone and joint surgery American volume. 1991;73(10):1492-502.
42. Handolin L, Pajarinen J, Lindahl J, Hirvensalo E. Retrograde intramedullary nailing in distal femoral fractures–results in a series of 46 consecutive operations. Injury. 2004;35(5):517-22.
43. Henry SL. Supracondylar femur fractures treated percutaneously. Clinical orthopaedics and related research. 2000(375):51-9.
44. Hartin NL, Harris I, Hazratwala K. Retrograde nailing versus fixed-angle blade plating for supracondylar femoral fractures: a randomized controlled trial. ANZ journal of surgery. 2006;76(5):290-4.
45. Hierholzer C, von Rüden C, Pötzel T, Woltmann A, Bühren V. Outcome analysis of retrograde nailing and less invasive stabilization system in distal femoral fractures: A retrospective analysis. Indian Journal of Orthopaedics. 2011;45(3):243-50.
46. Bell KM, Johnstone AJ, Court-Brown CM, Hughes SP. Primary knee arthroplasty for distal femoral fractures in elderly patients. The Journal of bone and joint surgery British volume. 1992;74(3):400-2.
47. Mounasamy V, Cui Q, Brown TE, Saleh KJ, Mihalko WM. Primary total knee arthroplasty for a complex distal femur fracture in the elderly: a case report. European Journal of Orthopaedic Surgery & Traumatology. 2007;17(5):491-4.
48. Gangavalli AK, Nwachuku CO. Management of Distal Femur Fractures in Adults: An Overview of Options. The Orthopedic clinics of North America. 2016;47(1):85-96.
49. Choi NY, Sohn JM, Cho SG, Kim SC, In Y. Primary Total Knee Arthroplasty for Simple Distal Femoral Fractures in Elderly Patients with Knee Osteoarthritis. Knee surgery & related research. 2013;25(3):141-6.
50. Appleton P, Moran M, Houshian S, Robinson CM. Distal femoral fractures treated by hinged total knee replacement in elderly patients. The Journal of bone and joint surgery British volume. 2006;88(8):1065-70.
51. Thomas Haufe SF, Peter Müller, Johannes Plath, Edgar Mayr. The Role of a Primary Arthroplasty in the Treatment of Proximal Tibia Fractures in Orthogeriatric Patients. BioMed research international. 2016;2016:5.
Dr. Mohsin e Azam
(Abstract) (Full Text HTML) (Download PDF)
Classification of Distal Femur Fractures and Their Clinical Relevance
/in Jan - April 2016 | Volume 2 | Issue 1Volume 2 | Issue 1 | Jan-Apr 2016 | Page3-6 |Raja Bhaskara Kanakeshwar, Arun Kamal C, Dheenadayalan J
Author: Raja Bhaskara Kanakeshwar[1], Arun Kamal C[1], Dheenadayalan J[1]
[1]Ganga Hospital, 313, MTP road, Coimbatore , Tamilnadu, India Pin code – 641043
Address of Correspondence
Dr Raja Bhaskara Kanakeshwara
Ganga hospital,313, MTP road, Coimbatore , Tamilnadu, India, Pin code – 641043
Email id – rajalibra299@gmail.com
Abstract
Introduction: Analysis and classifying distal femur fractures is one of the important steps for an orthopaedic surgeon towards a successful outcome in treating these fractures. Few surgeons tried to classify these fractures and we discuss in detail those systems and their clinical relevance . Three classification systems have been discussed below and it has shown the Müller AO classification system remains the ideal classification for these fractures as it is user friendly, easy to document and gives an idea on the prognosis .
Keywords : Distal femur fracture, classification, Müller, AO, Hoffa.
Introduction
To treat a fracture better, we need to understand it better. To understand them better, we need to analyse them better and classify them . Distal femur fractures are often comminuted and intra-articular, and they frequently involve osteoporotic bone, which makes it difficult to reduce them while maintaining joint function and overall limb alignment [1,2]. Hence, classifying them in an appropriate manner which would help surgeons to give a better outcome is of utmost impotance. Unlike proximal femur fractures – which have numerous classifications to describe them – there are only a few systems proposed for distal femur fractures mainly due to the less complex muscular anatomy and vascular anatomy involved between both these regions[3,4,5].
For a classification system to have clinical significance, it must be able to :
1) allow adequate documentation so that a common language is possible to discuss these injuries
2) be ‘user friendly’
3) help in clinical decision making
4) prognosticate the outcome depending on the treatment option [3] .
We shall discuss about the various classification systems described for distal femur fractures and their clinical significance .
Classification of distal femur fractures and their clinical relevance
Classification systems in distal femur fractures :
The various classification systems described for distal femur fractures are (Table 1,2) :
1) Neer and associates ( 1967 )
2) Seinsheimer classification ( 1980 )
3) AO Classification – Müller ( 1990 )
Table 1: Basic algorithm – Distal femur fracture classification – Müller AO :
Table 2: Summary of Classification systems for distal femur fractures and their significance.
Neer and associates classification [ 8 ] :
One of the simpler classification systems of supracondylar femur fractures was that of Neer and associateswhich was described early in 1967 . They subdivided supracondylar- intracondylar femur fractures into three primary categories . The 2nd category had two subdivisions[ 8 ] .
Category I : Minimal displacement
Category II : Displacement of the condyles
A) Medial condyle displacement
B ) Lateral condyle displacement
Category III : Concomitant supracondylar and shaft fractures [Fig 1]
Figure1: Neer and associates classification
Clinical relevance :
This classification was very basic and did not give much clinical information to the surgeon . No light was thrown upon coronal plane fractures . Moreover , there was no information on the prognosis of these injuries[3]. Hence, this system did not gain much popularity and is seldom used anywhere now among trauma surgeons worldwide .
Seinsheimer classification [9] :
In 1980, Seinsheimer published his system where he classified the fractures of the distal 3.5 inches of the femur into 4 types [9].
Type I : Non-displaced fractures ( less than 2mm displacement )
Type II : Distal metaphyseal fractures ( Extra-articular )
II-A : 2 part fractures
II-B : Communited fractures
Type III : Fractures involving the intercondylar notch in which one or both condyles are separate fragments
Type IV : Intra-articular fractures
IV-A : Medial condyle fracture
IV-B : Lateral condyle fracture
IV-C : Comminuted fractures
Clinical relevance :
Seinsheimer found that the type I and II fracture patients had osteoporosis prior to the injury and they were usually following low energy trauma . On the other end of the spectrum , he found that type IV fractures resulted from high energy trauma[9]. This classification system though it had a better descriptive detail about the fracture pattern , did not become popular as it was not user friendly and provided minimal information on prognosis[3].
AO Classification system – Müller and associates [6,7,80] :
The “Schweizer Arbitsgemenischaft fur Oseosysthesesfragen” Group ( SWISS AO ) , chaired by Müller, through its documentation data centre in Davos brought forward their classification system on distal femur fractures after analysing thousands of these fractures . This system has been found to be easy to use and satisfies all the criteria for an ideal classification [3,8] .
Müller and his colleagues divided these fractures into 3 primary groups [6,8] . Based on the common principles of the AO classification, type A fractures include extra-articular fractures and type B fractures are partial articular fractures, meaning parts of the articular surface remains in contact with the diaphysis of the femur [Fig 2]. Type C fractures include complete articular fractures with both condyles being detached from the diaphysis. The fracture types are further subdivided describing the degree of comminution and other characteristics. Further subdivision of type B fractures includes Bl (sagittal, lateral condyle), B2 (sagittal, medial condyle) and B3 (frontal, Hoffa type). Fracture type C is divided in C1 (articular simple, metaphyseal simple), C2 (articular simple, metaphyseal multifragmentary) and C3 (multifragmentary)[8].
Figure 2: The Müller Classification
The B3 type fracture – popularly known as ‘Hoffa’s fracture’- has immense clinical signifcance in the outcome following treatment and has been further subdivided into three types [3,8,10] . This type of cornoal fractures of he distal femur are further classified into :
B3.1 – Anterior and lateral flake fracture
B3.2 – Unicondylar Hoffa’s fracture
B3.3 – Bicondylar Hoffa’s fracture
Clinical relevance :
This classification also states that progressing from type A to type C , the severity of the trauma and injury increases whereas the prognosis for a good outcome decreases [3,10,14] . This relation also holds true for the progression from type 1 to type 3 in each group . Communication among surgeons worldwide regarding distal fractures using this system was easy and it was unanimously accepted as the gold standard classification woldwide [3,9].
Regarding the appropriate treatment or surgical option for any particular type of fracture based on the AO Müller classification system , there have been many articles published[11-16] (Table 3) . The final treatment for the patient anyhow needs to be taken by the treating surgeon depending upon many factors including the soft tissue status and the general condition of the patient [16]. A variety of surgical exposures, reduction techniques and various new implants have been developed to treat such fractures and these include intramedullary nailing, screw fixation ,periarticular locked plating and also the LISS ( Less Invasive Stabilization System ) technique [15,16] .
However, in simple fractures compression osteosynthesis should be favoured over bridging osteosynthesis since higher rates of non-unions have been reported for using locking plating for treatment of simple fractures[12].
Table 3: The recommended Surgical treatment option based upon the type of the Muller’s classification is[ 12,13 ]
Among all the classifications described for distal femur fractures, the Müller AO classification system is the most widely accepted system and is being used worldwide. This classification takes into account the involvement of anatomic region of the distal femur, the energy of the injury and also prognosticates the outcome . It has a high inter-observer reliability and validity. Being user friendly and also serving as a common language among surgeons worldwide to discuss distal femur fractures, this classification is the one of choice for treating these fractures.
References
1. Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. J Am Acad Orthop Surg. 2010 Oct;18(10):597-607.
2. Everhart JS, Chaudhari AM, Flanigan DC. Creation of a simple distal femur morphology classification system. J Orthop Res. 2015 Nov 17.
3. Krettek C, Schandelmaier P, Richter M, Tscherne H. [Distal femoral fractures].Swiss Surg. 1998;(6):263-78.
4. Martinet O, Cordey J, Harder Y, Maier A, Bühler M, Barraud GE. The epidemiology of fractures of the distal femur. Injury. 2000 Sep;31 Suppl 3:C62-3.
5. Mu¨ller, M.E.; Allgo¨wer, M.; Schneider, R.; Willenegger, H. Manual of Internal Fixation, 3rd ed. New York, Springer-Verlag, 1991.
6. Mu¨ller, M.E.; Nazarian, S.; Koch, P. 1987. Classification AO des Fractures. Springer-Verlag New York,
7. Mu¨ller, M.E.; Nazarian, S.; Koch, P.; Schatzker, J. The Comprehensive Classification of Fractures of Long Bones. New York, Springer-Verlag, 1990.
8. Neer, C.S.; Grantham, S.A.; Shelton, M.L. Supracondylar fracture of the adult femur. A study of one hundred and ten cases. J Bone Joint Surg Am 49:591–613, 1967.
9. Seinsheimer, F. Fractures of the distal femur. Clin Orthop 153:169–179, 1980.
10. Stover M.: Distal femoral fractures: current treatment, results and problems. Injury, 32 (Suppl. 3): SC3-13, 2001
11. ZLOWODZKI M, BHANDARI M, MAREK DJ, COLE PA, KREGOR PJ. Operative treatment of acute distal femur fractures: systematic review of 2 comparative studies and 45 case series (1989 to 2005). J. Orthop. Trauma, 20: 366-371, 2006
12. LIU, E., TAO, R., CAO, Y., WANG, Y., ZHOU, Z., WANG, H., et al.: The role of LISS (less invasive stabilisation system) in the treatment of peri-knee fractures. Injury, 40: 1187-1194, 2009.
13. SHAHCHERAGHI, G. H., DOROODCHI, H. R.: Supracondylar fracture of the femur: closed or open reduction? J. Trauma, 34: 499-502, 1993.
14. Bel JC, Court C, Cogan A, Chantelot C, Piétu G, Vandenbussche E; SoFCOT. Unicondylar fractures of the distal femur. Orthop Traumatol Surg Res. 2014 Dec;100(8):873-7.
15. Arastu MH, Kokke MC, Duffy PJ, Korley RE, Buckley RE. Coronal plane partial articular fractures of the distal femoral condyle: current concepts in management. Bone Joint J. 2013 Sep;95-B(9):1165-71.
16. Pritchett, J.W. Supracondylar fractures of the femur. Clin Orthop 184:173–177, 1984.
Dr. Raja Bhaskara Kanakeshwara
Dr. Arun Kamal C
Dr. Dheendalayan J
(Abstract) (Full Text HTML) (Download PDF)
Non Union Distal Femur Fracture: Causes and Management Options
/in Jan - April 2016 | Volume 2 | Issue 1Volume 2 | Issue 1 | Jan-April 2016 | Page 28-33|Puneet Maheshwari, Pramod Maheshwari
Author: Puneet Maheshwari[1], Pramod Maheshwari[1]
[1] Maheshwari Nursing Home, 163, Bhagat Singh Marg
Dewas M.P. 455001, India
Address of Correspondence
Dr. Puneet Maheshwari
Maheshwari Nursing Home, 163, Bhagat Singh Marg
Dewas M.P. 455001, India
Email: puneet1984@gmail.com
Abstract
Distal femur fractures are common but complex fractures and often are associated with complications. The cases of failure may be secondary to mechanical failure or biological failure. The current review offers overview of these complications and tips and tricks on how to manage these complications.
Keywords: Distal Femur Fractures, Complications, Surgical management
Introduction
Distal femoral fractures are a common orthopaedic problem in all age groups of patients with and incidence of about 37 per 100,000 person years.(1) Distal femoral fractures since a long time has been considered difficult to treat using traditional implants due to high failure rate and secondary varus collapse. (2)
Distal femoral fractures in young age group is most commonly due to high energy trauma while in older age group it is mostly associated with fall from height or walking along with osteoporosis of bones. Treatment of these fractures can be successfully done with variety of plates(3-6) and retrograde intramedullary nails(7-10).
Early studies of treating distal femoral fractures with locked plates reported excellent out come with non-union rates of 0-14% (mostly less than 6%) (4, 11-21).
However, with the recent data being analyzed and reported the non-union rates are now as high has 17-21% (11, 22, 23). This can be partially attributed to wider variety of fracture morphology and in patients prone for development of non-union.
Definition of Non-union
Non-union definition is based on three factors namely, duration of time since injury, characteristics of fracture on serial x-rays and lastly clinical parameters assessed by the treating surgeon.
Presently, US FDA defines non-union as fracture bone that has not completely healed in 9 months since injury and which has not shown any signs of healing over 3 consecutive months on serial x-rays.(24)
Multiple literatures indicates that optimal time for healing is in between 4 to 12 months, taking into account the type of bone fractured, nature of injury and quality of the soft tissues around the fractured bone. (25-33)
Along with these factors one more important factor is the physiologic capability of the individual in mounting a healing response.
Classification
Distal femur fractures (AO classification)
As per the AO classification the distal femur (33) can be classified in to 3 types namely extra-articular, partial articular and complete articular factures, which are further classified.
Distal femur fractures are:
Type 33A: extraarticular fracture
o A1: simple
o A2: metaphyseal wedge and/or fragmented wedge
o A3: metaphyseal complex
Type 33B: partial articular fracture
o B1: lateral condyle, sagittal
o B2: medial condyle, sagittal
o B3: frontal
Type 33C: complete articular fracture
o C1: articular simple, metaphyseal simple
o C2: articular simple, metaphyseal multifragmentary
o C3: articular multifragmentary
Weber and Cech have classified femoral non-union based on the viability or blood supply of the fracture into two broad groups viable and non-viable types. (24)
Viable type of non-union has an intact blood supply to the fracture area and thus body can mount a healing response to injury. Viable type is further divided into hypertrophic and oligo-trophic non-union.
Non-viable type of non-union is also called as atrophic or avascular non-union. The vascularity of the fracture area is absent and thus it cannot mount a healing response to injury. Type of non-union can be determined on plain x-ray in AP and lateral view or more accurately on bone scans.
Classification of non-union is important not just for documentation purposes but also for management point. In a viable non-union minimally invasive or non-invasive treatment can lead to union and thus saving the patient from another major surgical procedure.
These procedures would be give a questionable healing response in case of atrophic non-union and there the surgeon need to be more aggressive and has to plan a more extensive treatment.
Diagnosis and Evaluation
It is extremely important for the treating surgeon to timely diagnose, evaluate and document a non-union both for management as well as for legal purpose.
Diagnosis begins with a detailed history and examination of the patient and the affected limb. Patient-related risk factors like tobacco addiction, use of analgesics peripheral vascular disease, diabetes should be looked for and documented. Any clinical symptom that may point towards infection (occult/overt) like fever, malaise, night pain or history of wound healing problem should be elicited.
Physical examination should identify and document any deformity, pain over fracture area, soft tissue cover problems, increased local temperature, drainage, abnormal mobility, crepitation, and limb length discrepancy.
Radiological evaluation should be done with plain x-rays of the affected part in AP, lateral, and both oblique views (45 degrees internal and external views). In majority of patients this will get the accurate diagnosis of nonunion and its subtype. CT scan is a more accurate modality than plain x-rays in diagnosing the non-union.(34)
Infection should be cause in all cases of femoral non-union unless ruled out. Hence proper blood work-up is must which should include complete blood count, ESR and CRP. Deep tissue culture at the time of secondary surgery is the gold standard for diagnosis of infection. (35)
Causes and Risk factors
Main causes of distal femoral nonunion are
Inadequate fracture stabilization leading to motion at fracture site
Avascularity at the fracture ends – due to compound fractures, excessive stripping of soft tissue during surgery
Fracture gap
Infection
Patient related
Surgeon related
Inadequate fracture stabilization leads to micro and macro movements at the fracture site, which may result due to inadequate fixation at the time of primary surgery or due to implant failure.
Avascularity or diminished blood supply to the fracture end results due to compound injury (27), excessive stripping of soft tissue during surgery, comminuted fractures.(36) Decreased blood supply leads to a poor healing response and causes atrophic non-union.
Multiple literature supports that in fractures with significant comminution the soft tissue stripping is more and thus injuring the blood supply.(28)
Presence of gap at the fracture site either due to bone loss or during surgery (fracture fixed in distraction or debridement) also contribute to the occurrence of non-union.(29) Any gap present is usually bridged by the fracture callus, but when the body fails to bridge this gap non union results.
Infection can result as a complication of open injury or surgical treatment. Infection leads to formation of dead necrotic bone in the form of sequestrum, ingrowth of infected granulation tissue, osteolysis and motion at fracture site due to loosening of implant or implant failure.
Patient factors like age, smoking, tobacco use, chronic use of analgesics (NSAIDs), medical comorbidities and obesity to name a few can lead to non-union (22, 37).
Surgeon related factors include technical factors like plate length, screw density of plate, material of implant (titanium vs. stainless steel) and cortical reduction. Studies have shown that use of titanium implants significantly reduces the chances of non-union and thus need for a secondary surgical procedure (22).
In case of implant failure, the most important factor is the length of plate used. Shorter plates are prone to fail earlier than longer plates due to relatively lower fatigue properties because of mechanical disadvantage. Usually, a plate with 9 or more screws are is less liable to give away (37).
Treatment Options
Ultimate aim of the surgeon is to achieve osseous union without complications. Along with this it is important for the surgeon to correct any mal-alignment control infection if present, achieving sufficient muscle strength and rehabilitation.
Currently the accepted method of primary fixation of distal femur fractures is retrograde nail and lateral plating either lateral locked plates or fixed angle plates.
1. Nail dynamisation
2. Exchange nailing
3. Plate osteosynthesis
4. External fixation
5. Adjuvant treatment options
a. Electrical stimulation and ultrasound therapy
b. Bone grafting
c. Bone graft substitutes and biologic agents
d. Bone marrow infiltration
Nail Dynamisation
Nail dynamisation is the term used when the statically locked nail is converted to a dynamically locked plate. This is accomplished by removal of screw/s adjacent to the dynamic hole of the nail.
Mechanism of healing with this technique is that it allows for a controlled axial instability of the bone and implant at the fracture site. This allows transfer of weight bearing forces to non-union site and promotes healing.(38)
Dynamisation is most effective when done at an early stage of non-union or delayed union as judged by serial radiographs. Optimal time for dynamisation is around 3-6 months of injury and primary treatment.(36)
Available literature suggests a success rate of about 50%. Nail dynamisation should be done is axially stable fractures like transverse or oblique fractures.
There are few complications associated with this technique namely shortening, implant failure. Thus a regular follow-up of the patients is a must.
Exchange Nailing
Exchange nailing refers to the surgical technique where an already present nail is removed and a larger diameter and stiffer nail is inserted after reaming. It is desirable that the second nail should be atleast 1-2mm larger than the earlier nail and the reaming should be done until the osseous chatter is heard.
This method provides both mechanical and biological stimulus for healing. A larger diameter and stiffer nail provides more mechanical stability along with increased working length of the implant thus decreasing the chances of implant failure. Biologically reaming causes deposition of fresh marrow material in the non-union site and stimulates periosteal reaction.(39) Union rates reported with this technique is variable with some studies showing union rates as high as 97%. (31, 32) Studies show that chances of non-union are more when reaming is not done.(40)
Plate Osteosynthesis
Plate osteosynthesis is the most common and gold standard treatment option in cases of distal femoral non-unions.(37) Plating offers increased mechanical stability to fracture specially in hypertrophic non-unions. Plate osteosynthesis (open reduction and internal fixation) provides an excellent opportunity of the surgeon to correct any associated deformities along with providing an excellent axial and torsional stability. Traditionally fixed angled 95 degree angled blade plate was used for distal femoral fractures, applied on the lateral aspect.(3, 41) The newer locked plates now available are the implant of choice in present scenario.(4, 5, 11-13, 15, 16, 18-20, 42, 43) With the use of compression holes excellent direct compression of the fracture site can be achieved.(44)
Few studies have reported union rates for distal femur non-unions with plate osteosynthesis around 91% to 100%.(45, 46) Even in case of poor bone stock and long standing non-unions the union rates are in range of 95 to 98% (31, 47)
This method of achieving union has its own risks and disadvantages. There is increased risk of infection, blood loss, increased tissue stripping, implant breakage, screw loosening etc. (6, 45, 47-50). Another disadvantage is that patients treated with plate osteosynthesis require strict immobilization for some duration, which may lead to joint stiffness and decreased range of motion of joints along with delay in starting rehabilitation.
Abdel-Aa et al (46) reported in their study that about 13% of patients treated with plate osteosynthesis for distal femoral non union required quadricepsplasty and knee arthrolysis within one year of surgery.
Another technique has been described in literature where both nail and plate are used simultaneously in achieving union. In this technique with an intramedullary implant in situ, a plate is fixed in compression mode at the fracture site. This method provides positive points of both the techniques in the form of early weight bearing, fracture fixed in direct compression thus chances of early union, improved torsional and rotational stability. If required bone grafting can also be done at same time to further increase the osteogenic potential and to fill up any bony defects if present. In studies using this method there has been a union rate of 100% within one year of surgery.(49, 51, 52)
External Fixation
Multiplanar (Ilizarov technique) and uniplanar external fixation for treatment of non-union of femur has been reported in literature with modest success (53, 54). Compression and distraction at non-union site has been demonstrated to show signs of healing(55). However, with the high complication rate (eg osteomyletitis, severe pain requiring opiod anagesics, septic arthritis, pin failure, joint stiffness etc.) use of external fixation for non-union healing is restricted to small number of patients. Along with this, the technical complexity and cost factor also restricts its use to tertiary level centres (54).
Adjuvant Treatment
These treatment options can be used as an isolated treatment option or as a supplementary treatment for achieving union.
Electrical Stimulation
Multiple studies show that mechanical forces, electrical forces, magnetic forces and ultrasound waves have variable level of effect on bone healing and growth (56-59). Electrical stimulation is thought to be effective non-invasive modality for promoting fracture healing and in treatment of non-unions.
Generation of electrical potentials around bone occurs when mechanical stress is applied(60, 61). Electronegative and electropositive potentials are generated with compression and tension respectively (62). It has been proven that in electronegative potential bone growth occurs and with electropositive potential bone is resorbed (63).
There are three techniques of electrical stimulation, namely, direct electric current, capacitive coupling and inductive coupling.
Direct electrical current is an invasive technique involving one or more cathode electrodes being implanted in the bone and an anode usually placed on the skin over the fracture site(64). In a case series by Brighton et al. (65) out of 168 fractures, 76% showed good bony union by 12 weeks of electrical stimulation therapy.
Capacitive coupling is a noninvasive technique where two electrodes are placed over the skin such that fracture site lies in between the electrodes. Here alternating current (AC) is used and an electric field is generated in and around the fracture site. It is a dose dependent technique whereby the greater electrical field leads to more osteoblastic cell response along with increased time of exposure leading to increased osteoblastic cell proliferation (66, 67).
Inductive coupling uses the principle of Pulsed Electromagnetic Field (PEMF) generation using specific device. The device is placed over the skin (non-invasive) over the fracture site. Passing current in the device generates the magnetic field. This magnetic field induces an electrical field, which leads to a bone healing response. This time-varying electrical field simulates normal response of osteoblastic cells to mechanical stimuli (68).
Bone Grafting, bone marrow aspirate and biologic agents
These procedures and materials can be used as an isolated or adjuvant treatment depending of the non-union type.
Autogenous bone grafts are considered gold standard for grafting procedures(69). Autologous bone grafting in past has got a bad review mainly due to donor site complications(70). With advances in harvesting techniques there is a renewed interest in this procedure(71-73).
Biologic agents like Bone Morphogenic Proteins (BMP) have been studied in detail both in animals and in humans and gives promising results.
Bone Morphogenic Proteins are part of the Transforming Growth Factor-Beta (TGF-B) superfamily and with a cascade sequence of events leads to bone healing via chondrogenesis, osteogenesis, angiogenesis and extracellular matrix remodeling (74). There are more than 20 BMP identified in humans. Studies in animals and in-vitro have shown BMP -2,4,6,7,9 have high osteogenic potential (75-78). Recombinant BMP-2 and 4 are in use clinically (74) but with questionable safety and efficacy profile(79-82).
Summary
Every surgically managed fracture is a race between bony union and implant/biological failure leading to non-union. Management of acute distal femur fracture with a nail or plate has good union rate or more than 90%. But when non-union occurs, it becomes a challenging task for the surgeon and patient both. It presents a significant mental, emotional and financial implication on the patient and his/her family.
Careful history taking and meticulous examination during routine follow-ups can help a surgeon to diagnose a delayed union or non-union in early stage and can modify the management as per the need to achieve bony union. Established non-union requires a well planned out management protocol to be decided before hand. Surgeon should decide the management plan (either non-invasive or invasive) on case-to-case basis to achieve union, correction of deformities. Surgeon should also take care of the patient modifiable risk factors like use of NSAIDs, smoking, medical co-morbidities and nutritional status of patient.
References
1. Zlowodzki M, Bhandari M, Marek DJ, Cole PA, Kregor PJ. Operative treatment of acute distal femur fractures: systematic review of 2 comparative studies and 45 case series (1989 to 2005). J Orthop Trauma. 2006;20(5):366-71.
2. Davison BL. Varus collapse of comminuted distal femur fractures after open reduction and internal fixation with a lateral condylar buttress plate. American journal of orthopedics. 2003;32(1):27-30.
3. Merchan ECR, Maestu PR, Blanco RP. Blade-Plating of Closed Displaced Supracondylar Fractures of the Distal Femur with the AO System. The Journal of Trauma: Injury, Infection, and Critical Care. 1992;32(2):174-8.
4. Haidukewych G. Results of Polyaxial Locked-Plate Fixation of Periarticular Fractures of the Knee. The Journal of Bone and Joint Surgery (American). 2007;89(3):614.
5. Kregor PJ, Stannard JA, Zlowodzki M, Cole PA. Treatment of Distal Femur Fractures Using the Less Invasive Stabilization System. Journal of Orthopaedic Trauma. 2004;18(8):509-20.
6. Vallier HA, Hennessey TA, Sontich JK, Patterson BM. Failure of LCP Condylar Plate Fixation in the Distal Part of the Femur: A Report of Six Cases. The Journal of Bone & Joint Surgery. 2006;88(4):846-53.
7. Thomson AB, Driver R, Kregor PJ, Obremskey WT. Long-Term Functional Outcomes After Intra-Articular Distal Femur Fractures: Orif Versus Retrograde Intramedullary Nailing. Orthopedics. 2008;31(8):748-50.
8. Handolin L, Pajarinen J, Lindahl J, Hirvensalo E. Retrograde intramedullary nailing in distal femoral fractures—results in a series of 46 consecutive operations. Injury. 2004;35(5):517-22.
9. Hartin NL, Harris I, Hazratwala K. RETROGRADE NAILING VERSUS FIXED-ANGLE BLADE PLATING FOR SUPRACONDYLAR FEMORAL FRACTURES: A RANDOMIZED CONTROLLED TRIAL. ANZ J Surg. 2006;76(5):290-4.
10. Singh SK, El-Gendy KA, Chikkamuniyappa C, Houshian S. The retrograde nail for distal femoral fractures in the elderly: High failure rate of the condyle screw and nut. Injury. 2006;37(10):1004-10.
11. Syed AA, Agarwal M, Giannoudis PV, Matthews SJE, Smith RM. Distal femoral fractures: long-term outcome following stabilisation with the LISS. Injury. 2004;35(6):599-607.
12. Ricci AR, Yue JJ, Taffet R, Catalano JB, DeFalco RA, Wilkens KJ. Less Invasive Stabilization System for treatment of distal femur fractures. American journal of orthopedics. 2004;33(5):250-5.
13. Fankhauser F, Gruber G, Schippinger G, Boldin C, Hofer H, Grechenig W, et al. Minimal-invasive treatment of distal femoral fractures with the LISS (Less Invasive Stabilization System) A prospective study of 30 fractures with a follow up of 20 months. Acta Orthopaedica. 2004;75(1):56-60.
14. Schutz M, Muller M, Kaab M, Haas N. Less invasive stabilization system (LISS) in the treatment of distal femoral fractures. Acta chirurgiae orthopaedicae et traumatologiae Cechoslovaca. 2003;70(2):74-82.
15. Schütz M, Müller M, Regazzoni P, Höntzsch D, Krettek C, Van der Werken C, et al. Use of the Less Invasive Stabilization System (LISS) in patients with distal femoral (AO33) fractures: a prospective multicenter study. Arch Orthop Trauma Surg. 2005;125(2):102-8.
16. Weight M, Collinge C. Early Results of the Less Invasive Stabilization System for Mechanically Unstable Fractures of the Distal Femur (AO/OTA Types A2, A3, C2, and C3). Journal of Orthopaedic Trauma. 2004;18(8):503-8.
17. Wong M-K, Leung F, Chow SP. Treatment of distal femoral fractures in the elderly using a less-invasive plating technique. International Orthopaedics (SICOT). 2005;29(2):117-20.
18. Ricci WM, Loftus T, Cox C, Borrelli J. Locked Plates Combined With Minimally Invasive Insertion Technique for the Treatment of Periprosthetic Supracondylar Femur Fractures Above a Total Knee Arthroplasty. Journal of Orthopaedic Trauma. 2006;20(3):190-6.
19. Kolb W, Guhlmann H, Windisch C, Marx F, Kolb K, Koller H. Fixation of Distal Femoral Fractures With the Less Invasive Stabilization System: A Minimally Invasive Treatment With Locked Fixed-Angle Screws. The Journal of Trauma: Injury, Infection, and Critical Care. 2008;65(6):1425-34.
20. Kao FC, Tu YK, Su JY, Hsu KY, Wu CH, Chou MC. Treatment of Distal Femoral Fracture by Minimally Invasive Percutaneous Plate Osteosynthesis: Comparison Between the Dynamic Condylar Screw and the Less Invasive Stabilization System. The Journal of Trauma: Injury, Infection, and Critical Care. 2009;67(4):719-26.
21. Fulkerson E, Tejwani N, Stuchin S, Egol K. Management of periprosthetic femur fractures with a first generation locking plate. Injury. 2007;38(8):965-72.
22. Rodriguez EK, Boulton C, Weaver MJ, Herder LM, Morgan JH, Chacko AT, et al. Predictive factors of distal femoral fracture nonunion after lateral locked plating: a retrospective multicenter case-control study of 283 fractures. Injury. 2014;45(3):554-9.
23. Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh JL. Locking Plates for Distal Femur Fractures: Is There a Problem With Fracture Healing? Journal of Orthopaedic Trauma. 2011;25:S8-S14.
24. Brinker MR. Nonunions: Evaluation and Treatment. In: Trafton PG, editor. Skeletal Trauma: Basic Science, Management, and Reconstruction. 3 ed. Philadelphia: W.B. Saunders; 2003. p. 507-604.
25. Furlong AJ, Giannoudis PV, DeBoer P, Matthews SJ, MacDonald DA, Smith RM. Exchange nailing for femoral shaft aseptic non-union. Injury. 1999;30(4):245-9.
26. Giannoudis PV, MacDonald DA, Matthews SJ, Smith RM, Furlong AJ, De Boer P. Nonunion of the femoral diaphysis. The Journal of Bone and Joint Surgery. 2000;82(5):655-8.
27. Malik MH, Harwood P, Diggle P, Khan SA. Factors affecting rates of infection and nonunion in intramedullary nailing. The Journal of bone and joint surgery British volume. 2004;86(4):556-60.
28. Noumi T, Yokoyama K, Ohtsuka H, Nakamura K, Itoman M. Intramedullary nailing for open fractures of the femoral shaft: evaluation of contributing factors on deep infection and nonunion using multivariate analysis. Injury. 2005;36(9):1085-93.
29. Pihlajamäki HK, Salminen ST, Böstman OM. The Treatment of Nonunions Following Intramedullary Nailing of Femoral Shaft Fractures. Journal of Orthopaedic Trauma. 2002;16(6):394-402.
30. Wu C-C. The Effect of Dynamization on Slowing the Healing of Femur Shaft Fractures after Interlocking Nailing. The Journal of Trauma: Injury, Infection, and Critical Care. 1997;43(2):263-7.
31. Kempf I, Grosse A, Rigaut P. The Treatment of Noninfected Pseudarthrosis of the Femur and Tibia with Locked Intramedullary Nailing. Clinical Orthopaedics and Related Research. 1986;&NA;(212):142???54.
32. Webb LX, Winquist RA, Hansen ST. Intramedullary Nailing and Reaming for Delayed Union or Nonunion of the Femoral Shaft. Clinical Orthopaedics and Related Research. 1986;&NA;(212):133???41.
33. Weresh MJ, Hakanson R, Stover MD, Sims SH, Kellam JF, Bosse MJ. Failure of Exchange Reamed Intramedullary Nails for Ununited Femoral Shaft Fractures. Journal of Orthopaedic Trauma. 2000;14(5):335-8.
34. Bhattacharyya T, Bouchard KA, Phadke A, Meigs JB, Kassarjian A, Salamipour H. The Accuracy of Computed Tomography for the Diagnosis of Tibial Nonunion. The Journal of Bone & Joint Surgery. 2006;88(4):692-7.
35. Gristina AG, Naylor PT, Webb LX. Molecular mechanisms in musculoskeletal sepsis: the race for the surface. Instructional course lectures. 1990;39:471-82.
36. Lynch JR, Taitsman LA, Barei DP, Nork SE. Femoral Nonunion: Risk Factors and Treatment Options. J Am Acad Orthop Surg. 2008;16(2):88-97.
37. Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ. Risk Factors for Failure of Locked Plate Fixation of Distal Femur Fractures. Journal of Orthopaedic Trauma. 2014;28(2):83-9.
38. Yokota H, Tanaka SM. Osteogenic potentials with joint-loading modality. J Bone Miner Metab. 2005;23(4):302-8.
39. Reichert ILH, McCarthy ID, Hughes SPF. The Acute Hemodynamic Response to Intramedullary Reaming of the Intact and Osteotomized Tibia: An Experimental Investigation with Radiolabeled Microspheres in the Ovine Tibia. Techniques in Orthopaedics. 1996;11(1):28-34.
40. Society COT. Nonunion following intramedullary nailing of the femur with and without reaming: Results of amulticenter randomized clinical trial. The Journal of bone and joint surgery American volume. 2003;85-A(11):2093-6.
41. Bolhofner BR, Carmen B, Clifford P. The Results of Open Reduction and Internal Fixation of Distal Femur Fractures Using a Biologic (Indirect) Reduction Technique. Journal of Orthopaedic Trauma. 1996;10(6):372-7.
42. Kayali C, Agus H, Turgut A. Successful results of minimally invasive surgery for comminuted supracondylar femoral fractures with LISS: comparative study of multiply injured and isolated femoral fractures. Journal of Orthopaedic Science. 2007;12(5):458-65.
43. Liu F, Tao R, Cao Y, Wang Y, Zhou Z, Wang H, et al. The role of LISS (less invasive stabilisation system) in the treatment of peri-knee fractures. Injury. 2009;40(11):1187-94.
44. Meyer RW, Plaxton NA, Postak PD, Gilmore A, Froimson MI, Greenwald AS. Mechanical Comparison of a Distal Femoral Side Plate and a Retrograde Intramedullary Nail. Journal of Orthopaedic Trauma. 2000;14(6):398-404.
45. Bellabarba C, Ricci WM, Bolhofner BR. Results of Indirect Reduction and Plating of Femoral Shaft Nonunions After Intramedullary Nailing. Journal of Orthopaedic Trauma. 2001;15(4):254-63.
46. Abdel-Aa AM, Farouk OA, Elsayed A, Said HG. The Use of a Locked Plate in the Treatment of Ununited Femoral Shaft Fractures. The Journal of Trauma: Injury, Infection, and Critical Care. 2004;57(4):832-6.
47. Ring D, Jupiter JB, Sanders RA, Quintero J, Santoro VM, Ganz R, et al. Complex Nonunion Of Fractures Of The Femoral Shaft Treated By Wave-plate Osteosynthesis. The Journal of Bone and Joint Surgery. 1997;79(2):289-94.
48. Rozbruch RS, M??ller U, Gautier E, Ganz R. The Evolution of Femoral Shaft Plating Technique. Clinical Orthopaedics and Related Research. 1998;354:195-208.
49. Ueng SWN, Chao E-K, Lee S-S, Shih C-H. Augmentative Plate Fixation for the Management of Femoral Nonunion after Intramedullary Nailing. The Journal of Trauma: Injury, Infection, and Critical Care. 1997;43(4):640-4.
50. Cove JA, Lhowe DW, Jupiter JB, Siliski JM. The Management of Femoral Diaphyseal Nonunions. Journal of Orthopaedic Trauma. 1997;11(7):513-20.
51. Ueng SWN, Shih C-H. Augmentative Plate Fixation for the Management of Femoral Nonunion with Broken Interlocking Nail. The Journal of Trauma: Injury, Infection, and Critical Care. 1998;45(4):747-52.
52. Choi YS, Kim KS. Plate augmentation leaving the nail in situ and bone grafting for non-union of femoral shaft fractures. Int Orthop. 2005;29(5):287-90.
53. Brinker MR, O’Connor DP. Ilizarov Compression Over a Nail for Aseptic Femoral Nonunions That Have Failed Exchange Nailing: A Report of Five Cases. Journal of Orthopaedic Trauma. 2003;17(10):668-76.
54. Patil S. Management of complex tibial and femoral nonunion using the Ilizarov technique, and its cost implications. Journal of Bone and Joint Surgery – British Volume. 2006;88-B(7):928-32.
55. Inan M, Karaoglu S, Cilli F, Turk CY, Harma A. Treatment of Femoral Nonunions by Using Cyclic Compression and Distraction. Clinical Orthopaedics and Related Research. 2005;&NA;(436):222-8.
56. Fukada E, Yasuda I. On the Piezoelectric Effect of Bone. Journal of the Physical Society of Japan. 1957;12(10):1158-62.
57. Duarte LR. The stimulation of bone growth by ultrasound. Archives of Orthopaedic and Traumatic Surgery. 1983;101(3):153-9.
58. Kenwright AGaJ. The influence of induced micromovement upon the healing of experimental tibial fractures. Bone & Joint Journal. 1985;67-B:650-5.
59. Valchanou VD, Michailov P. High energy shock waves in the treatment of delayed and nonunion of fractures. International Orthopaedics. 1991;15(3).
60. Becker RO, Bassett, C.A.L., Bachman, C.H. Bioelectric factors controlling bone structure. In: Frost H, editor. Bone biodynamics. Boston: Little, Brown & Company; 1964. p. 209–32.
61. Yasuda I. Fundamental aspects of fracture treatment. J Kyoto Med SOC. 1953;4:392.
62. Otter M, Goheen S, Williams WS. Streaming potentials in chemically modified bone. Journal of Orthopaedic Research. 1988;6(3):346-59.
63. Rubinacci A, Black J, Brighton CT, Friedenberg ZB. Changes in bioelectric potentials on bone associated with direct current stimulation of osteogenesis. Journal of Orthopaedic Research. 1988;6(3):335-45.
64. Black J. Electrical Stimulation: Its Role in Growth, Repair, and Remodeling of the Musculoskeletal
System. New York: Praeger; 1987.
65. Brighton CT, Black J, Friedenberg ZB, Esterhai JL, Day LJ, Connolly JF. A multicenter study of the treatment of non-union with constant direct current. The Journal of bone and joint surgery American volume. 1981;63(1):2-13.
66. Korenstein R, Somjen D, Fischler H, Binderman I. Capacitative pulsed electric stimulation of bone cells. Induction of cyclic-AMP changes and DNA synthesis. Biochimica et Biophysica Acta (BBA) – Molecular Cell Research. 1984;803(4):302-7.
67. Wang Z. Up-Regulation of Bone Morphogenetic Proteins in Cultured Murine Bone Cells with Use of Specific Electric Fields. The Journal of Bone and Joint Surgery (American). 2006;88(5):1053.
68. Nelson FR, Brighton CT, Ryaby J, Simon BJ, Nielson JH, Lorich DG, et al. Use of physical forces in bone healing. J Am Acad Orthop Surg. 2003;11(5):344-54.
69. Giannoudis PV, Dinopoulos HT. Autologous bone graft: when shall we add growth factors? Foot Ankle Clin. 2010;15(4):597-609.
70. Oakley MJ, Smith WR, Morgan SJ, Ziran NM, Ziran BH. Repetitive posterior iliac crest autograft harvest resulting in an unstable pelvic fracture and infected non-union: case report and review of the literature. Patient Saf Surg. 2007;1(1):6.
71. Newman JT, Stahel PF, Smith WR, Resende GV, Hak DJ, Morgan SJ. A New Minimally Invasive Technique for Large Volume Bone Graft Harvest for Treatment of Fracture Nonunions. Orthopedics. 2008;31(3):257-61.
72. Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: A systematic review. Injury. 2011;42:S3-S15.
73. Herscovici JD, Scaduto JM. Use of the reamer-irrigator-aspirator technique to obtain autograft for ankle and hindfoot arthrodesis. The bone & joint journal. 2012;94-B(1):75-9.
74. Lissenberg-Thunnissen SN, de Gorter DJ, Sier CF, Schipper IB. Use and efficacy of bone morphogenetic proteins in fracture healing. Int Orthop. 2011;35(9):1271-80.
75. Xiang L, Liang C, Zhen-Yong K, Liang-Jun Y, Zhong-Liang D. BMP9-induced osteogenetic differentiation and bone formation of muscle-derived stem cells. J Biomed Biotechnol. 2012;2012:610952.
76. Kang Q, Sun MH, Cheng H, Peng Y, Montag AG, Deyrup AT, et al. Characterization of the distinct orthotopic bone-forming activity of 14 BMPs using recombinant adenovirus-mediated gene delivery. Gene Ther. 2004;11(17):1312-20.
77. Luu HH, Song WX, Luo X, Manning D, Luo J, Deng ZL, et al. Distinct roles of bone morphogenetic proteins in osteogenic differentiation of mesenchymal stem cells. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2007;25(5):665-77.
78. Cheng H, Jiang W, Phillips FM, Haydon RC, Peng Y, Zhou L, et al. Osteogenic activity of the fourteen types of human bone morphogenetic proteins (BMPs). Urologic Oncology: Seminars and Original Investigations. 2004;22(1):79-80.
79. Burks MV, Nair L. Long-Term Effects of Bone Morphogenetic Protein- Based Treatments in Humans. Journal of Long-Term Effects of Medical Implants. 2010;20(4):277-93.
80. Carragee EJ, Hurwitz EL, Weiner BK. A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned. Spine J. 2011;11(6):471-91.
81. Carragee EJ, Ghanayem AJ, Weiner BK, Rothman DJ, Bono CM. A challenge to integrity in spine publications: years of living dangerously with the promotion of bone growth factors. Spine J. 2011;11(6):463-8.
82. Mroz TE, Wang JC, Hashimoto R, Norvell DC. Complications related to osteobiologics use in spine surgery: a systematic review. Spine (Phila Pa 1976). 2010;35(9 Suppl):S86-104.
Dr. Pramod Maheshwari
Dr. Puneet Maheshwari
(Abstract) (Full Text HTML) (Download PDF)
How to Avoid local Complications during Primary and Revision surgery of Trochanteric fractures: Advices and Tricks for operation tactics and Trouble-shooting
/in July Sep | Volume 1 | Issue 1Vol 1 | Issue 1 | July – Sep 2015 | page: 21-24 | Andreas Heinrich Hugo Tiemann[1], Ralf Herbert Gahr[2] .
Author: Andreas Heinrich Hugo Tiemann[1], Ralf Herbert Gahr[2].
[1]SRH Zentralklinikum Suhl, Medical Director,Albert-Schweitzer-Str. 2 ,98527 Suhl.
[2]Klinikum St. Georg Leipzig, Delitzscher Str. 141, 04129 Leipzig.
Address of Correspondence
Dr Ralf Herbert Gahr
Klinikum St. Georg Leipzig
Delitzscher Str. 141, 04129 Leipzig
Email: ralfgahr@sanktgeorg.de
Abstract
Background: Hip fractures belong to the most frequent fractures of elderly people. The treatment follows a specific algorithm that focuses on the medical as well as the social situation of these patients. Despite modern operative techniques and implants complications may occur. They may be distinguished into two groups: local complications and systemic complications
Especially local complications (cut out of the femoral head screw) are the reason for revision surgery. Surgery (“salvage procedures”) may only be performed after critical analysis of the local situation and individual planning of the revision procedure. This article outlines the tactical course of action in these cases.
Keywords: Hip fractures – complication – salvage procedure – therapeutic algorithm.
Introduction
Hip fractures are typical injuries of the elderly [1]. Recent studies prove that the incidence of these entities rises dramatically with increasing age [1]. In 2008 Lohmann et al. showed an incidence of 0.06 percent at an age between 60 and 64 years and an incidence of 1.3 percent at people at their eighties [2]. In other words: More than 90 percent of the patients are in their seventies and in addition more than 70 percent are females [3].
American authors assume, that the number of hip fractures will increase from 250,000 in the year 1990 up to 500,000 in 2040 [4]. In Germany the rate of hip fractures totals up to 90/100.000 inhabitants for all classes of age but is 966/100.000 for septuagenarians [5, 6]. Till 2050 the incidence is assumed to multiply by five [6].
In case of geriatric patients suffering from a hip fracture leads to a significant decrease of life expectancy accompanied by an increased medical risk and a number of social problems (for example accommodation in a retirement home) [7, 8]. Anglo-American analyses indicate an average reduction of life expectancy of 1.8 years or 25 percent of the remaining life span per patient [9]. The treatment of such injuries demands a specific algorithm that takes the local surgical problems and co-morbidities as well as social necessities into consideration. Highest goal of the surgical treatment is the early mobilization, prevention of secondary complications and the return to maximal autonomy. Hip fractures today are regularly treated by operative stabilization [10]. Nevertheless the ideal operative procedure is still discussed in the literature [11].
Even modern operative techniques and implants these procedures show adverse events or complications in 15 to 20 percent [12, 13]. Based on acuteness, topography and implant association they may be distinguished into the following groups [14]:
A. Acuteness
Early complication (within three months after surgery)
tactical surgical failure
technical surgical failure
local complication (like wound healing disturbance or infection)
systemic complications (like deep vein thrombosis)
Late complication (after more than three months postoperatively)
effect of poor bone biology (like delayed union or pseudarthrosis)
contracture
b.Topography
local complication (see above)
systemic complication (see above)
c. Implant association
implant associated complication (like cutout, peri-implant fracture or implant failure); (see below)
non implant associated complication
(Revision) Surgery: Planning and tactics
In reference to the special situation of aged patients one has to pay attention to two central factors no matter if one performs primary or revision surgery:
· short term operation
· full weight bearing possible after surgery
Thus the planning of surgery must be focused on the prevention of tactical and technical failures. Revision surgery necessary because of local complications may be divided into two groups:
· Implant (osteosynthesis) related procedures.
Planned implant replacement (for example progressive coxarthrosis that leads to removal of an intramedullary stabilization system in order to implant a total hip arthoplasty).
Enforced implant replacement based on local complications (salvage procedures)
Not implant related local surgery (like the relief of a local hematoma).
A strict separation between these two types of complications is not always possible in praxi. Based on the above named principles one has to keep in mind the following general standards [15]:
· On the part of the surgical procedure:
o full weight bearing possible after surgery
o stable implant fixation in osteoporotic bone
o preservation of the vascularization of the femoral neck and head
o simple operative technique
· On the part of the surgeon:
o profound knowledge of possible implants and surgical techniques
o mastery of the intramedullary and extramedullary surgical options as well as of arthroplasties
oclear Nevertheless the different studies still show different results indication for a specific implant.
Key-factor I: Preoperative analysis (Fig. 1 and 2)
Primary surgery as well as revision surgery demands a proper analysis of the local situation. The following questions have to be answered preoperatively [15]:
·Where is the problem localized (femoral head and/or femoral neck, trochanteric region, subtrochanteric)?
·Why did the complication occur?
·How may the problem be solved (reosteosynthesis versus (hemi) arthroplasty)?
·What is the correct implant?
·When is the optimal point in time for the operation?
Key-factor II: Osteosynthesis or arthroplasty (Fig. 3)?
In order to answer these questions the following factors are important:
Is the actual situation generally applicable to be treated with an osteosynthesis?
o from the part of the fracture
o from the part of the hip joint (i.e. presence of a significant symptomatic coxathrosis)
If the answer to this question is YES: Which technique will be performed?
o intramedullary stabilization
oextramedullary stabilization
If the answer to this question is NO: Which alternative technique should be performed (hemiarthroplasty, total arthroplasty) [16, 17, 18, 19]?
Stable fractures (AO/OTA 31-A1) present the classic indication for osteosynthesis. The cure rate is close to 100 percent [20]. These fractures mainly are stabilized by the use of a dynamic hip screw (DHS).
AO/OTA A31-A2 and –A3 are unstable fractures. The optimal treatment is still open to debate in the recent literature [16, 17]. Intramedullary stabilization is considered to be better in terms of biomechanical considerations [21]. Nevertheless osteosynthesis failure is estimated to be 56 percent [20].
The question whether to perform reosteosynthesis or switch to hip arthroplasty is elaborated just by few studies. The different studies show different results. Nevertheless Faldini 2002, Sinno 2007 and Giannotti 2013 and 2014 indicate, that elder patients suffering from those unstable pertrochanteric fractures benefit from treatment by cemented hemiarthoplasty. This leads to faster mobilization and lower mortality [16, 17, 18, 19]. According to D`Arrigo et al. the candidates for proximal femur replacement are patients with non-viable proximal femoral segments, destruction of the proximal femoral articular surface, advanced age and the absence of coxarthrosis [22]. Total arthroplasty may be taken into consideration in case of patients with additional severe coxarthrosis.
Switching from internal fixation to arthoplasty offers some special problems [22]:
· failed internal fixation (sometimes accompanied by broken screws) must be removed
· necessity of special instruments in order to remove the failed system
· compromised proximal femur with bone loss distal to the typical neck-resection level for hip arthroplasty
Key-factor III: Open or closed reduction (Table 1)?
The preoperative fracture analysis with a view to it`s reductive capacity based on the radiographic findings (X-ray, CT-scan) is an integral component as well for primary surgery as for revision surgery when reosteosynthesis seams to be possible. Open and closed reduction is the typical approach. Normally AO/OTA 31 fractures will be closed reduced. However between three and 17 percent are estimated to be applicative for closed reduction [23, 24, 25]. In their study Sharma et al. identified 4 general fracture situations, which are not applicative for closed reduction [25]:
· AO/OTA 31-A1 fractures where the proximal fragment is locked underneath the overridden and mediatized shaft fragment
· AO/OTA 31-A1 fractures with bisected lesser trochanter
· AO/OTA 31-A2 fractures with entrapment of the posteromedial fragment at the fracture site
· AO/OTA 31-A2 fractures with an anteriorly displaced proximal fragment and an underlying separate lesser trochanter
The mentioned AO/OTA 31-A1 fractures mainly occurred in younger, the AO/OTA 31-A2 fractures in older patients.
Implant related specification of typical complications of osteosynthesis
In case of planned (re-) osteosynthesis knowledge of the specific osteosynthesis related complications is vital in order to avoid local surgical complications. In general the complication rate is estimated to be three percent [26]. Sathiyakumar et al. distinguished five different treatment variant with significantly different typical implant related complications [9].
The complications mentioned below may occur after intramedullary stabilization as well as extramedullary stabilization of AO/OTA 31 fractures.
Particulars and choice of typical complications of extramedullary systems
The overall complication rate is estimated to be between 6.8 and 16.7 percent [27]. The rate of mechanical complications is estimated to be 2.8 percent [26].
Typical complications
· Cutout. Between three and 16.7 percent for dynamic hip screws [27, 28, 29].
· Z-effect. Mentioned below (intramedullary complications)
· Jamming of the lag screw. According to Simpson this is one of the main reasons for dynamic hip screw failure [30].
· Peri-implant fracture. Parker et al. found it in 0.1 percent in their 2010 study [27].
· Implant overload
· Implant dislocation
Particulars and choice of typical complications of intramedullary systems
The overall complication rate is estimated between 3.6 and 18 percent in the recent literature [26].
Typical complications
·Dislocation of the lesser trochanter
·Varus dislocation of the fracture
·Z-effect-A classical complication of two screw systems (like the proximal femoral nail). The repetitive axial loading of the implant combined with an unstable fracture fixation situation leads to toggling of the nail within the femoral canal [31]. This leads to medial migration of the nail. This mechanism is also described in the 2008 study of Weil et al. [32]. Nevertheless the precise etiology requires further clarification [33].
·Cutout. The Cochrane analysis of 2010 describes a rate of 3.4% for intramedullary implants [27]. The contemporary 2014 study of Greorgiannos evidences a rate between two and ten percent [34]. For intramedullary system as well as extramedullary ones the possibility of cutouts depends on the positioning of the lag or sliding screw in the proximal fragment [34]. As early as 1995 Baumgartner et al. described the so-called “tip-apex-distance” (TAD). This nowadays is accepted to be the central principle for the optimal positioning of the lag screw. It is determined intraoperative in the ap. and axial view fluoroscopy [35]. Kuzyk et al. showed in 2012 that the position of the lag screw next to the “Adam´s bow” in the ap. view and in the center of the proximal fragment in the axial view optimizes the biomechanical stability of the osteosynthesis [36]. In addition Nikoloski et al. could prove, that the original TAD rule should be modified depending on the used system, especially when “two screw systems” are used [37]. These authors distinguished two main types of cutout [37]:
o cephaled cutout
o axial cutout
· Knife effect
· Secondary screw dislocation
· Peri-implant fracture. Robinson et al. described an incidence of 18.74 fractures per 1000 person years in case of fractures treated with intramedullary systems [38]. The analysis of Parker et al. in 2010 showed an incidence of 2.6 percent [27]. By developing new designs of the intramedullary devices in the last decades the rate of these complication could be decreased dramatically.
· Implant failure
Discussion
Trochanteric femoral fractures comprise 50 percent of geriatric hip fractures. [39]. Although union rates as high as 100 percent have been reported after primary reduction and internal fixation with stable fractures ideal implants and optimal reduction failure rates over 50 percent are described in case of unstable fractures, suboptimal fracture fixation and poor bone quality [40]. Thus the correct individualized primary stabilization already presents a demanding problem. Appropriate management of failed primary osteosynthesis is even more challenging.
According to the recent literature the choice of treatment depends on the clear identification of the fracture type combined with the specific local situation [39]:
· AO/OTA classification of the fracture.
· radiographic analysis of the local bone structure
o presence or absence of osteoporosis
o presence or absence of extended bone loss
o presence or absence of significant coxarthrosis
When, based on the AO/OTA classification and the above-mentioned facts, the decision for internal (re-) fixation is made optimal reduction of the fracture fragments and positioning of the chosen implant is from central interest [35]. According to the recent literature implant failure generally seems to be the result of poor fracture reduction, mechanical stress, fracture instability or technical error [40] Although the optimal treatment for unstable fracture situations {AO/OTA 31-A2 and A3) are still discussed controversially in the last years a rising number of studies presents good results for arthroplasty as well for primary as for revision surgery [41,42]. Unfortunately there are only few comparative studies and even fewer prospective, random controlled ones which compare prosthetic hip replacement with the standard internal fixation in terms of primary and revision surgery [16]. In their 2014 study these authors come to the conclusion that there are no major differences between the treatment with hemi- or total arthroplasty but especially the elderly patients with severe osteoporosis or comminuted trochanteric fracture take significant profit from the treatment with hip arthroplasty compared to internal fixation [Giannotti]. According to Parker et al. in 2006 there are no significant differences between arthroplasty and internal fixation for mechanical complications, local wound complications, general complications and mortality at one year or long-term function [42].
Conclusion
· proximal hip fracture treatment is no trauma surgery for beginners
· local bone and fracture situation have to be clearly analyzed before taking one or the other surgical option into consideration
· primary stabilization as well as reoperations show specific pitfalls which may affect the outcome of any chosen treatment option significantly
· surgeons have to have profound knowledge about how to identify these pitfalls in order to avoid technical and tactical failure
especially in unstable fracture situations and in case of failed primary internal stabilization arthroplastic treatment should be a serious alternative.
References
1. Prokop A, Chmielnicki M. Pertrochantäre Femurfraktur – eine Anfängeraufgabe? Z Othop Unfall 2014; 152: 584-587
2. Lohmann R, Frerichmann U, Stöckle U et al. Proximal femoral fractures in the elderly. Analysis of data from health insurance providers on more than 23 Million insured persons – Part 1. Unfallchirurg 2007; 110: 603–609
3. Queally JM, Harris E, Handoll HH, Parker MJ. Intramedullary nails for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2014 Sep12;9:CD004961.
4. Gilbert TB, Hawkes WG, Hebel JR, Hudson JI, Kenzora JE, Zimmerman SI, Felsenthal G, Magaziner J. Spinal anesthesia versus general anesthesia for hip fracture repair: a longitudinal observation of 741 elderly patients during 2-year follow-up. Am J Orthop (Belle Mead NJ). 2000 Jan;29(1):25-35.
5. Bonnaire F et al. Versorgung proximaler Femurfrakturen. Unfallchirurg 2005; 108: 387 – 400
6. Bonnaire F et al. Behandlung von Schenkelhalsfrakturen. Chirurg 2008;: 595 – 611
7. Smektalla R et al. Zur Prognose der Schenkelhalsfraktur. Beurteilung der Mortalität nach Schenkelhalsfraktur durch sektorenübergreifende Datenzusammenführung. Unfallchirurg 2005; 108: 927 – 937
8. Smektalla R et al. Mediale Schenkelhalsfraktur: Einfluss des Versorgungszeitpunktes auf die Ergebnisqualität. Unfallchirurg 2010; 113: 287 – 292
9. Sathiyakumar V, Greenberg SE, Molina CS, Thakore RV, Obremskey WT, Sethi MK. Hip fractures are risky business: an analysis of the NSQIP data. Injury. 2015 Apr;46(4):703-8.
10. Egol KA et al. Perioperative considerations in geriatric patients with hip fracture: What is the evidence? J Orthop Trauma 2009; Vol 23, No 6: 386 – 394
11. Geiger F et al. Trochanteric fractures in the elderly: the influence of primary hip arthroplasty on 1-year mortality. Arch Orthop Trauma Surg 2007; 127: 959 – 966
12. Parker MJ et al. Hemiarthroplasty versus internal fixation for displaced intracapsular hip fractures: a long-term follow-up of a randomized trial. Injury 2010: 41(4): 370 – 373
13. Klinger HM et al. A comparative study of unstable per- and intertrochanteric femoral fractures treated with dynamic hip screw (DHS) and trochanteric bitt press plate vs. proximal femoral nail (PFN). Zentralblatt für Chirurgie 2005; 130(4): 301 -306
14. Huang HK et al. Displaced femoral neck fractures in young adults treated with closed reduction and internal fixation. Orthopedics 2010; 33(12): 873
15. Tiemann AHH, Hofmann GO. Osteosynthesen hüftgelenknaher Frakturen. Trauma und BK 2012;
16. Giannotti S, Bottai V, Dell’Osso G, De Paola G, Bugelli G, Guido G. The hip prosthesis in lateral femur fracture: current concepts and surgical technique. Clin Cases Miner Bone Metab. 2014 Sep;11(3):196-200.
17. Giannotti S, Bottai V, Pini E, Dell’osso G, De Paola G, Guido G. Clinical and surgical approach of severe bone fragility fracture: clinical case of 4 fragility fracture in patient with heavy osteoporosis. Clin Cases Miner Bone Metab. 2013 Jan;10(1):52-5.
18. Sinno K et al. The effectiveness of primary bipolar arthroplasty in treatment of unstable intertrochanteris fractures in elderly patients. N Am J Med Sci 2010; Dec; 2(12): 561 – 568
19. Faldini A. et al. Surgical treatment of intertrochanteric fractures by total hip arthroplasty in old osteoporotic patients. Scientific Exhibit At 69th AAOS annual Meeting 2002: 12 – 19
20. Haidukewych GJ, Israel TA, Berry DJ. Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am. 2001 May;83-A(5):643-50.
21. Schipper IB et al. Unstable trochanteric femoral fractures: extramedullary or intramedullary fixation? Review of literature. Injury 2004; Feb; 35(2): 142 – 151
22. D’Arrigo C, Perugia D, Carcangiu A, Monaco E, Speranza A, Ferretti A. Hip arthroplasty for failed treatment of proximal femoral fractures. Int Orthop. 2010 Oct;34(7):939-42.
23. Moehring HD, Nowinski GP, Chapman MW, Voigtlander JP. Irreducible intertrochanteric fractures of the femur. Clin Orthop Relat Res. 1997 Jun;(339):197-9.
24. Chun YS et al. Technique and early results of percutaneous reduction of sagittaly unstable intertrochanteric fractures. Clin Orthop Surg 2011; 3: 217 – 224
25. Sharma B et al. Pertrochanteric fractures (AO/OTA 31-A1 and A2) not amenable to closed reduction: Causes of irreducibility. Injury Int J Care Injured 2014; 45: 1950 – 1957
26. Tsang STJ et al. When does hip surgery fail? Injury Int J Care Injured 2014; 45: 1059 – 1065
27. Parker MJ et al. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures. Cochran Library Database System Rev 2010; 9: Dc000093.
28. Nordin S et al. Mechanical failure of dynamic hip screw (DHS) fixation in intertrochanteric fracture of the femur. Med J Malaysia 2001;56 (Suppl D): 12 – 17
29. Huseh KK et al. Risk factors in cutout of sliding hip screws in intertrochanteric fractures: an evaluation of 937 patients. Int Orthop 2010; 34(8): 1273 – 1276
30. Simpson F et al. Sliding hip screws: modes of failure. Injury 1989; 20(4): 227 – 231
31. Takasago T et al. Intrapelvic Migration of the lag screw in intramedullary nailing. Case Reports in Orthopedics 2014; Vol 2014, Article ID 519045;
32.Weil YA, Gardner MJ, Mikhail G, Pierson G, Helfet DL, Lorich DG. Medial migration of intramedullary hip fixation devices: a biomechanical analysis. Arch Orthop Trauma Surg. 2008 Feb;128(2):227-34.
33. Strauss EJ et al. The “Z-effect” phenomenon defined: a laboratory study. J Orthop Res. 2007; 25: 1568-1573.
34. Georgiannos D et al. Complications following treatment of trochanteric fractures with Gamma3 nail: Is the latest version of Gamma nail superior to its predecessor? Surgery Research and Practice 2014; Article ID 143598;
35. Baumgaertner MR et al. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. JBJS Am 1995; vol 77, no 7: 1058 – 1064
36. Kuzyk PR, Zdero R, Shah S, Olsen M, Waddell JP, Schemitsch EH. Femoral head lag screw position for cephalomedullary nails: a biomechanical analysis. J Orthop Trauma. 2012 Jul;26(7):414-21.
37. Nikoloski AN, Osbrough AL, Yates PJ. Should the tip-apex distance (TAD) rule be modified for the proximal femoral nail antirotation (PFNA)? A retrospective study. J Orthop Surg Res. 2013 Oct 17;8:35.
38. Robinson CM, Adams CI, Craig M, Doward W, Clarke MC, Auld J. Implant-related fractures of the femur following hip fracture surgery. J Bone Joint Surg Am. 2002 Jul;84-A(7):1116-22.
39. Murphy DK, Randell T, Brennan KL, Probe RA, Brennan ML. Treatment and displacement affect the reoperation rate for femoral neck fracture. Clin Orthop Relat Res. 2013 Aug;471(8):2691-702.
40. Carpintero P, Caeiro JR, Carpintero R, Morales A, Silva S, Mesa M. Complications of hip fractures: A review. World J Orthop. 2014 Sep 18;5(4):402-11.
41. Kiran Kumar GN et al. Bipolar Hemiarthroplasty in Unstable Intertrochanteric Fractures in elderly: A Prospective Study. J Clin Diagn Res. 2013 Aug; 7(8): 1669-1671
42. Sancheti Kh, Sancheti P, Shyam A, Patil S, Dhariwal Q, Joshi R. Primary hemiarthroplasty for unstable osteoporotic intertrochanteric fractures in the elderly: A retrospective case series. Indian J Orthop. 2010 Oct;44(4):428-3.
43. Parker MJ, Handoll HH. Replacement arthroplasty versus internal fixation for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2006 Apr 19;(2):CD000086.
(Abstract) (Full Text HTML) (Download PDF)
Management Options and Treatment Algorithm in Intertrochanteric Fractures
/in July Sep | Volume 1 | Issue 1Vol 1 | Issue 1 | July – Sep 2015 | page: 12-16 | Anoop C Dhamangaonkar [1]
Author: Anoop C Dhamangaonkar [1].
[1]Lokmanya Tilak Municipal Medical College and Lokmanya Tilak Municipal General Hospital,
Sion, Mumbai- 400022, India.
Address of Correspondence
Dr. Anoop C Dhamangaonkar
2/28,Madhavi Soc., Mogal Lane, Matunga (W), Mumbai-400016.India.
Email: anoopd_7@yahoo.com
Abstract
Background: Intertrochanteric (IT) fractures are one of the most common lower limb fractures. There are many varied treatment options to treat the same. Also, our basic understanding of IT fractures is improving leading to evolution of newer concepts which in turn is leading to designing of newer implants. In this sea of newer treatment options, are all newer implants merely market driven? The new- age orthopaedic surgeon needs to be made aware of the newer concepts of IT fractures, implant designs and also a comprehensive literature support of the various treatment options available like concept of unstable IT farcture, the dynamic hip screw (DHS) system, Medoff’s plate, DHS with a trochanteric stabilization plate, 95 degree Dynamic Condylar Screw, first to third generations of gamma nails, proximal femoral nails (PFN), expandable PFN, InterTAN with integrated interlocking screws, proximal femoral locking plates and use of bipolar hemiarthroplasty. This article also aims to present a practical treatment algorithm for the treatment of IT fractures, but this may not be generalizable to all orthopaedic surgeons.
Keywords: Intertrochanteric; unstable; DHS; PFN; Gamma; hemiarthroplasty.
Introduction
Intertrochanteric (IT) fractures are disabling injuries that most commonly affect the elderly population and also in young. The incidence has increased significantly during recent years due to the advancing age of the world’s population. These fractures were managed by conservative methods before 1930s when the age of fixation began. Through this article we wish to present the gradual yet sudden transition in various treatment modalities.
Till the third decade of the twentieth century trochanteric fractures were treated conservatively. Conservative treatment regimes included, simple support with pillows or splinting to the opposite limb, Buck’s (skin) traction, Well-leg traction, plaster spica immobilization, Russell’s balanced traction and skeletal traction through the lower femur or upper tibia. Nonsurgical treatment of intertrochanteric hip fractures is not preferred but is usually reserved for patients with comorbidities who are not fit for anesthesia. Mortality after non-operative treatment is commonly due to cardiopulmonary complications, thromboembolism, and sepsis [1]. In 1989, Hornby et al compared the nonsurgical treatment with a dynamic hip screw (DHS) in 106 patients with intertrochanteric hip fracture [2]. There was no significant difference in complications, 6-month mortality, pain, leg swelling, or pressure sores. SHS group gave better anatomic reduction and a shorter hospital stay. Patients treated conservatively had greater loss of independence at 6-month follow-up. The authors recommended surgical treatment for medically stable patients. A 1981 prospective trial of 150 patients compared nonsurgical treatment (ie, skeletal traction with a tibial pin) with surgical treatment [3]. The authors concluded that excellent results with traction alone could be obtained provided a good nursing care was maintained with careful attention to bedside physical therapy, respiratory care, deep vein thrombosis prophylaxis, and prevention of ulcers. A 2003 retrospective study reviewed a population database to compare mortality rates in patients with severe comorbidities who were treated either nonsurgically or surgically for intertrochanteric hip fracture [4]. It concluded that the mortality rate was low in the conservatively treated patients provided the patients were mobilized early out of bed to chair. The evidence-based literature supports surgical fixation while also providing valuable information in regard to medically unstable patients who must be treated nonsurgically [2-4].
Operative treatment options
Era of Dynamic Hip Screw (DHS)
During the early 1950s when the use of Smith Peterson nail and Jewett nail-plate was very common, W. Schumpelick et al. revolutionized treatment of IT fractures by presenting the results of the sliding neck screw of the DHS in 1955 [5]. Here any force acting on the femoral head in the direction of the body axis will be diverted by the sliding neck screw into the direction of the axis of the screw, so that it strikes the fracture line approximately at a right angle and acts not as a shearing but as a compressing force stimulating callus formation. Here too varus collapse, shortening, superior cut-out occurred. But in non-union was rare.
What is an unstable intertrochanteric fracture?
Stable intertrochanteric fracture implies that the reduction is stable with a lesser tendency to collapse further post-operatively. Whereas the unstable IT fractures have a tendency to collapse much more post-operatively, especially in varus and retroversion. Fractures with a large posteromedial void, reverse oblique fracture configuration, IT fractures with subtrochanteric extension and IT fractures with a lateral wall fracture [6-10].
Modifications of DHS:
Two major modifications to the DHS are the Medoff’s plate and the DHS with a trochanteric stabilisation plate.
In 1991, Medoff et al used a new axial compression screw plate device for unstable intertrochanteric or proximal subtrochanteric fractures of the hip with no technical failures [11]. The device has an axial compression screw to allow compression along an axis parallel to the femoral shaft. As the fracture settles postoperatively, dynamic axial compression continues. In 1993, Babst et al. stated that the lateralisation of the greater trochanter could be prevented in all cases with a trochanteric buttress plate being added to the sliding screw-plate [12]. This also leads to a limitation of telescoping, with less shortening even with immediate full weight bearing. Leung F et al concluded that the DHS blade plate was an effective fixation option in elderly osteoporotic patients with intertrochanteric fracture femur where the conventional lag screw was replaced with a helical blade [13]. Here, the helical blade leads to better blade fixation in osteorotic bone by impaction of the cancellous bone while insertion rather than destroying bone while reaming for the DHS lag screw.
Other conventional options:
95 degree DCS or angle blade plate is often used to treat the reverse oblique intertrochanteric fractures as they biomechanically mimic the subtrochanteric fractures. Rosso R et al recommend that the DCS may be used to treat subtrochanteric fractures rather than intertrochanteric fractures [14].
Era of Intramedullary nails:
Gamma Nail:
This was one of the earliest intra-medullary (IM) imlants to be designed in 1988. The premise on which the IM implants were designed were:
1. To reduce the varus strain on the implant while weight bearing by reducing the force arm.
2. To provide a lateral buttress with an IM device to prevent the lateralization of the proximal fragment and control the collapse rather than relying on the integrity of the lateral wall.
Bridle et al in 1991, prospectively compared the dynamic hip screw and the gamma nail in100 intertrochanteric fractures in elderly patients [15]. They found no difference in the operating time, blood loss, wound complications, and stay in hospital or the patient’s mobility. But fractures of the femur in 4 cases were seen in the gamma nail group which required further revision surgery.
Leung KS et al in 1992conducted a randomized study in elderly patients comparing gamma nails and dynamic hip screws and concluded similar final outcome with both, but achieved less surgical trauma, less screening time, less blood loss and earlier rehabilitation with gamma nails [16].
Radford PJ et al prospectively compared the Dynamic hip screw and the Gamma nail for fixing 200 peritrochanteric femoral fractures in elderly patients [17]. There was less intraoperative blood loss and a lower rate of wound complications in the patients treated by the Gamma nail. They however had a high incidence of femoral shaft fractures which were related to the implant design. They did not recommend the use of the Gamma nail for these fractures. Curtis MJ in 1994 assessed the rigidity and strength of fixation provided by intramedullary and extramedullar devices for proximal femoral fractures [18]. Stable and unstable intertrochanteric fractures were studied after fixation with Gamma nail and DHS implants. There was no significant difference in the strength of fixation of stable and unstable intertrochanteric fractures between the Gamma nail and the hip screw, although the Gamma nail provided more rigid fixation. In 2001, Adams CI et al prospectively compared the IM nailing with a DHS and side plate in 400 patients [19]. Revision rates, femoral shaft fractures, and lag screw cutout were slightly higher in the IM nailing group but not statistically significant from the DHS cohort. There was no difference in the early or 1 –year functional outcomes. Ahrengart L et al randomized 426 intertrochanteric fractures to be fixed with either the Gamma nail or a compression hip screw [20]. The surgical time was not significantly different between the two groups. In the Gamma nail group, difficulty was encountered with the distal locking technique. The incidence of cephalic position of the compression screw within the femoral head, screw cutout, and intraoperative fracture were higher in the Gamma nail group. Walking ability was the same in both groups. The authors recommended compression hip screws for less comminuted fractures, reserving Gamma nails for comminuted patterns.
Utrilla AL et al compared the Gamma nail with a compression hip screw in 210 stable and unstable fractures and found no difference in total surgical time [21]. However, the Gamma nail group had a significantly lower postoperative transfusion requirement. Mortality, fracture healing, and intra- and postoperative complication rates were not significantly different between the two groups. In patients with unstable fracture patterns, postoperative ambulation was significantly improved in the Gamma nail group.
Newer Gamma nails:
The Preference to the use of Gamma nail for unstable IT fractures after early 2000 was primarily due to the introduction of second generation Gamma nail called the Trochanteric Gamma Nail (TGN) and the third generation Gamma nail called the Gamma3 Nail (G3). Better implant design led to decreased fracture shaft femur, which was the complication seen in early generation Gamma Nail [22].
The G3 proximal diameter is 15.5 mm, 1.5 mm smaller than TGN (17 mm). G3 design also allows distal dynamic locking screw. But the migration resistance in G3 is lesser than TGN. The main reason for this is the smaller diameter in the G3 lag screw measuring 10.5 mm rather than 12 mm in the TGN [22].
The latest edition to the G3 design is the Gamma3Rotational Control, with the addition of a spreading U-Clip over the cephalic screw which increases the surface area and also the resistance to failure [22].
Clinical studies report better results with G3. Varela-Egocheaga JR et al reported 2 cases of cutout and 1 screw protrusion in 40 patients (7.5%) in a series comparing G3 with an extramedullary device [23]. Andruszkow H et al reported that a TAD should not exceed 25mm and a valgus reduction reduces the chances of screw cut-out [24]. de Grave PW et al [25] reported 2 cases of mechanical failure in 61 patients treated with a Gamma3 nail, and Westacott D and Bould M [26] reported no case of mechanical failure in 36 unstable proximal femoral fractures treated with a long Gamma3 nail. Mingo-Robinet J et al stated that there was no relationship between cutout rate and TAD in TGN and G3 [22]. Though they concluded that Gamma3 Nail has higher cutout rates than TGN in unstable fractures.
Proximal Femoral Nail
In 1996, AO/ASIF developed the proximal femoral nail (PFN) as an intramedullary device for the treatment of unstable per, inter and subtrochanteric femoral fractures.
Pajarinen J et al compared the DHS with a proximal femoral nail (PFN) in 108 patients and the main outcome measure was recovery of ambulation [27]. The patients treated with IM devices had a significantly faster return to preoperative ambulation levels. Nuber S et al evaluated 129 patients with unstable intertrochanteric fractures treated with either a DHS or a PFN [28]. Revision rates were similar between the two groups. However, there was a significantly shorter surgical time, shorter hospital stay, earlier full weight bearing and lesser pain intensity at 6-months post-op in the PFN cohort. Zhang K et al stated in a meta-analysis of six studies including 669 intertrochanteric fractures that the PFN group had significantly less operative time, intraoperative blood loss and length of incision than the DHS group [29]. There was no significant difference in the postoperative infection rate, lag screw cut-out rate, or reoperation rate between the PFN and DHS groups. They concluded stating that PFN is a better implant than DHS.
Newer PFN designs
PFNA-II is the modified PFN design meant to match the Asian proximal femoral morphometry. Expandable PFN was designed to retain the mechanical characteristics of a large-diameter nail, to provide the good torsional stability between the femoral neck and shaft obtained by an expendable peg inserted in the femoral head (especially in cases of poor bone quality), and to avoid the need for interlocking screws. However its long term utility needs further literature support. Elis J et al concluded that the expandable PFN was at least as good as the 95 degree DCS after comparing the EPFN and the 95 degree DCS [30]. Jin YM et al concluded that expandable PFN are better implants than DHS and anatomic plates in treating intertrochanteric fractures [31].
InterTAN
This is a newer intra-medullary fixation device which uses proximal intergrated interlocking screws in a figure of eight position to attain compression of the intertrochanteric fracture site.
Wang Q et al compared the InterTAN and the DHS and concluded that InterTAN significantly reduces the operative time, intra-operative radiation exposure, intra-operative blood loss and postoperative complications [32]. The InterTAN can be used in elderly osteoporotic patients and in and unstable intertrochanteric fractures.
Jiang Y et al stated that a proper pre-operative imaging, reaming is essential before inserting the InterTAN [33]. But an open reduction and internal fixation with DHS be preferred in cases where the reduction is difficult.
Nüchtern JV et al concluded that the InterTAN with two integrated screws was able to withstand higher loads than the Gamma 3 nail [34].
Newer Proximal femoral Locking plates:
Many new designs of proximal femoral locking plates have been used to treat intertrochanteric fractures. But there is not enough literature evidence of they being better than IM implants. Haq RU et al concluded that PFN is a better implant than reverse-distal femoral locking plate for intertrochanteric fractures with a deficient lateral wall [35]. Zhong B et al stated that the proximal femoral locking plates were better for treating subtrochanteric fractures rather than intertrochanteric fractures [36].
Azboy I et al concluded that both proximal femoral locking plate and 95 degree angle blade plate gave equally good results in reverse oblique intertrochanteric fractures. However, angle blade plates were preferred as they were an economical option [37].
Dhamangaonkar AC et al compared the Proximal femoral locking plate with the DHS. They concluded that proximal femoral locking plates decreased the chances of limb shortening and medialisation of the shaft [38].
A recent study by Shen J et al concluded that these plates are an effective and safe method in the treatment of all types of intertrochanteric femoral fractures, but good fracture reduction and ideal positioning of the neck screw are prerequisites for the success of the device [39].
Hemiarthroplasty
Prosthetic hip replacement generally has not been considered a primary treatment option for intertrochanteric fractures. In this setting, prosthetic replacement for intertrochanteric fractures typically requires a more complex surgical procedure to reconstruct the calcar and trochanters with potentially higher morbidity. In the patient with preexisting symptomatic degenerative arthritis and in extremely comminuted osteoporotic intertrochanteric fractures, primary prosthetic replacement may be a better option [40].
Kim Y et al studied 143 hips in 139 octagenarians who underwent a cementless bipolar hemiarthroplasty for intertrochanteric fractures concluded that cementless bipolar hemiarthroplasty appears to be a suitable method for the treatment of intertrochanteric fracture in octogenarians [41]. And recommended that stable fixation of the posteromedial fragment is necessary to avoid stem subsidence. Emami M et al studied 60 patients with IT fractures, compared bipolar hemiarthroplasty and DHS fixation and concluded that in elderly patients with co-morbidities, bipolar hemiarthroplasty was more effective than DHS with better functional status, however there was no difference in pain severity between the two groups [42]. Cankaya D et al compared the functional outcome of cementless versus cemented hemiarthroplasty in 86 elderly patients and concluded that cementless hemiarthroplasty was better in terms of duration of surgery, amount of blood loss and perioperative mortality rates than in the cemented group [43]. But Shen J et al categorically stated after studying 124 patients above 70 years of age, that Internal fixation is preferred as it leads to a higher Harris scores, lesser pain, and better walking ability than those treated with hemiarthroplasty provided there is good and stable reduction, even when severe osteoporosis is present [44]. Tang P et al, after retrospectively studying 303 patients concluded that PFNA was superior to hemiarthroplasty according to the operative statistics, especially the anaesthesia, operation lasting time, blood loss, blood transfusion and the drainage, but there were no significant differences in functional outcome [45]. But the incidences of complications were higher in hemiarthroplasty group. Hemiarthroplasty may still find favor in cases with fracture comminution in elderly with severe osteoporosis or in cases with failed fixation of intertrochanteric fracture [46]. More definative evidence will be needed to stratify the patients who would be benefitted by hemiarthroplasty.
Treatment Algorithm
The American Academy of Orthopaedic Surgeons (AAOS) presented a Clinical Practice Guidelines (CPG) on the management of hip fractures after reviewing above16,000 abstracts and above 1700 full-text articles and came out with 25 evidence-based recommendations. We present here a summary of the same [47].
Apart from the operative decision, the recommendations do suggest important practices like avoiding delays to surgery, decreasing delirium, initiate postoperative physical therapy, nutritional, calcium and vitamin D supplementation and evaluation of osteoporosis.
The next important determinant affecting the operative plan, is the IT fracture configuration- whether stable or unstable. There is equal evidence for the use of either intramedullary implants or sliding hip screws in the treatment of stable intertrochanteric fractures. Though the newer generation orthopaedic surgeonsprefer the use of IM implants due to its percutaneous insertion, lesser operative time and blood loss. Though, the cost of implant, comfort and training of the surgeon determines the choice of implants.
There a strong recommendation to use the IM implants for the unstable IT fractures, especially the ones with a subtrochanteric extension and reverse oblique fracture configuration. There is however not enough literature to suggest use of short or long IM implants and further studies are required to determine the outcome of each.
Clinical Relevance
The most important determinant of treatment of IT fractures is whether the fracture is stable or unstable and advantages of the newer implant designs available to treat IT fractures. Stable fractures may be fixed with either intra-medullary or extra-medullary implants. The treatment of unstable IT fractures needs meticulous pre-operative planning, good intra-operative reduction and use of intra-medullary implants. The surgeon is free to use any design amongst the many intra-medullary implants as per the training and experience of the surgeon. There is as yet no consensus in literature regarding whether to use short or long IM nails. As far as possible fixation of IT fractures is to be attempted rather than a hemiarthroplasty.
References
1. Parker MJ, Handoll HH: Conservative versus operative treatment for extracapsular hip fractures. Cochrane Database Syst Rev 2000; 2: CD000337.
2. Hornby R, Evans JG, Vardon V: Operative or conservative treatment for trochanteric fractures of the femur: A randomized epidemiological trial in elderly patients. J Bone Joint Surg Br 1989; 71:619-623.
3. Bong SC, Lau HK, Leong JC, Fang D, Lau MT: The treatment of unstable intertrochanteric fractures of the hip: A prospective trial of 150 cases. Injury 1981; 13:139-146.
4. Jain R, Basinski A, Kreder HJ: Nonoperative treatment of hip fractures. Int Orthop 2003; 27:11-17.
5. Schumpelick W, Jantzen PM. A new principle in the operative treatment of trochanteric fractures of the femur. J. Bone Joint Surg. Am. 1955; 37; 693-698.
6. Aktselis I, Papadimas D, Fragkomichalos E, et al.. Intramedullary nailing of trochanteric fractures–operative technical tips. Injury. 2012;43:961–965.
7. Haidukewych GJ, Israel TA, Berry DJ. Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am. 2001;83-A:643–650.
8. Sims SH. Subtrochanteric femur fractures. Orthop Clin North Am. 2002;33:113–126
9. Gotfried Y. The lateral trochanteric wall: a key element in the reconstruction of unstable pertrochanteric hip fractures. Clin Orthop Relat Res. 2004;425:82–86.
10. Palm H, Jacobsen S, Sonne-Holm S, et al.; Hip Fracture Study Group. Integrity of the lateral femoral wall in intertrochanteric hip fractures: an important predictor of a reoperation. J Bone Joint Surg Am. 2007;89:470–475.
11. Medoff RJ, Maes K. A new device for the fixation of unstable pertrochanteric fractures of the hip. JBoneJoint Surg Am. 1991;73:1192-1199.
12. Babst R et al. The DHS (dynamic hip screw) buttress plate in the management of unstable proximal femoral fractures. Schweiz Med Wochenschr. 1993;123:566-568.
13. Leung F , Gudushauri P, Yuen G, Lau TW, Fang C, Chow SP. Dynamic hip screw blade fixation for intertrochanteric hip fractures. J Orthop Surg (Hong Kong). 2012;20:302-306.
14. Rosso R , Babst R, Marx A, Hess P, Heberer M, Regazzoni P. Proximal femoral fractures. Is there an indication for the condylar screw (DCS)?. Helv Chir Acta. 1992;58:679-82.
15. Bridle SH, Patel AD, Bircher M, Calvert PT . Fixation of intertrochanteric fractures of the femur. A randomised prospective comparison of the gamma nail and the dynamic hip screw. J Bone Joint Surg Br. 1991;73:330-334.
16. LeungKS , So WS, Shen WY, Hui PW. Gamma nails and dynamic hip screws for peritrochanteric fractures. A randomised prospective study in elderly patients. J Bone Joint Surg Br. 1992;74:345-351.
17. Radford PJ, Needoff M, Webb JK. A prospective prolonged comparison of the Dynamic hip screw and the Gamma locking nail. J Bone Joint Surg 1993; 75 : 789-793.
18. Curtis MJ, Jinnah RH, Wilson V. Proximal femoral fractures: A biomechanical study to compare intramedullary and extramedullar/ fixation. J Bone Joint Surg 1994; 25 :99-104.
19. Adams CI, Robinson CM, Court-Brown CM, McQueen MM: Prospective randomized controlled trial of an intramedullary nail versus dynamic screw and plate for intertrochanteric fractures of the femur. J Orthop Trauma 2001; 15:394-400.
20. Ahrengart L, Törnkvist H, Fornander P, et al.: A randomized study of the compression hip screw and Gamma nail in 426 fractures. Clin Orthop Relat Res 2002; 401:209-222.
21. Utrilla AL, Reig JS, Muñoz FM, Tufanisco CB: Trochanteric gamma nail and compression hip screw for trochanteric fractures: A randomized, prospective, comparative study in 210 elderly patients with a new design of the gamma nail. J Orthop Trauma 2005; 19:229-233.
22. Mingo-Robinet J, Torres-Torres M, Martínez-Cervell C, Alonso Del Olmo JA, Rivas Laso JA, Aguado-Hernández Het al. Comparative study of the second and third generation of gamma nail for trochanteric fractures: review of 218 cases. J Orthop Trauma. 2015;29:e85-90.
23. Varela-Egocheaga JR, Iglesias-Colao R, Suarez-Suarez MA, et al.. Minimally invasive osteosynthesis in stable trochanteric fractures: a comparative study between Gotfried percutaneous compression plate and Gamma3 intramedullary nail. Arch Orthop Trauma Surg. 2009;129:1401–1407.
24. Andruszkow H, Frink M, Frömke C, et al.. Tip apex distance, hip screw placement, and neck shaft angle as potential risk factors for cut-out failure of hip screws after surgical treatment of intertrochanteric fractures. Int Orthop. 2012;36:2347–2354.
25. de Grave PW, Tampere T, Byn P, et al.. Intramedullary fixation of intertrochanteric hip fractures: a comparison of two implant designs. A prospective randomised clinical trial. Acta Orthop Belg. 2012;78:192–198.
26. Westacott D, Bould M. Outcome in 36 elderly patients treated with the Gamma3 Long Nail for unstable proximal femoral fracture. Acta Orthop Belg. 2011;77:68–72.
27. Pajarinen J, Lindahl J, Michelsson O, Savolainen V, Hirvensalo E: Pertrochanteric femoral fractures treated with a dynamic hip screw or a proximal femoral nail: A randomised study comparing post-operative rehabilitation. J Bone Joint Surg Br 2005; 87:76-81.
28. Nuber S, Schönweiss T, Rüter A: Stabilisation of unstable trochanteric femoral fractures: Dynamic hip screw (DHS) with trochanteric stabilisation plate vs. proximal femur nail (PFN) [German]. Unfallchirurg 2003; 106:39-47.
29. Zhang K, Zhang S, Yang J, Dong W, Wang S, Cheng Y et al. Proximal femoral nail vs. dynamic hip screw in treatment of intertrochanteric fractures: a meta-analysis. Med Sci Monit. 2014;20:1628-33.
30. Elis J, Chechik O, Maman E, Steinberg EL. Expandable proximal femoral nails versus 95° dynamic condylar screw-plates for the treatment of reverse oblique intertrochanteric fractures. Injury. 2012;43:1313-1317.
31. Jin YM , Chen JP, Li XL, Huang YZ, Yang D. [Retrospective study of comparing the different internal fixation methods in treating intertrochanteric fracture of femur]. Zhongguo Gu Shang. 2008;21:329-332.
32. Wang Q , Yang X, He HZ, Dong LJ, Huang DG. Comparative study of InterTAN and Dynamic Hip Screw in treatment of femoral intertrochanteric injury and wound. Int J Clin Exp Med. 2014;7:5578-5582.
33. Jiang Y, Li J, Dib HH, Li YC.Implantation of INTERTAN™ nail in four patients with intertrochanteric fractures leading to single or comminute fractures: pitfalls and recommendations: a case series. J Med Case Rep. 2014;8:383.
34. Nüchtern JV, Ruecker AH, Sellenschloh K, Rupprecht M, Püschel K, Rueger JM et al. Malpositioning of the lag screws by 1- or 2-screw nailing systems for pertrochanteric femoral fractures: a biomechanical comparison of gamma 3 and intertan. J Orthop Trauma. 2014;28:276-282.
35. Haq RU , Manhas V, Pankaj A, Srivastava A, Dhammi IK, Jain AK. Proximal femoral nails compared with reverse distal femoral locking plates in intertrochanteric fractures with a compromised lateral wall; a randomised controlled trial. Int Orthop. 2014;38:1443-1449.
36. Zhong B , Zhang Y, Zhang C, Luo CF. A comparison of proximal femoral locking compression plates with dynamic hip screws in extracapsular femoral fractures. Orthop Traumatol Surg Res. 2014;100:663-668.
37. Azboy I, Demirtaş A, Gem M, Cakır IA, Tutak Y. A comparison of proximal femoral locking plate versus 95-degree angled blade plate in the treatment of reverse intertrochanteric fractures. Eklem Hastalik Cerrahisi. 2014;25:15-20.
38. Dhamangaonkar AC, Joshi D, Goregaonkar AB, Tawari AA. Proximal femoral locking plate versus dynamic hip screw for unstable intertrochanteric femoral fractures. J Orthop Surg (Hong Kong). 2013;21:317-322.
39. Shen J, Luo F, Sun D, Huang Q1, Xu J, Dong S et al. Mid-term results after treatment of intertrochanteric femoral fractures with percutaneous compression plate (PCCP). Injury. 2015;46:347-357.
40. Parker MJ, Handoll HH: Replacement arthroplasty versus internal fixation for extracapsular hip fractures. Cochrane Database Syst Rev 2000; :CD000086.
41. Kim Y, Moon JK, Hwang KT, Choi IY, Kim YH. Cementless bipolar hemiarthroplasty for unstable intertrochanteric fractures in octogenarians. Acta Orthop Traumatol Turc. 2014;48:424-430.
42. Emami M , Manafi A, Hashemi B, Nemati A, Safari S. Comparison of intertrochanteric fracture fixation with dynamic hip screw and bipolar hemiarthroplasty techniques. Arch Bone Jt Surg. 2013;1:14-17.
43. Cankaya D, Ozkurt B, Tabak AY. Cemented calcar replacement versus cementless hemiarthroplasty for unstable intertrochanteric femur fractures in the elderly. Ulus Travma Acil Cerrahi Derg. 2013;19:548-553.
44. Shen J, Wang DL, Chen GX, Yang HL, Li L, Wei MX et al. Bipolar hemiarthroplasty compared with internal fixation for unstable intertrochanteric fractures in elderly patients. J Orthop Sci. 2012;17:722-729.
45. Tang P, Hu F, Shen J, Zhang L, Zhang L. Proximal femoral nail antirotation versus hemiarthroplasty: a study for the treatment of intertrochanteric fractures. Injury. 2012;43:876-881.
46. Sancheti Kh, Sancheti P, Shyam A, Patil S, Dhariwal Q, Joshi R. Primary hemiarthroplasty for unstable osteoporotic intertrochanteric fractures in the elderly: A retrospective case series. Indian J Orthop. 2010 Oct;44(4):428-34
47. Roberts KC, Brox WT.From Evidence to Application: AAOS Clinical Practice Guideline on Management of Hip Fractures in the Elderly. J Orthop Trauma. 2015;29:119-120.
(Abstract) (Full Text HTML) (Download PDF)
Classifications of Intertrochanteric fractures and their Clinical Importance
/in July Sep | Volume 1 | Issue 1Vol 1 | Issue 1 | July – Sep 2015 | page: 7-11 | Dhiraj V Sonawane[1].
Author: Dhiraj V Sonawane[1].
[1] Grant Medical College and Sir JJ Group of Hospitals, Mumbai. India.
Address of Correspondence
Dr. Dhiraj V. Sonawane
Asst. Prof. Grant Medical College and Sir JJ Group of Hospitals, Mumbai.
Email: dvsortho@gmail.com
Abstract
Intertrochanteric fractures are one of the most common fractures encountered by an orthopaedic Surgeon. Many attempts to classify these fractures are made and different scientific rationale are applied by various authors. Here we tried to provide an overview of both old and new classification of intertrochanteric fractures and also provide with the clinical significance of the same
Keywords: intertrochanteric fractures, hip fractures, classifications
Introduction
Intertrochanteric (IT) fractures are most common fractures seen in elderly osteoporotic, usually due to simple fall in the house. With increasing number of elderly patients its number is estimated to be double by 2040 [1]. Understanding important factors in management of IT fracture like stability, reduction, role of posteriomedial wall, lateral wall, will help in choosing implant for better outcome. Most classifications are based on these factors and help in selecting management protocols. Many classification systems have come from last 6 decades, but none of them are found to be unanimously acceptable worldwide. Few classifications have focussed on stability and anatomical pattern (Evans; Ramadier; Decoulx; & Lavarde) while others on maintaining reduction of various types (Jensen’s modification of Evan’s, Ender; Tronzo, AO).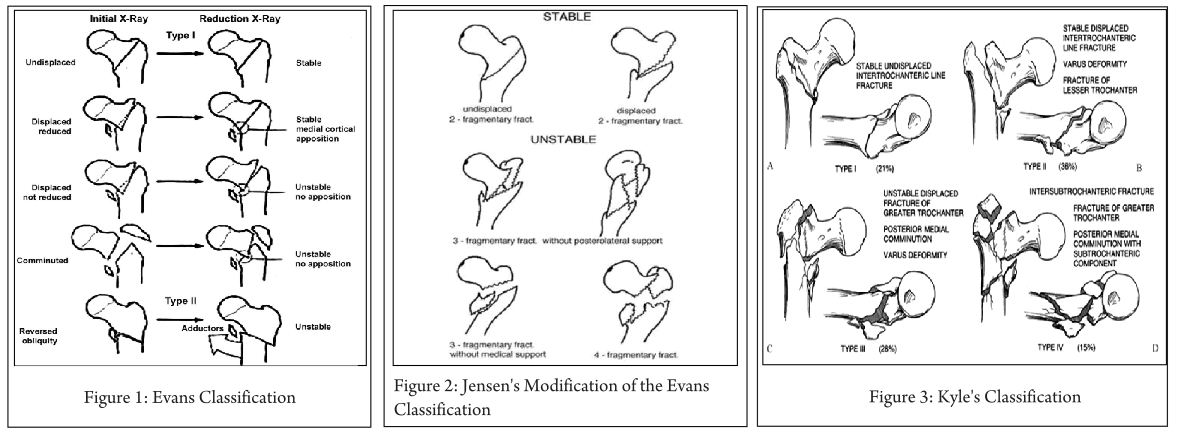
An ideal classification should be simple, reproducible, easy to apply and should provide information on stability after reduction, secondary displacement, technique of fixation, postoperative mobilisation, outcome, and also data organisation for research. It should have good interrater and intrarater reliability and validity.
Classification Review:
Various classifications in Intertrochanteric fractures:
Evans Classification [2] (Fig 1):
In 1949, Evans published his classification on intertrochanteric (IT) fractures as follows:
Type I:
Stable:
-Undisplaced fractures.
-Displaced but after reduction overlap of the medial cortical buttress make the fracture stable.
Unstable:
-Displaced and the medial cortical buttress is not restored by reduction of fracture.
-Displaced and comminuted fractures in which the medial cortical buttress is not restored by reduction of the fracture.
Type II: Reverse obliquity fractures.
Clinical importance: This helped in better understanding of intertrochanteric fractures based on stability of fracture after close reduction and skeletal traction. According to Evans, posterior-medial cortex continuation is important for restoring stability of IT fractures. Based on this he classified IT fractures into Stable and Unstable fractures. Stable fractures have intact or minimally communited posteriomedial cortex, while Unstable fracture has greater communition of posteriomedial cortex. Unstable fractures after reduction can be converted to stable fracture if the posteriomedial cortex opposition can be achieved. Reverse oblique pattern was considered inheritably unstable fracture as distal femur has tendency to drift medially due adductor pull.
Jensen’s Modification of the Evans Classification [3] (Fig. 2):
Jansen (1975 ) later modified Evans classification into three groups.
Displaced or undisplaced stable 2-fragment fractures, Unstable 3-fragment fractures with greater or lesser trochanter fracture and 4-fragment fractures
Clinical Importance: the classification reduced the number of types from 6 to 5 by including the extremely rare fracture with a reversed oblique fracture line and large greater trochanter fragment into Type 3. Modification of the Evans system offers the best prediction of the possibility of obtaining reliable anatomical reduction and the risk of secondary fracture dislocation.
Kyle’s Classification [4] (Fig. 3):
Type I fractures consist of nondisplaced stable intertrochanteric fractures without comminution.
Type II fractures represent stable, minimally comminuted but displaced fractures; these are the fractures that, once reduced, allow a stable construct. Stable fractures are not a problem and hold up well with any type of fixation device.
Type III intertrochanteric fracture is a problem fracture and has a large posteromedial comminuted area.
Type IV fracture is uncommon and consists of an intertrochanteric fracture with a subtrochanteric component. This is the most difficult type of fracture to fix because of the great forces imposed by muscle forces and weight bearing on the subtrochanteric region of the femur.
Clinical Importance: Addition of new variant (type 4) extension of intertrochanteric fracture in neck.
AO/ Orthopaedic Trauma Association (OTA) Alphanumeric Classification [5] (1980-1987) (Fig. 4):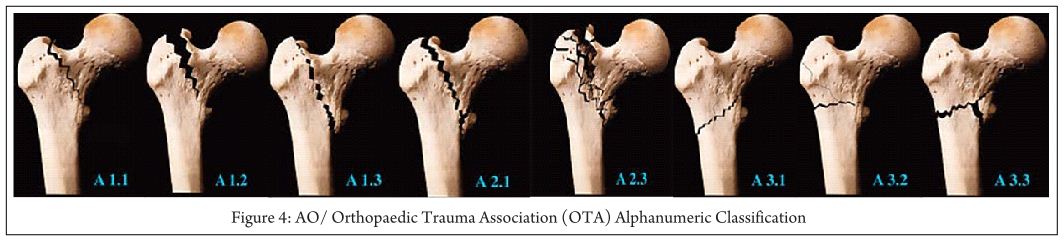
In the Comprehensive Classification of Fractures of the Long Bones, Müller and colleagues coded proximal hip fractures to offer a uniform alphanumeric fracture classification. This system was advocated by the AO/ASIF, and later adopted by OTA in their Fracture Compendium.
According to AO/OTA alphanumeric classification intertrochanteric fractures (Type 31A) Bone = femur = 3,Segment = proximal = 1,Type = A1, A2, A3 A1: simple (two-part) fractures, with the typical oblique fracture line extending from the greater trochanter to the medial cortex; the lateral cortex of the greater trochanter remains intact.
A2: fractures are comminuted with a posteromedial fragment; the lateral cortex of the greater trochanter, however, remains intact. Fractures in this group are generally unstable, depending on the size of the medial fragment
A3: fractures are those in which the fracture line extends across both the medial and lateral cortices; this group includes the reverse obliquity pattern or subtrochanteric extensions.
31-A Femur, proximal trochanteric
31-A1 Peritrochanteric simple
31-A1.1 Along intertrochanteric line
31-A1.2 Through greater trochanter
31-A1.3 Below lesser trochanter
31-A2 Peritrochanteric multifragmentary
31-A2.1 With one intermediate fragment
31-A2.2 With several intermediate fragments
31-A2.3 Extending more than 1 cm below lesser trochanter
31-A3 Intertrochanteric
31-A3.1 Simple oblique
31-A3.2 Simple transverse
31-A3.3 Multifragmentary.
Clinical importance: This helps in predicting prognosis and suggests treatment for the entire spectrum of IT fractures. Fractures A1.1 through A2.1 are commonly described as stable, and fractures A2.2 through A3.3 usually are unstable.
Generally, the Evans-Jensen type I fracture is represented by the 31-A1 group. Evans-Jensen type II fractures are in the 31-A2 group. The so-called reverse obliquity intertrochanteric fracture is in group 31-A3. It’s alphanumeric and standardized format make this system useful, particularly for research and documentation.
Boyd and Griffin Classification (1949) [6] (Fig. 5):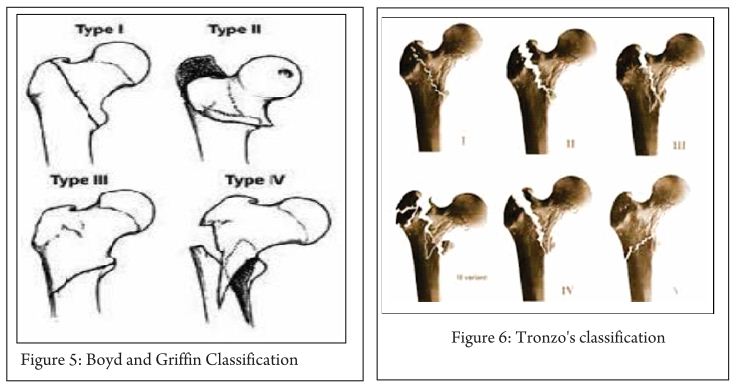
They were first to mention instability in both coronal and sagittal plane. This classification, included fractures from the extracapsular part of the neck to a point 5 cm distal to the lesser trochanter.
Type 1: Fractures that extend along the intertrochanteric line.
Type 2: Comminuted fractures with the main fracture line along the intertrochanteric line but with multiple secondary fracture lines (may be in coronal plane).
Type 3: Fractures that extend to or are distal to the lesser trochanter.
Type 4: Fractures of the trochanteric region and proximal shaft with fractures in at least two planes.
Clinical importance:
Type 1- Reduction usually is simple and is maintained with little difficulty. Results generally are satisfactory
Type 2- Reduction of these fractures is more difficult because the comminution can vary from slight to extreme
Type 3- these fractures usually are more difficult to reduce and result in more complications at operation and during convalescence.
Type 4- if open reduction and internal fixation are used, two-plane fixation is required because of the spiral, oblique, or butterfly fracture of the shaft.
Tronzo’s classification [7] (1973) (Fig. 6):
Tronzo incorporated Boyds and Griffin two plane instability in classification.
Type 1: Incomplete fractures
Type 2: Uncomminuted fractures, with or without displacement; both trochanters fractured
Type 3: Comminuted fractures, large lesser trochanter fragment; posterior wall exploded; neck beak impacted in shaft
Type 3 Variant: As above, plus greater trochanter fractured off and separated
Type 4: Posterior wall exploded, neck spike displaced outside shaft
Type 5: reverse obliquity fracture, with or without greater trochanter separation
Clinical importance:
This system is complex to use & not adequate to apply in clinical practice. It has poor reliability, though can be used for documentation of long-term results and comparison of treatment modality. Yet many surgeons prefer it for its simplicity and biomechanical rationale.
The Ramadier’s Classification[8](Fig. 7):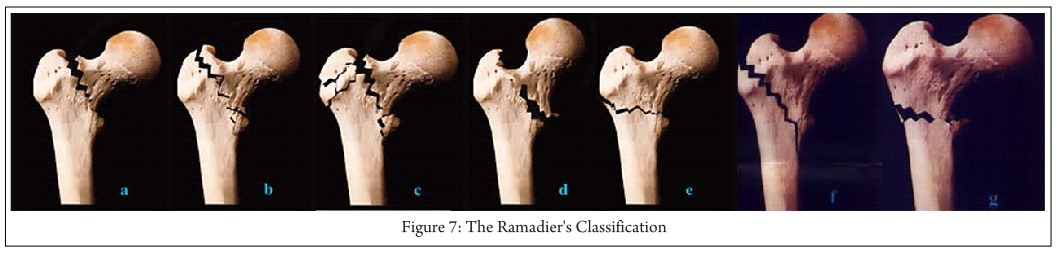
A: Cervico-trochanteric fractures- with a fracture line at the base of the femoral neck
b: Simple pertrochanteric fractures- fracture line that runs parallel to the intertrochanteric line; frequently, the lesser trochanter is broken off
c: Complex pertrochanteric fractures have an additional fracture line that separates most of the greater trochanter from the femoral shaft; the lesser trochanter is often fractured
d: Pertrochanteric fractures with valgus displacement- fracture line that begins on the greater trochanter and finishes below the lesser trochante
e: Pertrochanteric fractures with an intertrochanteric fracture line
f: Trochantero-diaphyseal fractures- spiral line through the greater trochanter and into the proximal shaft often with 3rd fragment.
G: Subtrochanteric fractures- more or less horizontal fracture line that runs below the two trochanters
Decoulx and Lavarde’s classification [9](1969):Simple anatomical classification for descriptive purposes.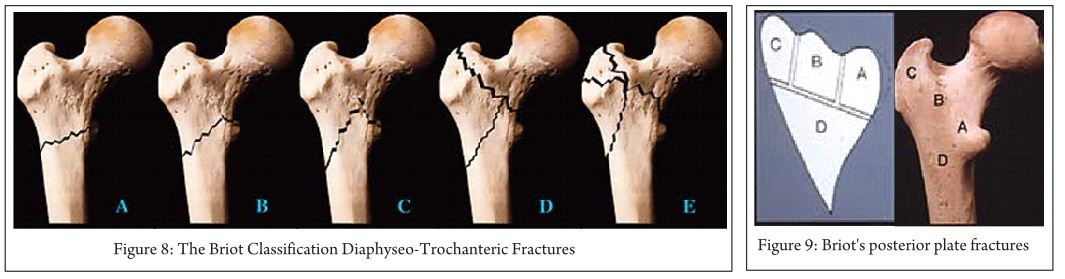
Cervico-trochanteric fractures
Pertrochanteric fractures
Intertrochanteric fractures
Subtrochanteric fractures
Subtrochantero-diaphyseal fractures
The Briot Classification Diaphyseo-Trochanteric Fractures [10] (1980) (Fig. 8):
A Evans’ reversed obliquity fracture
B “Basque roof” fractures
C Boyd’s “steeple” fracture
D Fractures with an additional fracture line ascending to the intertrochanteric line
E Fractures with additional fracture lines radiating through the greater trochanter
Briot’s posterior plate fractures
Note: Boundaries of posterior plate, Maximum extent of plate, Possible fracture lines
Clinical importance: Its simple and based on biomechanical concept. Briot’s found posterior wall fracture is important for sagittal instability and external rotation sometimes causing malunion in external rotation. Reduction can be done in these by internal rotation reducing the anterior gap while realign the posterior fractured wall.
Ender Classification(1970)[11] (Fig. 10):
Trochanteric eversion fractures
-1. Simple fractures
-2. Fractures with a posterior fragment
-3 Fractures with lateral and proximal displacement
3. trochanteric inversion fractures
-4. With a pointed proximal fragment spike
-5 .With a rounded proximal fragment beak
6. Intertrochanteric fractures
Subtrochanteric fractures
-7 and 7a Transverse or reversed obliquity fractures
-8 and 8a Spiral fractures
Clinical importance: This classification gives information on injury mechanism, which can be helpful to reduce fracture while performing closed nailing.
Dr G. S. Kulkarni et al Classification / Modified Jenson-Evan’s Classification[1] (Fig 11):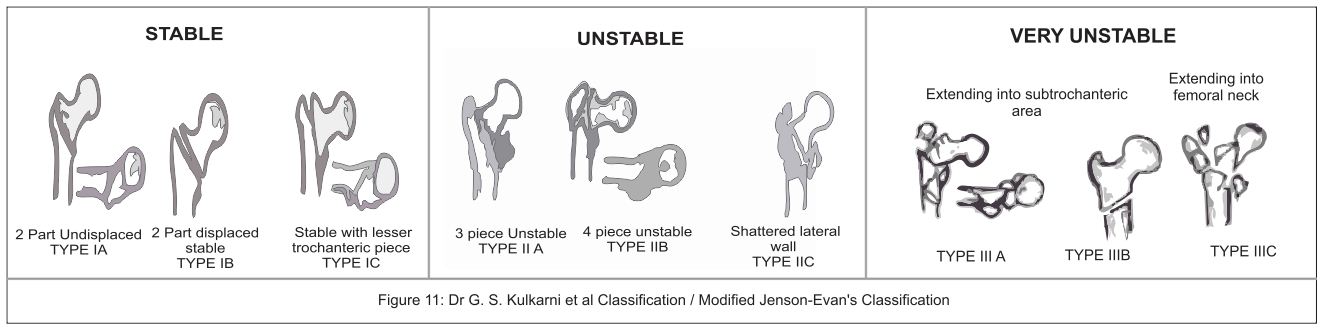
Dr G.S. Kulkarni et al [1] published his new classification in intertrochanteric fractures based on AO & Evan-Jansen classification. He added new varieties of intertrochanteric fractures described by Gotfried[12] and Kyle [4]. This classification is treatment oriented and will help in deciding the implant according to the fracture type.
Type IA- stable undisplaced.
Type IB- stable minimally displaced.
Type IC- stable minimally displaced with a small fragment of lesser trochanter.
Type IIA- unstable 3 piece fracture with large posteromedial fragment of lesser trochanter.
Type IIB- 4 piece fracture.
Type C- Shattered lateral wall.
Type IIIA- trochanteric fracture with extension into subtrochanter.
Type IIIB- reserve oblique.
Type IIIC- trochanteric fracture with extension into femoral neck area.
Clinical Importance: Classification helps in selecting treatment protocols as below.
Type I: This stable fractures can be managed by any fixation modality gives excellent results. DHS is implant of choice.
Type II: These unstable fractures are described as problem fractures can be managed with DHS with some modification or IMN.
Type III: This very unstable fracture with DHS gives poor results. In these type with lateral wall fracture use of DHS lead to excessive collapse, pain, restricted mobility in hip, sometime non union and failure. Intramedullary nails (IMN) are better choice as they prevents excessive collapse at fracture site, better restoration of anatomy and biomechanically stronger implants; Arthroplasty can also be done in select cases. Unusual fracture pattern like basi-cervical fractures extension can be fixed with additional derotation screw as these are also rotationally unstable. Reverse oblique pattern like fracture lateral wall are better fixed with IMN.
Conclusion:
Various classifications have been proposed over years described the fracture patterns, focusing on importance of posteriomedial and lateral wall for stability. Tronzo classification is found to be less reliable and not useful in clinical practice. AO/OTA and Dr G.S. Kulkarni et al modified classification has described in detail the preferred implant according to the fracture type. An AO/OTA group has good reliability but subgroup assessment has poor reliability; it is more useful in record keeping, deciding management and research. Kulkarni et al classification is found to be more simple & easy to apply in practice, record keeping and research. There is still no consensus on the best classification but with new biomechanical informations coming through, the classification systems would continue to evolve.
References
1. GS Kulkarni, Rajiv Limaye, Milind Kulkarni, Sunil Kulkarni. Current Concept review: Intertrochanteric fractures. Indian Journal of Orthopaedics.2006;40:16-23.
2. Evans, E. M. () The treatment of trochanteric fractures of the femur. J. Bone Jt Surg. 1949;31-B: 190-203.
3. Jensen J. S. Classification of trochanteric fractures. Actaorthop. Scand. 1980; 51:803-810.
4. Kyle R. F., Gustilo R. B. And Premer R. F. Analysis of six hundred and twenty-two intertrochantenc hip fractures. J. Bone joint(Am). 1979;61: 216-21.
5. M.E. Muller, S. Nazarian, P. Koch, J. Schatzker The comprehensive classification of fractures of long bones Springer, Berlin. 1990.
6. Boyd HB, Griffin LL. Classification and treatment of trochanteric fractures. Arch Surg. 1949; 58:853.
7. Tronzo RG. Symposium on fractures of the hip. Special considerations in management. Orthop Clin North Am. 1974; 5(3): 571–583.
8. M. Bombart, J.O. Ramadier Trochanteric fractures Rev Chir Orthop, 52 (1966), 353–374.
9. Decoulx P, Lavarde G. Fractures of the trochanteric region. A statistical study of 2,612 cases. J Chir (Paris). 1969; 98(1):75-100.
10. Briot B. Fractures per-trochantériennes: anatomie pathologique et classification. Cahiers d’Enseignement de la SOFCOT Expansions Sci Franc.1980;12: 69-76.
11. J. Ender Per- und subtrochantere Oberschenkelbrüche. Hefte Unfallheilk;1970:106, 2–11.
12. Gotfried Y. The lateral trochanteric wall. Clin Orthop. 2004; 425:.82-86.
(Abstract) (Full Text HTML) (Download PDF)